

Background and epidemiology: According to actuarial projections, the number of deaths from chronic obstructive pulmonary disease (COPD) involving Canadian women will increase about 3-fold over the next decade, from 4000 to 12 000, whereas the numbers involving men will rise more modestly, from about 6000 to 8000.1 The rapid rise among women reflects a greater decrease in smoking prevalence among men (from 61% to 25%) than among women (from 38% to 21%) during 1965–2001. For the first time, smoking rates among teenaged girls have now exceeded those among boys.2 This female trajectory led one respirologist presenting grand rounds recently at a Toronto teaching hospital to wryly observe that, like osteoporosis, COPD will soon become known as an “old woman's disease.”
It is one reason why the Canadian Thoracic Society (CTS) recommends that high-dose inhaled corticosteroids, which carry the risk of reducing bone density,3 not be considered first-line therapy for COPD but instead be reserved for patients with moderate to severe COPD who have 3 or more exacerbations a year.
The recommendation is one of many put forth by the CTS in June 2003 for the management of COPD. Overall, the evidence and recommendations outlined by the society serve to position the newer classes of drugs, such as the longer-acting anticholinergics (e.g., tiotropium), in the management of COPD and demonstrate the importance of key interventions such as patient education and access to trained COPD educators and pulmonary rehabilitation services in managing this disease.
COPD is a respiratory disorder largely caused by smoking and is characterized by progressive, partly reversible airway obstruction, systemic manifestations and increasing frequency and severity of exacerbations. Persistent airway inflammation and emphysematous destruction lead to expiratory flow limitation and dynamic collapse of small airways. Air trapping, lung over-inflation and region inequalities of ventilation and perfusion throughout the lungs lead to pulmonary hypertension and right heart failure. Rates of hospital admission are high. In 1998 a conservative estimate of the direct and indirect health care costs of COPD in Canada was $1.67 billion.1
Clinical management: Studies have estimated that more than 50% of patients with COPD remain undiagnosed in the community. The CTS guidelines identify at-risk people for whom targeted spirometric assessment is indicated. However, spirometric values, although necessary for diagnosis, correlate poorly with symptom intensity. Therefore, the CTS guidelines recommend that management decisions be based on an assessment of dyspnea and disability according to the Medical Research Council's scale.4 The guidelines outline a stepwise approach to management (Fig. 1).1 To support the use of long-acting β2-agonists and anticholinergics, the guidelines cite several studies that show how the longer-acting medications offer more sustained improvements in pulmonary function, chronic dyspnea and quality-of-life than do the shorter-acting ones.1
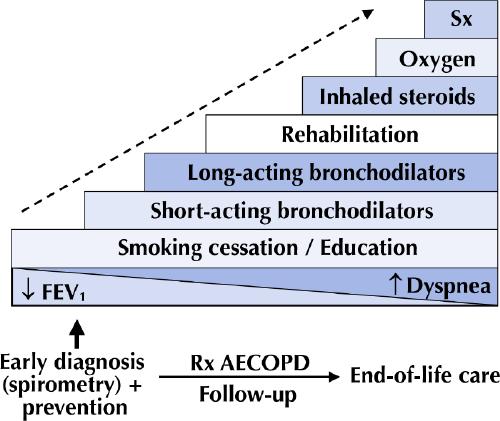
Fig. 1: Stepwise approach to the management of chronic obstructive pulmonary disease (COPD). FEV1 = forced expiratory volume in the first second, Rx AECOPD = treatment of acute exacerbations of COPD, Sx = surgery (lung volume reduction surgery or transplantation). [Reproduced, with permission, from O'Donnell et al.1]
Prevention: Smoking cessation is the single most effective intervention to reduce the risk of COPD. Pneumococcal and influenza vaccinations prevent exacerbations. Comprehensive patient self-management programs and access to trained COPD educators and pulmonary rehabilitation programs improves quality of life and reduces health care use and overall costs.
Erica Weir CMAJ
References
- 1.O'Donnell DE, Hernandez P, Aaron S, Bourbeau J, Marciniuk D, Hodder R, et al. Executive summary: Canadian Thoracic Society recommendations for management of chronic obstructive pulmonary disease — 2003. Can Respir J 2003;10(Suppl A):11A-65A. Available: www.pulsus.com/Respir/10_SA/contents.htm (accessed 2003 Dec 17). [DOI] [PubMed]
- 2.Women's health surveillance report, 2003: a multidimensional look at the health of Canadian women. Ottawa: Health Canada; 2003. Available: http://secure.cihi.ca/cihiweb/dispPage.jsp?cw_page=PG_29_E&cw_topic=29 (accessed 2003 Dec 17).
- 3.Egan JJ, Maden C, Adams JE, Eastell R, Woodcock AA. A randomized, double-blind study comparing the effects of beclomethasone and fluticasone on bone density over two years. Eur Respir J 1999;13:1267-75. [PubMed]
- 4.O'Donnell D, Hernandez P, Aaron S, Bourbeau J, Marciniuk D, Hodder R, et al. Canadian Thoracic Society COPD guidelines: Summary of highlights for family doctors. Can Respir J 2003;10:183-5. [DOI] [PubMed]