

Spending on prescription drugs is an important component of health care costs in this country. The $15 billion that Canadians spent on prescription drugs in 2003 represented 13% of all health care expenditures. Yet prescription drug spending varies markedly between provinces. Data from the Canadian Institute for Health Information show that per capita spending on prescription drugs in 2002 ranged from approximately $350 in British Columbia to over $500 in Ontario and Quebec.
This variation is an effect of differences in the volume of drugs prescribed, prices paid for chemically equivalent drugs and the selection of drugs within therapeutic classes. Using methods described elsewhere,1 I calculated interprovincial differences in these “volume effects,” “price effects” and “therapeutic choices” using Canadian CompuScript data (IMS Health, Canada) for oral solid prescription drugs, which account for 79% of the market. IMS Health groups these drugs by primary indication into 171 mutually exclusive drug classes, which are further aggregated into 40 treatment categories.
In 2002 per capita spending on oral solid prescription drugs varied across the provinces by 51%, ranging from $269 in Saskatchewan to $406 in Quebec (see Fig. 1 and the online table [www.cmaj.ca/cgi/content/full/170/3/329/DC1]). In general, western provinces spent less on these drugs than did eastern provinces. Much of this difference is explained by volume effects. In particular, the volume of drug purchases was lower in British Columbia and Saskatchewan than in the other provinces. Although Quebec residents received more prescriptions per capita, the average prescription length was shorter than in the other provinces. The net effect was, as in Ontario, a modestly higher volume effect than in the other provinces. In New Brunswick and Nova Scotia, the volume effect was more pronounced.
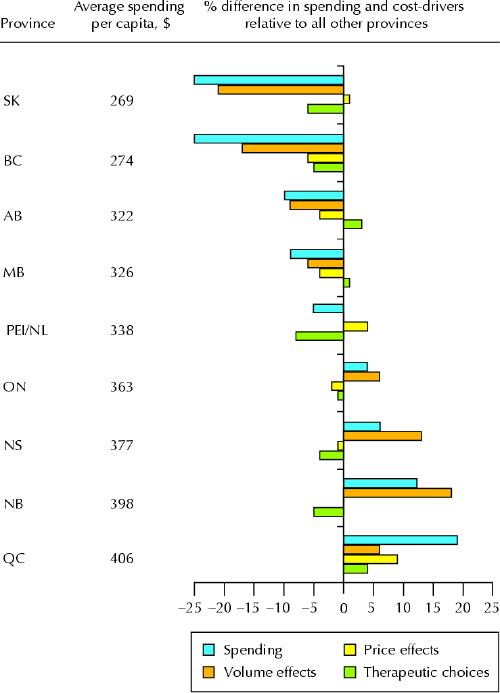
Fig. 1: Magnitude and determinants of interprovincial variation in per capita drug spending on oral solid prescription drugs, 2002. Cost-drivers are shown as volume effects, price effects and therapeutic choices. Volume effects represent differences in the number of prescriptions for oral solid drugs and in the average number of units dispensed per prescription. Price effects represent differences in unit prices for products already on the market and in cost savings from the use of generic drugs. Therapeutic choices represent differences in the choice of product class from which to prescribe and in the selection of specific drugs from within a class. Data are drawn from the Canadian CompuScript Audit (IMS Health, Canada). Data collected from 2100 retail pharmacies were projected by IMS Health to the population of each province, with the exception of PEI and Newfoundland and Labrador, whose data are combined in view of their smaller populations.
Price factors explain very little of the cost differences across provinces. Variations in unit prices, including all professional fees and mark-up, were no greater than 7%. Much of the variation in price reflected average dispensing fees paid per unit of drug purchased. Shorter prescriptions result in higher dispensing fees per unit, as the examples of British Columbia and Quebec illustrate. The average total unit price in Quebec was 7% higher than the average for all other provinces combined, but the average length of prescriptions in Quebec was far shorter. After adjustment for dispensing fees paid per unit, Quebec prices exceeded the average for the other provinces by only 2%. British Columbia had relatively long prescriptions, resulting in total prices that were 4% below the average for the other provinces. However, adjustment for dispensing fees renders British Columbia prices only 2% below the average for the other provinces. Removing estimated dispensing fees from all provinces, based on average fees paid by provincial drug plans, reduces drug price variation across Canada to only 4%.
Therapeutic choices explain some of the variation in drug costs across the country. Quebec residents purchased prescriptions for relatively more costly classes of drug within given broad therapeutic categories than did residents of the other provinces. Residents of Saskatchewan, British Columbia and the Atlantic Provinces tended to purchase from the least costly classes of drug within treatment categories. For example, from within the cardiovascular category they received a greater proportion of thiazide diuretics than ACE inhibitors, calcium-channel blockers or angiotensin II receptor antagonists. Variation in drug selection within narrow classes was more modest. Residents of British Columbia and Saskatchewan received a lower-cost mix of drugs from within narrow drug classes than did residents of the other provinces.
In general, observed differences in per capita expenditures stem from multiple cost-drivers, the most significant being the volume of drugs purchased and the type of products selected. Residents of Quebec, with the highest per capita drug expenditures in Canada, used more prescription drugs, used a more expensive mix of products and paid more per unit purchased than did residents of the other provinces. In contrast, residents of British Columbia and Saskatchewan purchased a lower volume of drugs than residents of the other provinces and received relatively low-cost therapeutic alternatives when drugs were prescribed. Policy decisions are likely to exert a significant influence on these dynamics. Without evidence on appropriate levels of drug use, it is difficult to assess whether provinces with high levels of spending are over-investing, or whether other provinces are under-investing, in pharmaceuticals. Canadian researchers and policy-makers should focus attention on determining the influences on and the impact of overall drug utilization and broad therapeutic choices.
Steve Morgan Centre for Health Services and Policy Research University of British Columbia Vancouver, BC
Supplementary Material
Reference
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.