

Abstract
Despite longstanding concern that the presence of children deters drug-dependent women from entering treatment, there have been few empirical tests of the relationship between parenting responsibilities and treatment-seeking behavior. In this study, the relationship between number of biological children and treatment history was examined in a cohort of 153 women seeking methadone maintenance treatment. In a standard multiple regression analysis that also allowed for the potential influence of (a) age, (b) education, (c) ethnic minority status, (d) cohabitation with a sexual partner, (e) chronicity of opioid use, and (f) knowledge of HIV infection, there was a significant, negative relationship between number of children and number of earlier contacts for drug abuse treatment. Ethnic minority status and cohabitation with a sexual partner were also associated with fewer earlier contacts; greater chronicity and knowledge of HIV infection were associated with more earlier contacts. Moreover, there was significant moderation of the negative relationship between parenting responsibilities and treatment history by (a) ethnic minority status, (b) cohabitation, and (c) chronicity of use. Within a cross-sectional research design, the findings highlight ways parenting responsibilities may interact with other factors over time to influence the treatment-seeking behavior of drug-dependent women.
Keywords: Opioid dependence, Methadone maintenance, Women, Parenting, Drug treatment history, Pharmacotherapy
1. Introduction
Over the past 30 years, there has been considerable interest in gender and the nature of drug dependence. At this time, there is substantial evidence that, when compared with men, drug-dependent women differ in terms of precursors to addiction (Luthar et al., 1996), the addictive process (Anglin et al., 1987a,b; Hser et al., 1987a,b), patterns of comorbid psychopathology (Brooner et al., 1997; Rounsaville et al., 1982), and related problems (Chatham et al., 1999; Kosten et al., 1985). Consistently, one of the more striking differences involves parenting issues. In general, drug-dependent women are more likely to be a parent (Gerstein et al., 1997; McMahon et al., 2001), they are more likely to be living with their children (Chatham et al., 1999; McMahon et al., 2001), and they are more likely to express concern about parenting issues as they enter treatment (Gerstein et al., 1997; Wechsberg et al., 1998).
As clear gender differences in responsibility for minor children have been documented time and again, unresolved questions about ways parenting responsibilities influence the treatment-seeking behavior of women have emerged. Review of the literature suggests that women repeatedly cite concern about the impact of their drug use on their children as one of the primary reasons to seek help (Davis, 1994; Kearney et al., 1994; Kline, 1996; Rosenbaum, 1981). However, this concern may be tempered by seemingly contradictory values, attitudes, and behavior such that the presence of children may actually deter help-seeking behavior.
For example, values among drug-dependent women that emphasize the importance of caring for children (Alicea and Friedman, 1999; Baker and Carson, 1999; Kearney et al., 1994; Rosenbaum, 1981) may cause some women to defer treatment because they believe they must put the needs of their children first. Similarly, efforts to minimize the impact of their use on family functioning (Baker and Carson, 1999; Kearney et al., 1994) may convince some women that it does not compromise their ability to function as a parent. Perceptions that drugs enhance their ability to cope with the demands of parenting (Baker and Carson, 1999) may also contribute to ambivalence about seeking treatment, and the need to balance drug-taking behaviors against day-to-day responsibilities to care for children (Kearney et al., 1994) may contribute to beliefs that they have no time to seek help.
Furthermore, although guilt about neglect of children may represent a strength to capitalize on once drug-dependent women enroll in treatment (Luthar and Suchman, 1999), need to avoid confronting pervasive feelings of guilt (Baker and Carson, 1999; Woodhouse, 1992) may prevent some from enrolling. More than anything else, intense fear about losing custody of their children to the child welfare system may prevent even the most concerned women from entering treatment (Rosenbaum, 1981). Rather than risk loss of custody, some women may defer treatment until their situation has deteriorated to the point that they must make alternative arrangements for the care of their children or they are already involved with the child welfare system (Kearney et al., 1994).
Ironically, enlightening descriptions of parenting concerns common among drug-dependent women have not been complemented with empirical validation of ways parenting responsibilities influence treatment-seeking behavior, in part because of difficulty clearly establishing links between parenting issues and decisions to seek assistance over time. However, one way to document the potential influence of parenting responsibilities is to examine the relationship between number of biological children and treatment history within cohorts of drug-abusing women. If responsibilities to care for children discourage enrollment in treatment then, with other potential influences held constant, number of biological children should, as a global marker of time spent caring for children, be associated with a more limited treatment history.
Therefore, this study was designed to test the validity of that assumption by examining the relationship between number of biological children and treatment history within a cohort of women entering methadone maintenance treatment. With allowance for the potential influence of (a) demographic characteristics, (b) pattern of cohabitation, (c) chronicity of opioid use, and (d) knowledge of HIV infection, number of biological children was expected to correlate negatively with number of earlier contacts for drug abuse treatment. Given the results of other research, (e.g. see Anglin et al., 1987a, 1997; Grella and Joshi, 1999; Meandzija et al., 1994; Moise et al., 1982a,b; Schuetz et al., 1994), ethnic minority status and the presence of a longstanding sexual partner were expected to be associated with a more limited treatment history, whereas knowledge of HIV infection and greater chronicity of use were expected to be associated with a more extensive treatment history. The possibility that the global relationship between parenting responsibilities and treatment history might be moderated by these other factors was also explored.
2. Method
2.1. Sample
The sample for this study was drawn from a cohort of 162 opioid-dependent women accounting for 177 consecutive admissions to a gender-specific methadone maintenance program located in southern Connecticut. The program offered outpatient and intensive outpatient services to inner-city women within a traditional methadone maintenance framework. Gender-specific enhancements included (a) female counseling staff, (b) child care, (c) medical consultation, (d) psychiatric consultation, (e) parenting groups, and (f) consultation concerning the developmental status of children. To secure entry, women had to meet federal guidelines for admission to methadone maintenance treatment (Center for Substance Abuse Treatment, 1993), and they had to document residence within the urban community served by the program. Admission to the enhanced versus a standard program through a central intake unit was determined only by the availability of an open treatment slot.
Complete data for 153 of the 162 women admitted to the program during a 36-month period were available for analysis. Only information obtained at the time of the most recent admission was retained for the 15 women who had more than one contact, and data for nine others were missing because shortly after admission they were imprisoned, hospitalized, or discharged because they did not return to complete the admission process. Characteristics of the final sample are summarized in Table 1.
Table 1.
Characteristics of the final samplea
| Variable | Final sample |
|---|---|
| Age | 35.10 (6.47) |
| Education | 11.74 (1.89) |
| Ethnicity | |
| Euro-American | 41.83 (64) |
| Ethnic minority | 58.17 (89) |
| African American | 43.14 (66) |
| Hispanic | 15.03 (23) |
| Cohabitation with partner | 46.41 (71) |
| Opioid use | |
| Years regular use | 9.65 (6.86) |
| Intravenous use | 51.63 (79) |
| Days used in past month | 11.49 (12.21) |
| Cocaine use | |
| Years regular use | 5.03 (5.60) |
| Days used in past month | 5.46 (8.64) |
| Known HIV+ | 16.99 (26) |
| Number of biological children | 2.15 (1.55) |
| Number of previous treatments | 3.45 (4.15) |
| ASI composite scores | |
| Alcohol use | 0.04 (0.11) |
| Drug use | 0.19 (0.13) |
| Employment | 0.82 (0.25) |
| Legal | 0.10 (0.18) |
| Medical | 0.22 (0.35) |
| Psychiatric | 0.20 (0.21) |
| Family-Social | 0.20 (0.22) |
| Beck Depression Index | 8.75 (7.14) |
| Global Symptom Index | 0.85 (0.71) |
| PSSS: Family | 13.28 (5.80) |
| PSSS: Friends | 13.41 (4.85) |
| PPVT | 74.55 (18.22) |
N = 153. Values for categorical variables (Ethnicity, Cohabitation, Usual Administration, Known HIV+) represent % (n); values for all others represent M (S.D.). Beck Depression Index is total score on the short version of the Beck Depression Inventory (Beck and Beck, 1972); Global Symptom Index is taken from the Brief Symptom Inventory (Derogatis, 1992); PSSS scores are total score on the Family and Friends subscales of the Perception of Social Support Scale (Procidano and Heller, 1983); PPVT is the standard score from the Peabody Picture Vocabulary Test (Dunn and Dunn, 1981).
As indicated in Table 1, most of the women were between 29 and 42 years of age, and there was substantial representation of African American and Hispanic women. As a group, they averaged approximately 10 years of regular opioid use, approximately half were using intravenously, and at the time of admission, a small number knew they were HIV seropositive. Most of the women (86%) were supporting themselves with public welfare benefits, approximately half were living with a sexual partner, and most (80%) were the biological mother of at least one child.
In addition, the 153 women averaged approximately two (range = 0–6) children, and the average age of their 329 children was 12.1 (S.D. = 7.3) years. Most (75%) of the children were minors, most (75%) of the minor children were living with their mother at the time of her admission, and women who were mothers had been parenting children for approximately 95% of the time they had been using opioids. ASI composite scores, report of psychiatric symptomatology, perception of social support, and a measure of verbal aptitude reflected the presence of mild psychiatric distress, perception of adequate social support, limited verbal aptitude, and serious problems in the area of vocational-educational functioning.
2.2. Procedure
All women admitted to the program completed a traditional clinical assessment supplemented by administration of the Addiction Severity Index (McLellan et al., 1992; National Institute on Drug Abuse, 1993), the Peabody Picture Vocabulary Test (Dunn and Dunn, 1981), and several self-report measures (Beck and Beck, 1972; Derogatis, 1992; Procidano and Heller, 1983). The supplemental component of the evaluation was required of all patients entering the program, and it was administered during the orientation phase of treatment by a bachelor-prepared clinical assistant trained in the standardized administration and scoring of each instrument.
2.3. Measurement
An expanded version of the Addiction Severity Index (McLellan et al., 1992) was used to define the variables of interest in this study. The Addiction Severity Index is a structured interview developed to document current and lifetime problems commonly associated with substance abuse. Specific items are used to document demographic information and problem severity across seven domains of psychosocial functioning: (a) medical, (b) vocational, (c) substance use, (d) legal, (e) family history, (1) family-social relations, and (g) psychiatric. The reliability and validity of the instrument have been documented repeatedly in research done with substance-abusing adults (e.g. see Cacciola et al., 1999; McDermott et al., 1996; McLellan et al., 1992).
For this project, two modifications were made to the standard interview. In the Medical section, two questions were added to gather information about date of last HIV screen and knowledge of HIV infection. Similarly, in the Family-Social Relationships section, a series of questions was added to gather information about number of biological children and the age, gender, custody, and living arrangement of each child.
Standard and supplemental items from the Addiction Severity Index were used to define the eight variables of interest. Age at time of admission, ethnicity, and years of education completed were coded from items in the General Information and Employment sections. Pattern of cohabitation with a sexual partner during the earlier 3 years was coded from the Usual Living Arrangements item in the Family-Social Relations section. Chronicity of opioid use was coded as years of regular opioid use using information taken from the Lifetime Use items in the Drug and Alcohol Use section. Knowledge of HIV infection at time of admission and number of biological children were coded from supplementary questions, and number of earlier contacts for drug abuse treatment was coded from the Lifetime Drug Treatment item in the Drug and Alcohol Use section. When cross referenced with the Drug Detoxification Only item in the same section, 250 (48%) of the 525 treatment contacts were determined to be for detoxification only, and number of contacts for detoxification only correlated almost perfectly (r = 0.90; P = 0.0001) with total number of earlier contacts.
2.4. Data analysis
A standard multiple regression done with a mix of categorical and continuous variables was used to test for a unique relationship between parenting responsibilities and treatment history in a statistical model that allowed for the potential influence of other factors and moderation of the relationship by those factors. Number of biological children was entered as the independent variable, and the number of earlier drug abuse treatments was entered as the dependent variable. Age, years of education, ethnic minority status, pattern of cohabitation, chronicity of opioid use, and knowledge of HIV infection were entered as covariates representing other potential influences on treatment history. Interaction terms created by crossing number of biological children with (a) ethnicity, (b) pattern of cohabitation, (c) chronicity of opioid use, and (d) knowledge of HIV infection were used to represent moderation of the relationship between parenting responsibilities and treatment history.
As suggested by Aiken and West (1991), age and years of education were centered to hold their influence constant at the mean for the sample. Weighted effect coding (Darlington, 1990), rather than dummy or simple effect coding, was used to represent the four dichotomous variables (ethnicity, cohabitation, chronicity of use, and knowledge of HIV infection). When groups represented by dichotomous variables are not equal, weighted effect coding adjusts parameter estimates for those groups so that they represent deviation from the parameters for the entire sample rather than deviation from the parameters associated with a specific comparison group (dummy coding) or an unweighted average of the parameters for the entire sample (simple effect coding) (Aiken and West, 1991; Darlington, 1990).
In this linear regression analysis, F ratios representing tests of main effects with P values less than 0.05 were considered statistically significant. To increase the power of the statistical analysis to detect potentially meaningful moderator effects, F ratios for tests of interaction effects with P values less than 0.10 were considered statistically significant. Squared semipartial correlation coefficients were used to characterize the strength of all effects, and graphical representations were used to characterize the nature of significant moderator effects.
In addition, because coding of ethnicity using three levels (Euro-American, African American, and Hispanic) produced virtually identical findings for African American and Hispanic women, these two groups were collapsed into a single group representing ethnic minority women to reduce the complexity of the analyses and increase statistical power. After a preliminary analysis, chronicity of opioid use was also dichotomized using a median split of the sample to facilitate graphical representation of a significant moderator effect. Finally, data screening indicated that the index of treatment history was significantly and positively skewed. Log10 transformation of this index as recommended by Tabachnick and Fidell (1996) normalized the distribution. However, the regression analysis done using the transformed variable did not produce findings that differed in any meaningful way from those done with the variable in its original format so the latter are presented here to facilitate interpretation of the results.
3. Result
The correlation matrix for the eight variables of interest is presented in Table 2. As indicated, the seven potential influences on treatment history were relatively independent of one another. There were, however, significant, positive, zero-order relationships between age and years of education, age and chronicity of use, age and number of children, and chronicity of use and knowledge of HIV infection. As expected, there was also a significant, negative, zero-order relationship between number of biological children and treatment history. Ethnic minority status also correlated significantly and negatively with treatment history, whereas greater chronicity of use correlated significantly and positively.
Table 2.
Zero-order correlation matrix for number of children, other potential influences, and treatment historya
| Variable | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 |
|---|---|---|---|---|---|---|---|---|
| 1 Age | – | 0.21** | −0.00 | −0.05 | 33** | 0.11 | 0.23** | 0.03 |
| 2 Education | – | −0.17 | 0.02 | 0.03 | −0.04 | −0.08 | 0.06 | |
| 3 Ethnicity | – | 0.04 | 0.07 | 0.14 | 0.14 | −0.29** | ||
| 4 Cohabitation | – | −0.02 | −0.00 | 0.13 | −0.15 | |||
| 5 Chronicity | – | 0.26** | −0.05 | 0.30** | ||||
| 6 Known HIV+ | – | 0.15 | 0.16 | |||||
| 7 Children | – | −0.21* | ||||||
| 8 Previous treatments | – |
N = 153. Weighted effect coding (Darlington, 1990) was used to represent Ethnicity, Cohabitation, Chronicity, and Known HIV+ such that the higher value designates ethnic minority versus Euro-American heritage, cohabitation with a sexual partner versus other living arrangements, greater versus less chronicity, and knowledge of HIV infection versus reportedly seronegative or never tested.
P<0.05;
P<0.01.
In the standard multiple regression analysis, the full statistical model accounted for a significant proportion of the variance in number of previous treatments (R2 = 0.35, F[11,141] = 6.61; P < 0.001). Statistics associated with tests of specific regressors are summarized in Table 3. As noted, there were significant, unique relationships involving (a) ethnicity, (b) pattern of cohabitation, (c) chronicity of opioid use, and (d) knowledge of HIV infection. Parameter estimates indicate that, with the other factors in the statistical model, ethnic minority status and cohabitation with a sexual partner were associated with fewer previous treatments; greater chronicity of use and knowledge of HIV infection were associated with more previous treatments. As the squared semipartial correlation coefficients (sr2) indicate, unique relationships involving ethnic minority status, cohabitation, chronicity of use, and knowledge of HIV infection accounted for 2 to 14% of the variance in number of earlier contacts for treatment.
Table 3.
Results of standard multiple regression analysis examining the relationship between number of children and treatment historya
| Variable | Previous treatments
|
|||
|---|---|---|---|---|
| Sr2 | b | (SEb) | t | |
| Age | 0.00 | −0.03 | (0.05) | −0.61 |
| Education | 0.00 | 0.05 | (0.16) | 0.34 |
| Ethnicity | 0.13 | −2.22 | (0.42) | −5.33*** |
| Cohabitation | 0.04 | −1.55 | (0.54) | −2.85*** |
| Chronicity | 0.07 | 2.28 | (0.59) | 3.87*** |
| Known HIV+ | 0.02 | 2.79 | (1.31) | 2.12** |
| Children | 0.03 | −0.55 | (0.20) | −2.72 |
| Children × Ethnicity | 0.05 | 0.56 | (0.17) | 3.35*** |
| Children × Cohabitation | 0.02 | 0.48 | (0.21) | 2.33** |
| Children × Chronicity | 0.02 | −0.42 | (0.23) | −1.85* |
| Children × Known HIV+ | 0.01 | −0.62 | (0.47) | −1.31 |
N = 153. Intercept = 4.42. Weighted effect coding (Darlington, 1990) was used to represent Ethnicity, Cohabitation, Chronicity, and Known HIV+ such that a higher value designates ethnic minority versus Euro-American heritage, cohabitation with a sexual partner versus other living arrangements, greater versus less chronicity, and knowledge of HIV infection versus reportedly seronegative or never tested.
P<0.10 for tests of interaction effects;
P<0.05;
P<0.01.
As the statistics presented in Table 3 indicate, number of children correlated significantly and negatively with number of previous treatments. The semipartial correlation coefficient (sr2) indicates that this unique relationship accounted for approximately 3% of the variance in treatment history. The nature of the negative relationship with the other potential influences held constant is presented in Fig. 1.
Fig. 1.
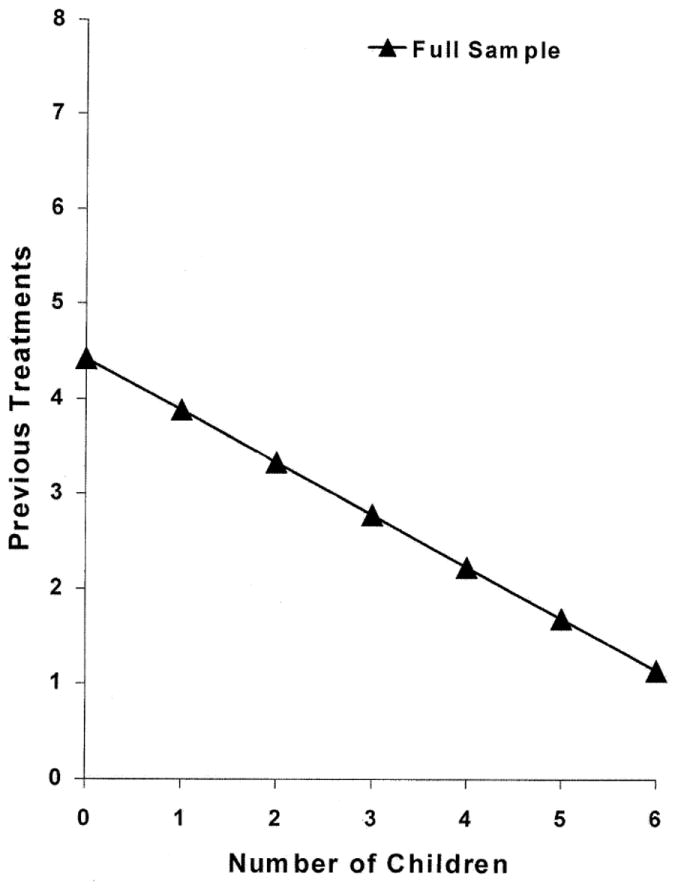
Relationship between number of children and treatment history with other potential influences held constant.
Statistics presented in Table 3 also indicate that there was significant moderation of this negative relationship by (a) ethnicity, (b) pattern of cohabitation, and (c) chronicity of opioid use. As the squared semipartial correlation coefficients (sr2) indicate, these moderator effects accounted for 2 to 6% of the variance in number of previous treatments, and the nature of the effects with other potential influences held constant are presented in Figs. 2 to 4.
Fig. 2.
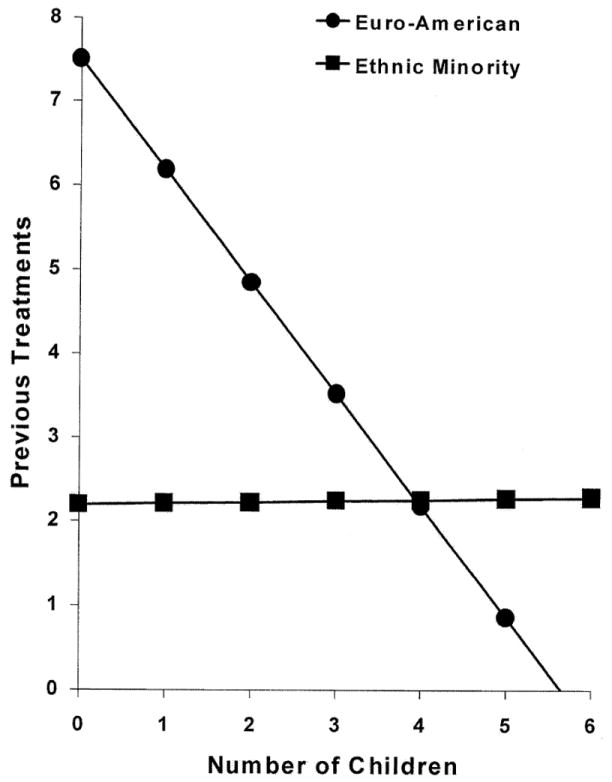
Moderation of the relationship between number of children and treatment history by ethnic minority status with other potential influences held constant.
Fig. 4.
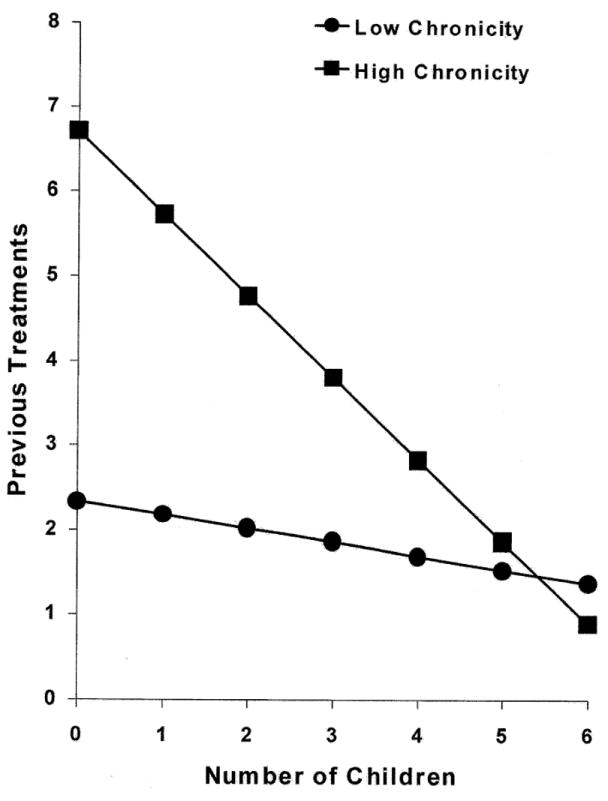
Moderation of the relationship between number of children and treatment history by chronicity of opioid use with other potential influences held constant.
When the moderating influence of ethnicity was examined, ethnic minority status was associated with attenuation of this generally negative relationship; Euro-American heritage was associated with accentuation of the relationship. As indicated in Fig. 2, there was a moderate, negative relationship between number of children and number of previous treatments among Euro-American women that was not present for ethnic minority women. The results indicate that, when compared with their Euro-American peers, ethnic minority women had enrolled in treatment much less frequently and parenting responsibilities did not represent much of a potential influence on their treatment-seeking behavior.
When the moderating influence of living arrangements was examined, cohabitation with a sexual partner for the earlier 3 years was associated with attenuation of this negative relationship; other living arrangements were associated with accentuation of the relationship. As indicated in Fig. 3, there was a moderate, negative relationship between number of biological children and number of previous treatments for women who had not been cohabitating that was not present for women who had been living with a sexual partner. The results suggest that, when compared with women who had not been cohabitating, women living with a sexual partner had enrolled in treatment much less frequently and parenting responsibilities did not represent much of a potential influence on their treatment-seeking behavior.
Fig. 3.
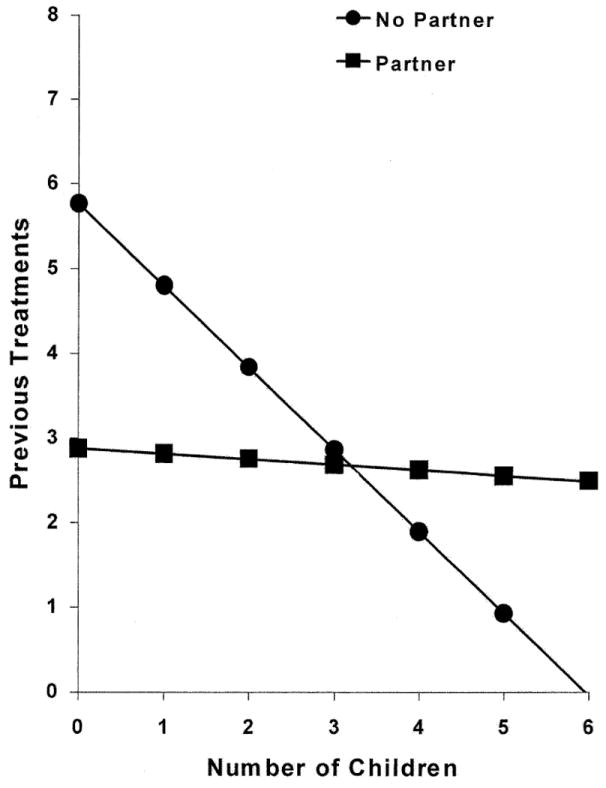
Moderation of the relationship between number of children and treatment history by cohabitation with a sexual partner with other potential influences held constant.
Finally, when the moderating influence of chronicity was examined, greater chronicity of opioid use was associated with accentuation of this negative relationship; less chronicity was associated with attenuation of the relationship. As indicated in Fig. 4, among women with briefer histories of regular opioid use there was little relationship between number of children and number of previous treatments, but there was a moderate, negative relationship for women with longer histories. The results suggest that, when compared with women with less chronicity of use, women with greater chronicity had enrolled in treatment much more frequently and parenting responsibilities were more of a potential influence on their treatment-seeking behavior.
4. Discussion
The results of this study quantify a moderate, negative, qualified relationship between number of biological children and treatment history within this cohort of opioid-dependent women. In the context of a chronic recurring condition that typically involves multiple contacts for different types of intervention, this negative, global relationship supports longstanding assumptions that parenting responsibilities limit treatment-seeking behavior. Unfortunately, there are only limited quantitative data against which to judge this finding because there has been little exploration of within-gender differences in the nature of drug dependence, particularly differences associated with motherhood. Moreover, the empirical data that are available do not document a consistent relationship between parenting responsibilities and treatment-seeking behavior. In general, researchers have asked about potential influences without attempting to link them with actual behavior, and even when there has been an effort to establish links with actual behavior, no two researchers have attempted to link the same markers of parenting responsibilities with the same dimensions of treatment-seeking behavior.
For example, Davis (1994) found that, within a sample of cocaine-dependent women, the negative effects of their drug use on the well-being of their children was the most commonly cited potential cost of continued use. Rounsaville and Kleber (1985) showed that treatment-seeking, opioid-dependent individuals reported greater compromise of parenting when compared with those not interested in treatment suggesting that awareness of that compromise may have influenced the decision to seek help. However, in a survey of substance-abusing women, Allen (1995) found that (a) domestic responsibilities, (b) need for drugs to cope with the stress of daily living, (c) fear of losing custody of children, and (d) shame were four of the six most frequently cited reasons for not seeking help.
Similarly, Faupel and Hanke (1993) found a significant, positive, zero-order relationship between motherhood and enrollment in treatment within a large sample of drug-abusing women, but the relationship did not prove significant in a multivariate analysis that accounted for group differences in age and chronicity of use. In contrast to this, Smith et al. (1992) noted that cocaine-dependent women receiving treatment had significantly fewer dependents than women not receiving treatment, but no multivariate analysis were conducted so the finding may also have been mediated by the presence of other group differences. Davis (1994) noted that, when compared with women who ended prematurely, women who completed 4 months of outpatient cocaine treatment did not differ in terms of number of children or custodial status of children, but they had significantly older children. In a secondary analysis of the CALDATA, Gerstein et al. (1997) found no relationship between child care responsibilities and retention in all types of drug abuse treatment.
Clearly, despite more than 30 years of concern about the issue, there are only limited empirical data that do not yet establish a consistent link between parenting responsibilities and the treatment-seeking behavior of drug-dependent women. However, if consistent across populations of drug-abusing women, the findings described here are of concern. Although more treatments over the course of an addiction career may represent greater severity (Grella and Joshi, 1999), opioid dependence is not likely to resolve without intervention (Cunningham, 1999, 2000), and multiple contacts for treatment may be necessary for many opioid-dependent individuals to establish an extended period of abstinence (Anglin et al., 1987a, 1997). Within opioid-dependent samples, a history of earlier treatment has also been associated with greater motivation to enter treatment, decisions to actually seek admission, greater initial involvement, successful retention, and more positive outcomes (Hser et al., 1998, 1999; Longshore and Hsieh, 1998; Schuetz et al., 1994). Consequently, to the extent that repeated contacts with the treatment system are associated with better outcomes, the results of this study suggest that the long-term prognosis for drug-dependent women to successfully manage their addiction may actually be poorer as parenting responsibilities increase.
Consistently, this negative, global relationship between parenting responsibilities and treatment history was moderated by other potential influences on treatment-seeking behavior. In particular, ethnicity moderated this relationship such that it was only present among women of Euro-American heritage. Ethnic minority women were less likely to have been enrolled in treatment, and parenting responsibilities did not represent much of a potential influence on their treatment-seeking behavior. In general, these results are consistent with other research (e.g. Longshore et al., 1992, 1993) indicating that ethnic minority women do not seek treatment for mental health and substance use problems as frequently as their Euro-American peers. Also, the absence of a relationship between parenting responsibilities and treatment history among ethnic minority women may be explained by the results of other research (Baydar and Brooks-Gunn, 1998; Korbin et al., 1998; Raley, 1995; Singh et al., 1998; Trent and Harlan, 1994; White, 1994) documenting ethnic differences in patterns of support for care of children within extended families that, when other factors do not interfere, may minimize the influence of child care issues on decisions by ethnic minority women to seek help.
The results of this study also highlight ways recent living arrangements may alter this negative, global relationship. Consistent with the results of other research (e.g. Amaro and Hardy-Fanta, 1995) suggesting cohabitation with a sexual partner who typically also abuses drugs can deter women from seeking treatment, cohabitation was associated with fewer previous treatments. However, the findings also suggest that, in the context of greater parenting responsibilities, the presence of a sexual partner may exert relatively little influence on what treatment women do seek. This may occur because opioid-dependent couples frequently make decisions to enter methadone maintenance treatment together (Anglin et al., 1987a), and once committed to enrolling, they may agree to share responsibilities to care for children so both partners can attend.
This negative, global relationship between parenting responsibilities and number of previous treatments was also moderated by chronicity of regular opioid use. Clearly, the relationship was much more pronounced among women with more years of regular opioid use. The data suggest that women with fewer years of regular use did not seek help very often regardless of their parenting status. Moreover, given that approximately half the treatment contacts were for detoxification only, the finding suggests that, as the addiction-treatment-relapse cycle progresses, women caring for children may be less likely to repeatedly seek this largely ineffective intervention (Sees et al., 2000). As the addiction progresses, women caring for children may learn, as qualitative data (e.g. Kearney et al., 1994) suggest, to more effectively manage their level of dependence outside a treatment program. Parenting responsibilities may also contribute to greater ambivalence about seeking either residential treatments that typically require separation from children or maintenance treatments that typically require daily attendance (Rosenbaum, 1981; Rosenbaum and Murphy, 1984).
As with all findings evolving out of a cross-sectional research design, this negative correlation between number of biological children and number of earlier contacts for treatment does not confirm causality. There are no data within this study that directly link the treatment decisions of these women with their parenting responsibilities or any of the other potential influences. Conceptually, this is just one way to establish an initial link between parenting responsibilities and the treatment-seeking behavior of drug-dependent women. In the future, prospective investigations that follow women from active use into treatment might help to establish a more definite causal relationship between parenting responsibilities and decisions to enter treatment.
Similarly, number of biological children is a very crude measure of parenting responsibilities. More sophisticated prospective investigations that follow drug-dependent women over time might examine ways other markers of parenting responsibilities like pregnancy, developmental needs of children, ability to voluntarily place children with friends or extended family, and involvement with the child welfare system influence treatment-seeking behavior. It is also important to note that these findings evolve from the analysis of data obtained from a relatively small cohort of women within a relatively small population of substance-dependent women. Given that there is evidence (e.g. Cohen et al., 1994) of important differences across samples of women using different drugs, it will also be important in future investigations to clearly document the extent to which parenting responsibilities influence the treatment-seeking behavior of women using different drugs of abuse.
Finally, although there has been extensive discussion of ways substance abuse treatment might be enhanced for women, the results of this study suggest that out-reach and engagement may need to be a critical component of any clinical program designed to support drug-dependent mothers. When considered with qualitative data concerning beliefs systems about drug use and parenting (Alicea and Friedman, 1999; Baker and Carson, 1999; Kearney et al., 1994; Woodhouse, 1992), these findings suggest that traditional approaches to enhancement that typically focus on making child care and transportation available to women with children may not be enough. Instead, creative approaches to engagement may need to be utilized in the community to directly address belief systems that prevent drug-dependent women with children from seeking help. The results of this correlational study suggest that, after all ethnic minority women, single mothers with multiple children and extensive drug abuse careers may be in greatest need of outreach and engagement.
Clearly, despite longstanding concern about the issue, surprisingly little is known about ways parenting issues affect the treatment-seeking behavior of drug-abusing women. This negative, global relationship between number of biological children and number of previous treatments in the absence of any clear mediating influence provides quantitative support for the idea that, over the course of a chronic drug abuse career, need to care for children may influence actual behavior. Moreover, multiple qualifications of this global relationship suggest that parenting responsibilities may be just one factor in a complex process that repeatedly influences decisions to seek treatment. That said, the findings clearly highlight the need for better documentation of ways child care responsibilities influence treatment-seeking behavior under varying circumstances so that drug-dependent women with children can be more effectively engaged in treatments known to positively impact both their psychosocial adjustment and that of their children.
Acknowledgments
Primary support for completion of this study was provided by the Center for Substance Abuse Treatment (Grant 5 HR2 T1003 13). Additional support for analysis of the data and preparation of this manuscript was provided by the National Institute on Drug Abuse (Grants P50 DA09241, R03 DAl1988, R0l DAl1498, and R0l DA10726). The authors would like to thank the clients, clinical staff, and administration of The APT Foundation for their support of this project. We would also like to thank Kimberly Doyle, Margaret Christinat, Kimberly DiMeola, and Brian Fitzgerald for their assistance with the collection and management of these data, and we would like to thank Bruce Rounsaville for his helpful comments on an initial draft of this manuscript.
References
- Aiken LS, West SG. Multiple Regression: Testing and Interpreting Interactions. Sage Publications; Newbury Park, CA: 1991. [Google Scholar]
- Alicea M, Friedman J. Motherhood, heroin, and methadone. In: Romero M, Abigail J, editors. Women’s Untold Stories: Breaking Silence, Talking Back, Voicing Complexity. Routledge; New York: 1999. pp. 159–173. [Google Scholar]
- Allen K. Barriers to treatment for addicted African-American women. J Natl Med Assoc. 1995;87:751–756. [PMC free article] [PubMed] [Google Scholar]
- Amaro H, Hardy-Fanta C. Gender relations in addiction and recovery. J Psychoact Drugs. 1995;27:325–337. doi: 10.1080/02791072.1995.10471698. [DOI] [PubMed] [Google Scholar]
- Anglin MD, Hser Y, Booth MW. Sex differences in addict careers. 4. Treatment. Am J Drug Alcohol Abuse. 1987a;13:253–280. doi: 10.3109/00952998709001513. [DOI] [PubMed] [Google Scholar]
- Anglin MD, Hser Y, McGlothlin WH. Sex differences in addict careers. 2. Becoming addicted. Am J Drug Alcohol Abuse. 1987b;13:59–71. doi: 10.3109/00952998709001500. [DOI] [PubMed] [Google Scholar]
- Anglin MD, Hser Y, Grella CE. Drug addiction and treatment careers among clients in the Drug Abuse Treatment Outcome Study (DATO S) Psychol Addict Behav. 1997;11:308–323. [Google Scholar]
- Baker PL, Carson A. “I take care of my kids”: mothering practices of substance abusing women. Gender Soc. 1999;13:347–363. [Google Scholar]
- Baydar N, Brooks-Gunn J. Profiles of grandmothers who help care for their grandchildren. Fam Relat. 1998;47:385–393. [Google Scholar]
- Beck AT, Beck RW. Screening depressed patients in family practice: a rapid technique. Postgrad Med. 1972;52:81–85. doi: 10.1080/00325481.1972.11713319. [DOI] [PubMed] [Google Scholar]
- Brooner RK, King VL, Kidorf M, Schmidt CW, Bigelow GE. Psychiatric and substance use comorbidity among treatment-seeking opioid abusers. Arch Gen Psychiatry. 1997;54:71–80. doi: 10.1001/archpsyc.1997.01830130077015. [DOI] [PubMed] [Google Scholar]
- Cacciola JS, Koppenhaver JM, McKay JR, Alterman AI. Test-retest reliability of the lifetime items on the addiction severity index. Psychol Assess. 1999;11:86–93. [Google Scholar]
- Center for Substance Abuse Treatment. State Methadone Treatment Guidelines (DHHS Publication No SMA 93-1991) Center for Substance Abuse Treatment; Rockville, MD: 1993. [Google Scholar]
- Chatham LR, Hiller ML, Rowan-Szal GA, Joe GW, Simpson DD. Gender differences at admission and follow-up in a sample of methadone maintenance clients. Subst Use Misuse. 1999;34:1137–1165. doi: 10.3109/10826089909039401. [DOI] [PubMed] [Google Scholar]
- Cohen E, Navaline H, Metzger D. High-risk behaviors for HIV: a comparison between crack-abusing and opioid-abusing African-American women. J Psychoact Drugs. 1994;26:233–234. doi: 10.1080/02791072.1994.10472436. [DOI] [PubMed] [Google Scholar]
- Cunningham JA. Resolving alcohol-related problems with and without treatment: the effects of different problem criteria. J Stud Alcohol. 1999;60:693–699. doi: 10.15288/jsa.1999.60.463. [DOI] [PubMed] [Google Scholar]
- Cunningham JA. Remissions for drug dependence: is treatment a prerequisite? Drug Alcohol Depend. 2000;59:211–213. doi: 10.1016/s0376-8716(99)00123-4. [DOI] [PubMed] [Google Scholar]
- Darlington RB. Regression and Linear Models. McGraw-Hill; New York: 1990. [Google Scholar]
- Davis S. Drug treatment decisions of chemically-dependent women. Int J Addict. 1994;29:1287–1304. doi: 10.3109/10826089409047943. [DOI] [PubMed] [Google Scholar]
- Derogatis LR. Brief Symptom Inventory (BSI): Administration, Scoring, and Procedures Manual. Clinical Psychometric Research; Baltimore, MD: 1992. [Google Scholar]
- Dunn LM, Dunn LM. Peabody Picture Vocabulary Test-Revised. American Guidance Service; Circle Pines, MN: 1981. [Google Scholar]
- Faupel CE, Hanke PJ. A comparative analysis of drug-using women with and without treatment histories in New York City. Int J Addict. 1993;28:233–248. doi: 10.3109/10826089309039625. [DOI] [PubMed] [Google Scholar]
- Gerstein DR, Johnson RA, Larison CL, Harwood HJ, Fountain D. Alcohol and Other Drug Treatment for Parents and Welfare Recipients: Outcomes, Costs, and Benefits. U.S. Department of Health and Human Services; Washington, DC: 1997. [Google Scholar]
- Grella CE, Joshi V. Gender differences in drug treatment careers among clients in the National Drug Abuse Treatment Outcome Study. Am J Drug Alcohol Abuse. 1999;25:385–406. doi: 10.1081/ada-100101868. [DOI] [PubMed] [Google Scholar]
- Hser Y, Anglin MD, Booth MW. Sex differences in addict careers. 3. Addiction. Am J Drug Alcohol Abuse. 1987a;13:231–251. doi: 10.3109/00952998709001512. [DOI] [PubMed] [Google Scholar]
- Hser Y, Anglin MD, McGlothin WH. Sex differences in addict careers. I. Initiation of use. Am J Drug Alcohol Abuse. 1987b;13:33–57. doi: 10.3109/00952998709001499. [DOI] [PubMed] [Google Scholar]
- Hser Y, Grella C, Chou CP, Anglin MD. Relationships between drug treatment careers and outcomes: findings from the National Drug Abuse Treatment Outcome Study. Eval Rev. 1998;22:496–519. [Google Scholar]
- Hser Y, Grella C, Hsieh SC, Anglin MD, Brown BS. Prior treatment experience related to process and outcome in DATO. Drug Alcohol Depend. 1999;57:137–150. doi: 10.1016/s0376-8716(99)00081-2. [DOI] [PubMed] [Google Scholar]
- Kearney MH, Murphy S, Rosenbaum M. Mothering on crack: a grounded theory analysis. Soc Sci Med. 1994;38:351–361. doi: 10.1016/0277-9536(94)90405-7. [DOI] [PubMed] [Google Scholar]
- Kline A. Pathways into drug user treatment: the influence of gender and racial/ethnic identity. Subst Use Misuse. 1996;31:323–342. doi: 10.3109/10826089609045815. [DOI] [PubMed] [Google Scholar]
- Kosten TR, Rounsaville BJ, Kleber HD. Ethnic and gender differences among opiate addicts. Int J Addict. 1985;20:1143–1162. doi: 10.3109/10826088509056356. [DOI] [PubMed] [Google Scholar]
- Korbin JE, Coulton CJ, Chard S, Platt-Houston C, Su M. Impoverishment and child maltreatment within African American and European American neighborhoods. Dev Psychopathol. 1998;10:215–233. doi: 10.1017/s0954579498001588. [DOI] [PubMed] [Google Scholar]
- Longshore D, Hsieh SC. Drug abuse treatment and risky sex: evidence for a cumulative treatment effect? Am J Drug Alcohol Abuse. 1998;24:439–451. doi: 10.3109/00952999809016908. [DOI] [PubMed] [Google Scholar]
- Longshore D, Hsieh SC, Anglin MD, Annon TA. Ethnic patterns in drug abuse treatment utilization. J Ment Health Adm. 1992;19:268–277. doi: 10.1007/BF02518991. [DOI] [PubMed] [Google Scholar]
- Longshore D, Hsieh SC, Anglin MD. Ethnic and gender differences in drug users’ perceived need for treatment. Int J Addict. 1993;28:539–558. doi: 10.3109/10826089309039646. [DOI] [PubMed] [Google Scholar]
- Luthar SS, Suchman NE. Developmentally informed parenting interventions: the relational psychotherapy mothers’ group. In: Cicchetti D, Toth S, editors. Developmental Approaches to Prevention and Intervention: Rochester Symposium on Developmental Psychopathology. University of Rochester Press; Rochester, NY: 1999. pp. 271–309. [Google Scholar]
- Luthar SS, Cushing G, Rounsaville BJ. Gender differences among opioid abusers: pathways to disorder and profiles of psychopathology. Drug Alcohol Depend. 1996;43:179–189. doi: 10.1016/s0376-8716(96)01310-5. [DOI] [PubMed] [Google Scholar]
- Meandzija B, O’Connor PG, Fitzgerald B, Rounsaville BJ, Kosten TR. HIV infection and cocaine use in methadone maintained and untreated intravenous drug users. Drug Alcohol Depend. 1994;36:109–113. doi: 10.1016/0376-8716(94)90092-2. [DOI] [PubMed] [Google Scholar]
- McDermott PA, Alterman AI, Brown L, Zaballero A, Snider EC, McKay JR. Construct refinement and confirmation for the addiction severity index. Psychol Assess. 1996;8:182–189. [Google Scholar]
- McLellan AT, Kushner H, Metzger D, Peters R, Smith I, Grissom G, Pettinati H, Argeriou M. The fifth edition of the Addiction Severity Index. J Subst Abuse Treat. 1992;9:199–213. doi: 10.1016/0740-5472(92)90062-s. [DOI] [PubMed] [Google Scholar]
- McMahon TJ, Winkel JD, Luthar SS, Rounsaville BJ. Looking for poppa: parenting responsibilities of men versus women seeking methadone maintenance treatment. 2001 submitted for publication. [PMC free article] [PubMed] [Google Scholar]
- Moise R, Kovach J, Reed BG, Bellows N. A comparison of black and white women entering drug abuse treatment programs. Int J Addict. 1982a;17:35–49. doi: 10.3109/10826088209054608. [DOI] [PubMed] [Google Scholar]
- Moise R, Reed BG, Ryan V. Issues in the treatment of heroin-addicted women: a comparison of men and women entering two types of drug abuse programs. Int J Addict. 1982b;17:109–131. doi: 10.3109/10826088209054613. [DOI] [PubMed] [Google Scholar]
- National Institute on Drug Abuse. Assessing Client Needs Using the ASI: Resource Manual NIH Publication No 93-3620. National Institute on Drug Abuse; Rockville, MD: 1993. [Google Scholar]
- Procidano ME, Heller K. Measures of perceived social support from friends and from family: three validation studies. Am J Community Psych. 1983;11:1–24. doi: 10.1007/BF00898416. [DOI] [PubMed] [Google Scholar]
- Raley RK. Black-white differences in kin contact and exchange among never married adults. J Fam Issues. 1995;16:77–103. [Google Scholar]
- Rosenbaum M. Women on Heroin. Rutgers University Press; New Brunswick, NJ: 1981. [Google Scholar]
- Rosenbaum M, Murphy S. Always a junkie? The arduous task of getting off methadone maintenance. J Drug Issues. 1984;14:527–552. [Google Scholar]
- Rounsaville BJ, Kleber HD. Untreated opiate addicts: how do they differ from those seeking treatment? Arch Gen Psychiatry. 1985;42:1072–1077. doi: 10.1001/archpsyc.1985.01790340050008. [DOI] [PubMed] [Google Scholar]
- Rounsaville BJ, Weissman MM, Kleber HD, Wilber C. Heterogeneity of psychiatric diagnosis in treated opiate addicts. Arch General Psychiatry. 1982;39:161–166. doi: 10.1001/archpsyc.1982.04290020027006. [DOI] [PubMed] [Google Scholar]
- Schuetz CG, Rapiti E, Vlahov D, Anthony JC. Suspected determinants of enrollment in detoxification and methadone maintenance treatment among injecting drug users. Drug Alcohol Depend. 1994;36:129–138. doi: 10.1016/0376-8716(94)90095-7. [DOI] [PubMed] [Google Scholar]
- Sees KL, Delucchi KL, Masson C, Rosen A, Clark HW, Robillard H, Banys P, Hall SM. Methaodone maintenance vs 180-day psychosocially enriched detoxification for treatment of opioid dependence: a randomized controlled trial. J Am Med Assoc. 2000;283:1303–1310. doi: 10.1001/jama.283.10.1303. [DOI] [PubMed] [Google Scholar]
- Singh BK, Williams JS, Singh BB. An examination of extended family residence sharing predisposition in the United States:1973–1989. Marriage Fam Rev. 1998;27:131–143. [Google Scholar]
- Smith IE, Dent DZ, Coles CD, Falek A. A comparison study of treated and untreated pregnant and postpartum cocaine-abusing women. J Subst Abuse Treat. 1992;9:343–348. doi: 10.1016/0740-5472(92)90029-n. [DOI] [PubMed] [Google Scholar]
- Tabachnick BG, Fidell LS. Using Multivariate Statistics. Third. Harper Collins College Publishers; New York: 1996. [Google Scholar]
- Trent K, Harlan SL. Teenage mothers in nuclear and extended households: differences by marital status and race/ethnicity. J Fam Issues. 1994;15:309–337. doi: 10.1177/0192513x94015002009. [DOI] [PubMed] [Google Scholar]
- Wechsberg WM, Craddock SG, Hubbard RL. How are women who enter substance abuse treatment different than men? A gender comparison from the Drug Abuse Treatment Outcome Study. Drugs Soc. 1998;13:97–115. [Google Scholar]
- White L. Coresidence and leaving home: young adults and their parents. Annu Rev Sociol. 1994;20:81–102. [Google Scholar]
- Woodhouse LD. Women with jagged edges: voices from a culture of substance abuse. Qual Health Res. 1992;2:262–281. [Google Scholar]