

Abstract
Methamphetamine abuse has become a significant problem in the United States with recent surveys reporting that nearly 10 million Americans have tried methamphetamine at least once. Methamphetamine is a stimulant drug that causes the release of monoamine neurotransmitters. Among its most deleterious effects are its ability to produce tachycardia, hypertension, and ischemia. However, it also has the potential to cause clinically significant effects outside of the cardiovascular system although a case of paralytic ileus caused by methamphetamine use has not been described before in the literature. Described is a case in which a patient presented with chest and abdominal pain after methamphetamine use. The patient was ultimately diagnosed with a methamphetamine-induced paralytic ileus.
Introduction
Crystal meth (methamphetamine hydrochloride) is a stimulant which produces a rapid and intense “high” secondary to release of the monoamine neurotransmitters dopamine, serotonin, and norepinepherine.1 The drug's potentially therapeutic effects include alertness, energy, euphoria, and suppression of appetite.2 However, it has multiple harmful effects on the cardiovascular and gastrointestinal systems. The rapid release of norepinephrine results in activation of alpha-1 receptors and vasoconstriction.3 Depending on the duration and severity of this vasoconstriction ischemia can result. Additionally, independent of its actions on the cardiovascular system, methamphetamine can also effect the gastrointestinal system through direct affects on cocaineregulate and amphetamine-regulate transcript (CART) peptide as well as indirect effects from the release of dopamine and other neurotransmitters.4,5 Herein, we present a case of methamphetamine-induced ileus and describe the biochemical and neurologic mechanisms of this process.
Case Report
A 19-year-old man was seen in an acute care clinic for right-sided chest pain after a morning run and was found to have sinus tachycardia with a rate of 138 beats per minute. He was subsequently transferred to the emergency department for further care. On arrival his chest pain had resolved, but he now had focal right lower quadrant abdominal pain (described as a sharp, stabbing pain without radiation) and anorexia. He denied having any other symptoms and he was otherwise healthy. He admitted to having been drinking alcohol the night before, but initially denied using any illicit drugs. His physical exam was remarkable for tenderness to palpation in the right lower quadrant, diminished bowel sounds, and the absence of peritoneal signs. His laboratory analysis was remarkable for a white blood cell count of 22.0 × 109 cells/L with 85% neutrophils, arterial pH of 7.44, PaCO2 of 27 mmHg, serum bicarbonate of 16 mmol/L, and base deficit of 6 mmol/L. His urine drug screen demonstrated the presence of amphetamines, and confirmatory testing determined the origin to be methamphetamine. An abdominal X-ray series demonstrated the presence of air throughout the small intestine, appendix, and colon (Figure 1). A CT scan demonstrated similar findings to the X-ray; of note it was without evidence of ischemic changes to the bowel. The patient was admitted to the hospital for a methamphetamine-induced ileus and observed for 48 hours. After correction of his physiologic abnormalities and consultation with the psychiatric service for drug abuse counseling he was discharged from the hospital.
Figure 1.
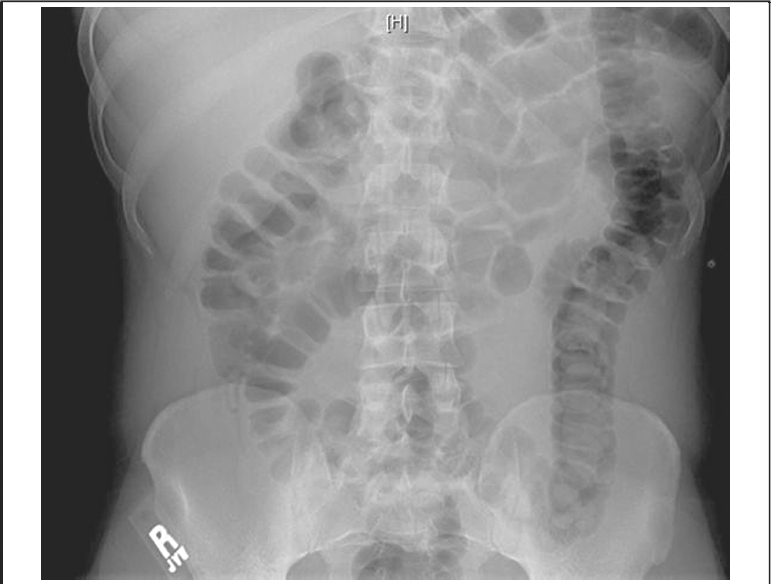
Abdominal X-ray showing dilated loops of bowel with intra-appendiceal air.
Discussion
The majority of catastrophic complications of methamphetamine use are caused by the rapid and sustained release of norepinephrine and its effects on the cardiovascular system. The release of norepinephrine results in arterial vasoconstriction via alpha-1 receptors and increased chronotropy and inotropy via beta-1 rectepors.3 These effects produce the tachycardia and hypertension characteristic of methamphetamine use. If severe enough this can result in cardiac ischemia. Similar effects can also be seen in the mesenteric vessels, as demonstrated by the many case reports of methamphetamine-inducted acute mesenteric ischemia.6,7
This case highlights the ability of methamphetamines to have non-vascular effects as well. The mechanism by which methamphetamines can induce an ileus is only partially understood. We believe this is the first described case. The potential for a direct effect on the gastrointestinal system has been proposed by the discovery of the cocaine and amphetamine regulated transcript (CART) receptor in the stomach, small intestine, and large intestine.8 While early studies suggested that CART may play a role in gastrointestinal motility, more recent studies have questioned these findings and suggest that it has limited to no effects on an otherwise normal enteric system.9 Rather, the role of CART within the enteric tract may be for remodeling after injury or in the presence of chronic derangements. The more likely source of the ileus is through the methadonemediated release of dopamine and norepinephrine. Activation of the dopamine-1 receptor results in a significant decrease in small bowel contractility and alteration of the migratory motor complex.4,10 Additionally, norepinephrine is also know to alter the enteric nervous system, resulting in a decrease in enteric muscle tone.3 These decreases in neurologic function result in the lack of enteric tone characteristic of ileus.
Finally, this case adds to the large differential of causes for right lower quadrant abdominal pain. Although the patient had many features that initially suggested that he may have appendicitis (tenderness in the right lower quadrant, leukocytosis with granulocytosis, and anorexia), careful review of the initial radiologic imaging demonstrated the presence of an air-filled appendix, thereby excluding this as a diagnosis. While methamphetamine-induced paralytic ileus may be a rare entity, given the prevalence of methamphetamine abuse, it should remain within the physician's differential diagnosis.
Footnotes
The views expressed in this manuscript are those of the authors and do not reflect the official policy or position of the Department of the Army, Department of Defense, or the US Government.
Conflict of Interest Statement
None of the authors identify any conflict of interest.
References
- 1.Kish SJ. Pharmacologic mechanism of crystal meth. CMAJ. 2008;178:1679–1682. doi: 10.1503/cmaj.071675. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Linberry TW, Bostwisk JM. Methamphetamine abuse: a perfect storm of complications. Mayo Clinic Proc. 2006;81:77–84. doi: 10.4065/81.1.77. [DOI] [PubMed] [Google Scholar]
- 3.Dunser MW, Hasibeder WR. Sympathetic overstimulation during critical illness: adverse effects of adrenergic stress. J Intensive Care Med. 2009;24:293–316. doi: 10.1177/0885066609340519. [DOI] [PubMed] [Google Scholar]
- 4.Dive A, Foret F, Jamart J, Bulpa P, Installe E. Effect of dopamine on gastrointestinal motility during critical illness. Intensive Care Med. 2000;26:901–907. doi: 10.1007/s001340051279. [DOI] [PubMed] [Google Scholar]
- 5.Tebbe JJ, Ortmann E, Schumacker K, Monnikes H, Kobelt P, Arnold R, et al. Cocaine- and amphetamine-regulated transcript stimulates colonic motility via central CRF receptor activation and peripheral cholinergic pathways in fed, conscious rats. Neurogastroenterol Motil. 2004;16:489–496. doi: 10.1111/j.1365-2982.2004.00561.x. [DOI] [PubMed] [Google Scholar]
- 6.Brannan TA, Soundararajan S, Houghton BL. Methamphetamine-associated shock with intestinal infarction. MedGenMed. 2004;6:6. [PMC free article] [PubMed] [Google Scholar]
- 7.Herr RD, Caravati EM. Acute transient ischemic colitis after oral methamphetamine ingestion. Am J Emerg Med. 1991;9:406–409. doi: 10.1016/0735-6757(91)90073-s. [DOI] [PubMed] [Google Scholar]
- 8.Ekblad E, Kuhar M, Wierup N, Sundler F. Cocaine- and amphetamine-regulated transcript: distribution and function in rat gastrointestinal tract. Neurogastroenterol Motil. 2003;15:545–557. doi: 10.1046/j.1365-2982.2003.00437.x. [DOI] [PubMed] [Google Scholar]
- 9.Ekblad E. CART in the enteric nervous system. Peptides. 2006;27:2024–2030. doi: 10.1016/j.peptides.2005.12.015. [DOI] [PubMed] [Google Scholar]
- 10.Zizzo MG, Mule F, Mastropaolo M, Serio R. D1 receptors play a major role in the dopamine modulation of mouse ileum contractility. Pharmacol Res. 2010;61:371–378. doi: 10.1016/j.phrs.2010.01.015. [DOI] [PubMed] [Google Scholar]