

Abstract
In several clinical situations, including resection of malignant or benign biliary lesions, reconstruction of the biliary system using the Roux-en-Y jejunum limb has been adopted as the standard procedure. The basic technique and the procedural knowledge essential for most gastroenterological surgeons are described in this article, along with a video supplement. Low complication rates involving anastomotic insufficiency or stricture can be achieved by using proper surgical techniques, even following small bile duct reconstruction. Using the ropeway method to stabilize the bile duct and jejunal limb allows precise mucosa-to-mucosa anastomosis with interrupted sutures of the posterior row of the anastomosis. Placement of a transanastomotic stent tube is the second step. The final step involves suturing the anterior row of the anastomosis. In contrast to the lower extrahepatic bile duct, the wall of the hilar or intrahepatic bile duct can be recognized within the fibrous connective tissue in the Glissonean pedicle. The portal side of the duct should be selected for the posterior wall during anastomosis owing to its thickness. Meticulous inspection to avoid overlooking small bile ducts could decrease the chance of postoperative intractable bile leakage. In reconstruction of small or fragile branches, a transanastomotic stent tube could work as an anchor for the anastomosis.
Electronic supplementary material
The online version of this article (doi:10.1007/s00534-011-0475-5) contains supplementary material, which is available to authorized users.
Keywords: Biliary reconstruction, Bilioenteric anastomosis, Choledochojejunostomy, Hepaticojejunostomy, Hepatobiliary resection
Introduction
Biliary reconstruction is required in several clinical situations, including resection of biliary malignancies, benign biliary strictures, intraoperative injury, and liver transplantation. Bilioenteric anastomosis using the Roux-en-Y jejunum limb is a well-established approach [1–4], especially in reconstruction of the biliary system after the resection of biliary malignancies. Reconstruction using the jejunum allows for safe and permissive anastomosis with infrequent postoperative bile leakage even when the anastomoses involve small intrahepatic branches [5, 6]. However, when biliary complications do occur following major hepatobiliary surgery, including liver transplantation, they can significantly impact the postoperative course [7–9]. Regarding iatrogenic bile duct injury during laparoscopic cholecystectomy, salvage surgery of the biliary system occasionally requires hepaticojejunostomy [10, 11]. Thus, fundamental techniques of bilioenteric anastomosis might be essential for not only hepatobiliary but also gastrointestinal or general surgeons [12].
In this article, we describe techniques of biliary anastomosis involving the jejunum and demonstrate the hepaticojejunostomy following right hepatectomy with caudate lobectomy (segmentectomy 1) using video supplement as routinely performed in the Department of Surgical Oncology, Hokkaido University Graduate School of Medicine.
Operative technique
Division of the bile duct(s)
Division of the middle or superior part of the extrahepatic bile duct
In most pancreatoduodenectomy cases, the bile duct is divided at the middle or superior part of the extrahepatic bile duct. In encircling the bile duct, it is important not to injure the right hepatic artery running just beneath the duct. Before dividing the bile duct, its duodenal side is simply ligated or closed with continuous suture, meanwhile the hepatic side should be occluded with a Bulldog-type vessel clamp. Electric cautery is used to divide the duct while coagulating the bleeding from the ductal wall. When intraoperative frozen section diagnosis is necessitated, division of the duct should be performed utilizing a surgical blade or scissors so as to preserve the surgical margin from heat damage caused by electric cautery. The clamp may be released just before starting the bilioenteric anastomosis to prevent contaminating the operative field with bile juice.
Division of the hilar or intrahepatic bile duct
During the resection of the hilar or intrahepatic ducts, the orifice of the bile duct is revealed by dividing the fibrous connective tissue after removing the portal and arterial tributaries from the Glissonean pedicle [13] (Fig. 1). To avoid missing the ducts, a stay suture with atraumatic needle should be placed in the stump of each duct immediately at the time of detection. The suture has to be positioned in the estimated anterior wall of the anastomosis because it is used for preserving the intraluminal space by lifting it up in suturing of the anterior wall. After coagulating the bleeding from the bile duct wall, careful inspection is again necessary to avoid overlooking tiny branches of the bile ducts such as those arising from the caudate lobe, segment 4, or segment 5, which joins the hilar bile duct (Fig. 1); failure to do this can result in intractable postoperative bile leakage. With the appearance of smaller branches into which 5-French stent tubes cannot be inserted, anastomosis should be abandoned and the orifice closed with sufficient sutures. In patients with poor hepatic reserves, even small branches ought to be reconstructed by utilizing smaller tubes such as a part of disposable intravenous catheters.
Fig. 1.

Intraoperative view following resection of the extrahepatic bile duct with hilar plate. During the resection of the hilar bile duct, the ductal wall can be recognized within fibrous connective tissue after mobilizing the portal vein and hepatic arteries in the Glissonean pedicle. Arrows indicate the ducts (B4′, B1l, B5′) that are liable to be overlooked
Anastomotic technique
Basic procedure of the anastomosis
Two neighboring duct orifices can be joined by two interrupted stitches to prepare them for anastomosis as a common channel [14, 15]. It might be better to use stay sutures during anastomosis (Fig. 2). In another reconstruction technique for plural neighboring ducts, the Glissonean sheath, including plural orifices, could be treated as a single duct by regarding the septa as a thick wall of the duct. When more than one duct orifice appears separately, plural orifices in the jejunum should be created according to the distance between the ducts. In the synchronous reconstruction of multiple individual anastomoses, entire rows of bile duct posterior walls should be accompanied first, followed by the anterior rows, because attempts to complete one anastomosis and then another may be difficult or sometimes impossible.
Fig. 2.

Plasty of neighboring ducts. Two neighboring duct orifices can be joined by two interrupted stitches to prepare them for anastomosis as a common channel. It might be better to use stay sutures during anastomosis
Preparation of Roux-en-Y jejunal limb
Sufficient jejunal limb length can usually be achieved by transecting the jejunum approximately 20 cm distal from the Treitz ligament via dissection of the 2nd or 3rd jejunal vessels. The limb is brought up in a retrocolic fashion to perform side-to-side anastomosis by means of a sufficiently large orifice made in the bottom of the mesocolon following the mobilization of the 2nd and 3rd portions of the duodenum. Alternatively, a retrogastric route can be used in patients who are morbid obese [16].
Creation of an anastomotic orifice in the jejunal limb and insertion of transanastomotic external drainage tubes
An anastomotic orifice in the jejunal limb should be created in a site that avoids tension at the anastomotic site by taking the length into concern that the stump of the jejunal limb would be attached to the peritoneum, because the transanastomotic tubes used for external biliary drainage should be brought out through the jejunal limb. As the jejunal incision becomes enlarged during the anastomosis, it should initially be smaller than the width of the bile duct.
The transanastomotic tubes we have used are 5-French polyvinyl chloride tubes (pancreatic duct drainage tube; Sumitomo Bakelite Co., Tokyo, Japan) that have a bulge 3 cm from the tip, multiple side holes, and a radiopaque line. The same number of tubes as bile ducts to be reconstructed are inserted through the jejunal incision and pulled out from the jejunal stump using blunt needles attached to the ends of the tubes (Fig. 3). The tip of each tube should be seized with mosquito forceps to prevent it from slipping out.
Fig. 3.
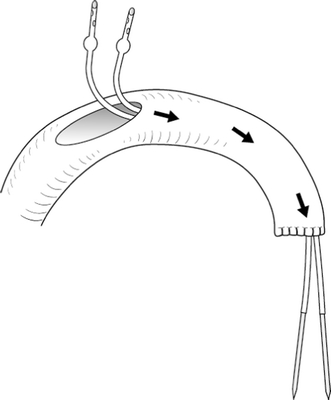
Preparation of the transanastomotic stent tube. 5-French polyvinyl chloride tubes with knots 3 cm from the tips, multiple side holes, and radiopaque lines are used, along with a blunt needle attached to each end. The same number of tubes as bile ducts to be reconstructed are inserted from the jejunal incision and pulled out from the jejunal stump using the blunt needle
Sutures of the posterior layer of the anastomosis
Single-layer interrupted sutures with 4-0 or 5-0 absorbable monofilament material are used for the anastomosis. Expert operators can use a limited number of continuous sutures in anastomosis of the extrahepatic duct. In the reconstruction of the intrahepatic duct, the wall of the bile duct appears as connective tissue after removing the portal vein and the hepatic artery from the Glissonean pedicle [13]. Thus, it is important to mobilize these vessels far enough away from the Glissonean pedicle to avert injuries caused by the suture needle during the anastomosis.
Firstly, two absorbable sutures 75 cm in length are placed in both corners of the jejunum and bile duct, in the case of the jejunum using a needle passing from the outside inwards and with the bile duct passing from the inside outwards to be tied on the outside of the anastomosis. The approximate center of each stitch is grasped by a rubber-shod clamp (small rubber-tipped forceps) so as to maintain distance between the jejunum and the bile duct by suspending them together, with the forceps clipping the bilateral ends of the stitch (ropeway method) (Fig. 4). Next, stitches using absorbable suture material 45 cm in length are placed so as to complete the posterior row approximating the jejunum and bile duct. The needles are passed through the jejunum at an interval of 1–2.5 mm from the inside outwards and through the bile duct from the outside inwards to be tied within the lumen. In order to maintain a favorable view during the anastomoses of multiple ducts, the stitches are serially introduced starting from the most dorsal side toward the ventral side. For the purpose of subsequent identification and prevention of suture tangling, both ends of the stitches should be grasped by small forceps and hung them in order with a large forceps. During suturing, stitches placed previously should be tented and moved aside by hooking with a right-angle forceps to prevent each stitch from tangling. When creating a large anastomosis, a stay suture placed in the center of the orifice can help surgeons to plan the suture interval. One of the sutures used for fixation of a transanastomotic stent might be clipped with a different type of forceps for easy recognition. Using a rapid-absorbing suture material for fixing the stent may enable it to be withdrawn without difficulty on the 14th postoperative day. After suturing the entire posterior row of the anastomosis, the clips for the ropeway method are released to “railroad” the jejunal limb down to the bile ducts’ orifices. The sutures except those at each corner are tied serially on the inside of the lumen. Surgeons should pay attention not to tear the bile duct by using improper ligation technique. Tied sutures of the posterior row are then cut, except the ones involved in stent fixation.
Fig. 4.

Ropeway method for the anastomosis of the posterior row. The approximate center of the each stitch is clipped by a rubber-shod clamp (small rubber-tipped forceps) so as to maintain distance between the jejunum and the bile duct by suspending them together with forceps clipping the bilateral ends of the stitch
Insertion and fixation of the transanastomotic stent
The stent tubes are inserted into bile ducts passing above the strings of the stent fixation suture, which form an opening in the shape of a letter “V” (Fig. 5). The fixation is usually performed on the proximal side of the bulge of the tube to prevent the tube from slipping out. In cases where the tube cannot be inserted deeply due to the small diameter of the duct, the fixation of the tube might alternatively be performed on the distal side of the tube’s bluge.
Fig. 5.

Insertion and fixation of the transanastomotic stent tube(s). A stent tube is inserted into a bile duct passing above the strings of the stent fixation suture, which form an opening in the shape of a letter “V”. The fixation is usually performed on the proximal side of the bulge of the tube to prevent the tube from slipping out
Sutures of the anterior layer of the anastomosis
The anterior row of sutures is placed to complete the approximation of the jejunum and bile duct, using absorbable suture material of 45 cm in length. As with the posterior row, suturing should start at the most dorsal side and progress ventrally. The needles are passed through the jejunum from the outside inwards, and through the bile duct from the inside outwards to be tied on the outside. After the suturing of the entire anterior row of the anastomosis is complete, all sutures (including those at both corners) are tied serially on the outside of the anastomosis. The mucosal layer of the jejunum should be buried intraluminally during the tying. In cases requiring reconstruction of tiny branches where the intraluminal mucosal layer cannot be recognized, needles should be inserted along with the stent tube in order to securely stitch the mucosa of the duct.
Fixation of the stent tube to the jejunal stump
The jejunal wall where the stent tubes have been pulled out is buried with interrupted sutures of seromuscular layer of the jejunum. After that, the tubes are fixed to the jejunal serosal layer with absorbable suture. Use of rapid-absorbing material is preferable in order to permit removal of the tube within a few weeks. The stump of the proximal jejunum is anastomosed with the side wall of the Roux-en-Y limb in end-to-side or side-to-side fashion.
Strategy for the reconstruction of thin and fragile bile ducts
In reconstructing the intrahepatic ducts, the portal side of the duct wall should be treated as the posterior wall of the anastomosis and sutured first, since this side is relatively thick and tough compared with the opposite side because of the existence of rich fibrous tissue. Of course, it is rather important to practice precise ligation technique, placing one of the fingers pulling the suture string beyond the tying point when making knots. If a wall is torn while tying the sutures, indwelling a perianastomotic sump tube with a continuous drainage system could be the best treatment instead of adding sutures over the torn duct. If a transanastomotic tube is adequately placed and the duct orifice is covered with the jejunum, the bile leakage could disappear within a few postoperative days as a result of the preemptive perianastomotic continuous drainage.
Postoperative management of hepaticojejunostomy after hepatobiliary resections
Especially in patients who undergo reconstruction of the relatively small intrahepatic branches, an external biliary drainage tube may not work at all or may stop aspirating suddenly during the early postoperative days. An obstruction of the stent tube may occur in these cases; however, no special treatment is necessary because bile juice can flow into the jejunum through the space between the luminal surface and the stent tube. Cholangiography via the stent tube should be strictly limited except in cases of severe and persistent bile leakage, because the procedure frequently causes severe cholangitis during the acute phase after the hepatectomy.
Discussion
In surgery for hepatobiliary malignancy, reconstruction of the biliary system with hepaticojejunostomy has become a standard procedure [1–4, 7, 8, 15]. The mucosa-to-mucosa anastomosis using a Roux-en-Y jejunal limb has proved to be safe and feasible even in the reconstruction of multiple subsegmental ducts, with postoperative bile leakage frequency rates of 2.4–5.6% [2–4]. Choledochoduodenostomy or hepaticoduodenostomy are accepted alternative approaches to bilioenteric reconstruction. The procedure seems to be preferable from an anatomical point of view when it is used only for the reconstruction of the middle bile duct, excluding the hilar or intrahepatic ducts. The long-term outcome of hepaticoduodenostomy has been reported to be comparable with that of hepaticojejunostomy as regards biliary function [11]. However, bilious gastritis due to duodenogastric reflux has occurred significantly more frequently following hepaticoduodenostomy than after hepaticojejunostomy in the treatment of benign disease [17]. Thus, reconstruction using the duodenum would not be the first choice for reconstructing the intestine. Duct-to-duct reconstruction, which is usually conducted in conjunction with liver transplantation, is often accompanied by biliary complications such as anastomotic leakage or stricture, the rate of which have reached up to 40%, even in recent studies [18]. For patients who suffer from such complications, aggressive management with hepaticojejunostomy has been shown to be more beneficial than repeated endoscopic and/or interventional treatments during the early posttransplant period [9, 19]. Similarly, patients who experience intraoperative bile duct injuries during laparoscopic surgery occasionally undergo duct-to-duct anastomosis, and up to 10% of these suffer from biliary stricture or leakage [19]. Despite recent advancements in endoscopic and interventional treatments, the majority of patients with major bile duct injuries finally undergo Roux-en-Y hepaticojejunostomy after long-term non-surgical treatment [19, 20]. To maximize postoperative quality of life, the choice of hepaticojejunostomy instead of duct-to-duct anastomosis for patients with iatrogenic major bile duct injury should be more aggressively considered.
The use of transanastomotic stents seems to be nonessential for anastomosis between the jejunum and distal bile ducts such as the common hepatic duct or bilateral hepatic duct [10, 21]. However, in biliary reconstruction following hepatobiliary resection, which usually requires stitches on the subsegmental small branches, we believe the transanastomotic stent is indispensable for recognizing the small duct orifices buried in the connective tissue of the Glissonean sheath. Especially in patients whose bile ducts were torn during the anastomosis, or who suffered from bile leakage postoperatively, stent tubes can play an important role in achieving complete healing of the anastomosis by maintaining continuity between the duct and jejunum, preserving the luminal space, and reducing the volume of bile leakage.
Most cases of postoperative bile leakage after bilioenteric anastomosis can be treated conservatively by maintaining a prophylactically placed drain and a transanastomotic stent [2, 8, 22]. Persistent and intractable bile leakage is caused by one or more overlooked and isolated bile ducts that have not been anastomosed. Ethanol injection therapy may be necessary to eradicate the bile duct [23]. It is rather important not to miss small bile ducts during anastomosis, especially in the reconstruction of intrahepatic or hilar bile ducts.
The most frequent late complication after bilioenteric anastomosis is cholangitis, which is sometimes associated with intrahepatic lithiasis [7]. Although this condition is usually attributed to retrograde bacterial infection, it is important to use imaging studies to clarify whether an anastomotic stricture exists. Furthermore, once such a stricture is definitively demonstrated, its dilatation can be performed by percutaneous transhepatic cholangioscopic (PTCS) drainage [24] or an endoscopic approach [25], but only once recurrence of the malignancy has been ruled out.
Summary and conclusions
After biliary system resection, reconstruction using the Roux-en-Y jejunal limb has been well-established with safe and secured results, even when that is performed with the small intrahepatic branches. In contrast with the lower extrahepatic bile duct, the wall of the hilar or intrahepatic bile ducts can be recognized within the fibrous connective tissue in the Glissonean pedicle. Regardless of the level of the bile duct, precise mucosa-to-mucosa single-layer interrupted sutures and placement of transanastomotic stent tubes achieve sufficient anastomosis with infrequent bile leakage or stricture. Meticulous inspection to avoid overlooking small bile ducts can decrease the chance of postoperative intractable bile leakage after the reconstruction of the hilar or intrahepatic ducts.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Video supplement. The technique of the hepaticojejunostomy following right hepatectomy and caudate lobectomy (segmentectomy 1) with pancreatoduodenectomy for hilar cholangiocarcinoma is presented. The four orifices of the bile duct were anastomosed with an incision created in the Roux-en-Y jejunal limb. The sutures of the posterior row of the anastomosis were firstly made using ropeway method, and then transanastomotic biliary stent tubes were inserted and fixed after tying the sutures of the posterior row. Finally anterior row of the anastomosis was closed with interrupted sutures. (MPG 27722 kb)
Conflict of interest
None.
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Footnotes
This article is based on the studies first reported in Highly Advanced Surgery for Hapato-Biliary-Pancreatic Field (in Japanese). Tokyo: Igaku-Shoin, 2010.
References
- 1.Sondenaa K, Kubota K, Sano K, Takayama T, Makuuchi M. Successful reconstruction of segmental or subsegmental bile ducts after resection of hilar bile ducts: short- and long-term results. Hepatogastroenterology. 2004;51:1278–1281. [PubMed] [Google Scholar]
- 2.Nagino M, Nishio H, Ebata T, Yokoyama Y, Igami T, Nimura Y. Intrahepatic cholangiojejunostomy following hepatobiliary resection. Br J Surg. 2007;94:70–77. doi: 10.1002/bjs.5531. [DOI] [PubMed] [Google Scholar]
- 3.Antolovic D, Koch M, Galindo L, Wolff S, Music E, Kienle P, et al. Hepaticojejunostomy—analysis of risk factors for postoperative bile leaks and surgical complications. J Gastrointest Surg. 2007;11:555–561. doi: 10.1007/s11605-007-0166-3. [DOI] [PubMed] [Google Scholar]
- 4.Hirano S, Kondo S, Tanaka E, Shichinohe T, Tsuchikawa T, Kato K, et al. Outcome of surgical treatment of hilar cholangiocarcinoma: a special reference to postoperative morbidity and mortality. J Hepatobiliary Pancreat Sci. 2010;17:455–462. doi: 10.1007/s00534-009-0208-1. [DOI] [PubMed] [Google Scholar]
- 5.Hasegawa K, Kokudo N, Imamura H, Sano K, Aoki T, Miki K, et al. Bilioenteric reconstruction for small bile ducts without mucosa-to-mucosa alignment: long-term results. Arch Surg. 2004;139:1050–1054. doi: 10.1001/archsurg.139.10.1050. [DOI] [PubMed] [Google Scholar]
- 6.Aydin U, Yedibela S, Yazici P, Aydinli B, Zeytunlu M, Kilic M, et al. A new technique of biliary reconstruction after “high hilar resection” of hilar cholangiocarcinoma with tumor extension to secondary and tertiary biliary radicals. Ann Surg. 2008;15:1871–1879. doi: 10.1245/s10434-008-9926-x. [DOI] [PubMed] [Google Scholar]
- 7.Meunier B, Lakehal M, Tay KH, Malledant Y, Launois B. Surgical complications and treatment during resection for malignancy of the high bile duct. World J Surg. 2001;25:1284–1288. doi: 10.1007/s00268-001-0111-7. [DOI] [PubMed] [Google Scholar]
- 8.Ferrero A, Russolillo N, Viganò L, Sgotto E, Lo Tesoriere R, Amisano M, et al. Safety of conservative management of bile leakage after hepatectomy with biliary reconstruction. J Gastrointest Surg. 2008;12:2204–2211. doi: 10.1007/s11605-008-0586-8. [DOI] [PubMed] [Google Scholar]
- 9.Langer FB, Györi GP, Pokorny H, Burghuber C, Rasoul-Rockenschaub S, Berlakovich GA, et al. Outcome of hepaticojejunostomy for biliary tract obstruction following liver transplantation. Clin Transpl. 2009;23:361–367. doi: 10.1111/j.1399-0012.2008.00923.x. [DOI] [PubMed] [Google Scholar]
- 10.Nakanishi Y, Zen Y, Kawakami H, Kubota K, Itoh T, Hirano S, et al. Extrahepatic bile duct carcinoma with extensive intraepithelial spread: a clinicopathological study of 21 cases. Mod Pathol. 2008;21:807–816. doi: 10.1038/modpathol.2008.65. [DOI] [PubMed] [Google Scholar]
- 11.Moraca RJ, Lee FT, Ryan JA, Jr, Traverso LW. Long-term biliary function after reconstruction of major bile duct injuries with hepaticoduodenostomy or hepaticojejunostomy. Arch Surg. 2002;137:889–893. doi: 10.1001/archsurg.137.8.889. [DOI] [PubMed] [Google Scholar]
- 12.Dixon E, Vollmer CM, Jr, Bathe O, Sutherland F. Training, practice, and referral patterns in hepatobiliary and pancreatic surgery: survey of general surgeons. J Gastrointest Surg. 2005;9:109–114. doi: 10.1016/j.gassur.2004.03.008. [DOI] [PubMed] [Google Scholar]
- 13.Hirano S, Tanaka E, Shichinohe T, Suzuki O, Hazama K, Kitagami H, et al. Treatment strategy for hilar cholangiocarcinoma, with special reference to the limits of ductal resection in right-sided hepatectomies. J Hepatobiliary Pancreat Surg. 2007;14:429–433. doi: 10.1007/s00534-006-1190-5. [DOI] [PubMed] [Google Scholar]
- 14.Rossi RL, Tsao JI. Biliary reconstruction. Surg Clin North Am. 1994;74:825–841. [PubMed] [Google Scholar]
- 15.Blumgart LH, Baer HU. Hilar and intrahepatic biliary-enteric anastomosis. In: Blumgart LH, editor. Surgery of the liver and biliary tract. New York: Churchill Livingstone; 2004. pp. 1051–1067. [Google Scholar]
- 16.Nagino M, Kamiya J, Kanai M, Uesaka K, Sano T, Arai T, et al. Hepaticojejunostomy using a Roux-en-Y jejunal limb via the retrocolic-retrogastric route. Langenbecks Arch Surg. 2002;387:188–189. doi: 10.1007/s00423-002-0304-z. [DOI] [PubMed] [Google Scholar]
- 17.Shimotakahara A, Yamataka A, Yanai T, Kobayashi H, Okazaki T, Lane GJ, et al. Roux-en-Y hepaticojejunostomy or hepaticoduodenostomy for biliary reconstruction during the surgical treatment of choledochal cyst: which is better? Pediatr Surg Int. 2005;21:5–7. doi: 10.1007/s00383-004-1252-1. [DOI] [PubMed] [Google Scholar]
- 18.Tsui TY, Schlitt HJ, Obed A. Prospective evaluation of biliary reconstruction with duct-to-duct continuous suture in adult live donor liver transplantation. Langenbecks Arch Surg. 2011;396:209–215. doi: 10.1007/s00423-010-0661-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.de Reuver PR, Busch OR, Rauws EA, Lameris JS, van Gulik TM, Gouma DJ. Long-term results of a primary end-to-end anastomosis in preoperative detected bile duct injury. J Gastrointest Surg. 2007;11:296–302. doi: 10.1007/s11605-007-0087-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Sicklick JK, Camp MS, Lillemoe KD, Melton GB, Yeo CJ, Campbell KA, et al. Surgical management of bile duct injuries sustained during laparoscopic cholecystectomy: perioperative results in 200 patients. Ann Surg. 2005;241:786–792. doi: 10.1097/01.sla.0000161029.27410.71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Tocchi A, Costa G, Lepre L, Liotta G, Mazzoni G, Sita A. The long-term outcome of hepaticojejunostomy in the treatment of benign bile duct strictures. Ann Surg. 1996;224:162–167. doi: 10.1097/00000658-199608000-00008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.DiFronzo LA, Egrari S, O’Connell TX. Safety and durability of single-layer, stentless, biliary-enteric anastomosis. Am Surg. 1998;64:917–920. [PubMed] [Google Scholar]
- 23.Matsumoto T, Iwaki K, Hagino Y, Kawano K, Kitano S, Tomonari K, et al. Ethanol injection therapy of an isolated bile duct associated with a biliary-cutaneous fistula. J Gastroenterol Hepatol. 2002;17:807–810. doi: 10.1046/j.1440-1746.2002.02661.x. [DOI] [PubMed] [Google Scholar]
- 24.Schumacher B, Othman T, Jansen M, Preiss C, Neuhaus H. Long-term follow-up of percutaneous transhepatic therapy (PTT) in patients with definite benign anastomotic strictures after hepaticojejunostomy. Endoscopy. 2001;33:409–415. doi: 10.1055/s-2001-14264. [DOI] [PubMed] [Google Scholar]
- 25.Raithel M, Naegel A, Dormann H, Derossi T, Diebel H, Raithel S, et al. Modern enteroscopic interventions and characterization of nonmalignant postsurgical biliary anastomosis by double-balloon endoscopy. Surg Endosc. 2011. Epub ahead of print. [DOI] [PubMed]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Video supplement. The technique of the hepaticojejunostomy following right hepatectomy and caudate lobectomy (segmentectomy 1) with pancreatoduodenectomy for hilar cholangiocarcinoma is presented. The four orifices of the bile duct were anastomosed with an incision created in the Roux-en-Y jejunal limb. The sutures of the posterior row of the anastomosis were firstly made using ropeway method, and then transanastomotic biliary stent tubes were inserted and fixed after tying the sutures of the posterior row. Finally anterior row of the anastomosis was closed with interrupted sutures. (MPG 27722 kb)