

Abstract
The relation between perceived racial discrimination and substance use was examined in two studies that were based on the prototype – willingness model (Gibbons, Gerrard & Lane, 2003). Study 1, using structural equation modeling, revealed prospective relations between discrimination and use five years later in a panel of African American adolescents (M age 10.5 at T1) and their parents. For both groups, the relation was mediated by anger/hostility. For the adolescents, it was also mediated by behavioral willingness, and it was moderated by supportive parenting. Study 2 was a lab experiment in which a subset of the Study 1 adolescents (M age = 18.5) was asked to imagine a discriminatory experience, and then their affect and drug willingness were assessed. As in the survey study, discrimination was associated with more drug willingness and that relation was again mediated by anger and moderated by supportive parenting. Implications of the results for research and interventions involving reactions to racial discrimination are discussed.
Keywords: Discrimination, Affect, Substance use
Psychologists have known for some time about the pernicious effects that perceived racial discrimination can have on mental health. Numerous correlational studies have documented relations between self-reports of discriminatory experiences and reports of distress, including anxiety and depression, as well as anger (Banks, Kohn-Wood, & Spencer, 2006; Bynum, Burton, & Best, 2007; Davis & Stevenson, 2006). Of late, the topic has taken on additional significance, as research has emerged linking perceived discrimination with physical as well as mental health problems. In fact, the strength of these relations has led some to conclude that racial discrimination is an important, perhaps primary, contributing factor to the significant disparity in health status that exists between African Americans (Blacks) and European Americans (Whites) in the US (Clark, Anderson, Clark, & Williams, 1999; Krieger, 2000; Mays, Cochran, & Barnes, 2007; Williams, Neighbors, & Jackson, 2003).
The discrimination → physical health relation appears to be both direct and indirect. In the former category, experimental and correlational studies have converged in demonstrating that perceived discrimination is associated with elevated blood pressure, which can lead to cardiovascular problems (Richman, Bennett, Pek, Siegler, & Williams, 2007; Ryan, Gee, & Laflamme, 2006). Other studies have suggested discrimination can affect health indirectly, through its impact on risky and/or unhealthy behavior. For example, discrimination is associated with an increase in aggression in Black adults (Dubois, Burk-Braxton, Swenson, Tevendale, & Hardesty, 2002), as well as Black boys (Simons et al., 2006), and Native Americans (Whitbeck et al. 2001); and aggressive behavior, in turn, increases the risk for injury and trauma (Piko, Kerestes, & Pluhar, 2006; Smith, 2003).
Similar relations have been reported with another type of risky behavior that is more directly associated with health--substance use. These studies have produced a consistent pattern of results: Blacks who report more experience with discrimination are also more likely to report that they use tobacco and alcohol (Bennett, Wolin, Robinson, Fowler, & Edwards, 2005; Landrine, Klonoff, Corral, Fernandez, & Roesch, 2006; Martin, Tuch, & Roman, 2003), and more likely to report lifetime use of marijuana or crack (Borrell, Kiefe, Williams, Diez-Roux, & Gordon-Larsen, 2006). These studies have been cross-sectional, however, which limits both causal inference and assessments of mediation. One study has shown a prospective relation between discrimination and substance use in Black adolescents and their parents. Gibbons, Gerrard, Cleveland, Wills, and Brody (2004) found that the parents' reports of discrimination were directly related to their reports of substance use two years later (T2), and indirectly related to use, through increases in distress, which was operationalized as anxiety and depression. Discrimination was also related to increased stress in the adolescents at T2, and this stress was marginally correlated with their substance use (p = .10); however, the adolescents were only 12 years old at the time, so very little use was reported.
If there is a causal relation between discrimination and substance use, as many suspect, it is important to determine what mediates that relation (e.g., what type of affect or distress). Such information has implications for the development of effective substance use interventions, especially for African Americans and other minorities facing discrimination. More generally, this information is central to an understanding of the impact of discrimination on mental and physical health-- and therefore the issue of health disparities-- as well as the connection between affect and risky behavior. In order to effectively assess mediation of the discrimination → substance use relation, longitudinal and experimental studies are needed.
What Mediates the Discrimination to Use Relation?
Recent research suggests that internalizing reactions (i.e., anxiety and depression), although often elevated by discrimination, may not be the affective response that links discrimination with substance use. Instead, this research, which comes from several different areas, points to externalizing reactions (i.e., anger and hostility) as the operative response. First, several studies have suggested that discrimination is more strongly linked with externalizing behaviors (hostility and anger) than it is with internalizing reactions (anxiety and depression) (Scott & House, 2005). Simons et al. (2006), for example, found that perceived discrimination was associated with violent delinquency among Black boys and that anger, rather than depression or anxiety, mediated this effect. Minior et al. (2003) found that Black adult substance users were much more likely to say they felt angry in response to discrimination than to say they felt ashamed (cf. Nyborg & Curry, 2003; Swim, Hyers, Cohen, Fitzgerald, & Bylsma, 2003).
Second, substance use and abuse appears to be more commonly associated with externalizing than internalizing reactions—although, again, both relations are frequently observed. Krueger's (1999) confirmatory factor analysis of data from the National Comorbidity Study on mental disorders among US adults (N = 8098) produced evidence of three primary factors: phobia, and both internalizing and externalizing reactions. The latter factor comprised both antisocial personality disorder and substance dependence (cf. Krueger et al., 2002). Finally, Terrell, Miller, Foster, and Watkins (2006) reported that Black adolescents who said they got angry in response to discrimination were also more likely to say they drank alcohol.
One reason why externalizing may lead to substance use is because it is associated with risk taking, and heavy substance use is a risky behavior. Both correlational and experimental studies have suggested that risk-taking is related to anger (Lerner & Keltner, 2001), whereas risk avoidance is related to fear and anxiety, as well as sadness (Michael & Ben-Zur, 2007; Raghunathan & Pham, 1999; Rydell et al., 2008). Curry and Youngblade (2006) found that reports of anger were more strongly correlated with risk behavior than were reports of depression (cf. Fite, Colder, & O'Connor, 2006). Hockey, Maule, Clough, and Bdzola (2000) also reported that state and trait anxiety and depression were not consistently related to risk behavior. Finally, studies in social cognition have shown that anger (and not sadness) prompts heuristic processing (Bodenhausen, Macrae, & Hugenberg, 2003; Leith & Baumeister, 1996; Moons & Mackie, 2007), and heuristic processing (see below) has been linked with riskier behavior (Reyna & Farley, 2006; Wang, 2006), perhaps, as some have suggested, because it is associated with less consideration of risk (Johnson, 2005; Trumbo, 1999).
Heuristic Processing and the Prototype/Willingness (Prototype) Model
The current studies use the prototype model to examine the impact of discrimination on the health behavior of Black adolescents (see Gerrard, Gibbons, Stock, Houlihan, & Pomery, 2008; Gibbons et al., 2003; and Gibbons, Gerrard, Reimer, & Pomery, 2006; for further discussion of the model). Briefly, the prototype model presents a dual-processing perspective on health behavior. It maintains that there are two paths to adolescent health risk (e.g., substance use), which involve different types of cognitive processing and have different proximal antecedents. The reasoned path involves analytic processing, which is more deliberative and planful. It reflects the fact that some risk behavior is the result of consideration (e.g., of risk, consequences, subjective norms) and planning--even among younger adolescents (Andrews, Hampson, Barckley, Gerrard, & Gibbons, 2008; Webb, Baer, Getz, & McKelvey, 1996). This path proceeds to health risk through behavioral intention (BI). The social reaction path involves processing that is more heuristic (it is also quicker, and is based more on affect and images). It reflects the fact that much adolescent risk behavior is neither planned nor reasoned. Instead, it is a reaction to situations that provide the adolescent with a risk opportunity. The social reaction path proceeds to use through a second proximal antecedent, behavioral willingness (BW).
BW is defined as an openness to risk opportunity; what an adolescent would be willing to do in different “risk-conducive” circumstances. These situations are usually of a social nature (e.g., a party with drugs; an interested, potential sex partner), but not always (e.g., “You're home alone and you know where your brother's marijuana is…”). Relative to BI, BW involves less contemplation and premeditation about the behavior—i.e., it is more impulsive or reactive and less “reasoned” (Gerrard, Gibbons, Houlihan, Stock, & Pomery, 2008). The two proximal antecedents are usually highly correlated (rs ranging from .25 to .70, depending on age and the behavior; Gibbons et al., 2004). For many adolescents, however, substance use is more reactive than planned, and it involves affect and images more than reasoning (Reyna & Farley, 2006; Verdejo-Garcia, Bechara, Recknor, & Pérez-García, 2007; Wang, 2006). Consequently, BW is usually a better predictor of substance use than is BI until about age 17 or 18 (Pomery, Gibbons, Reis-Bergan, & Gerrard, 2009).
One hypothesis explored in the current studies is that because it involves (negative) affect and heuristic processing (Gibbons et al., 2004), racial prejudice/discrimination should influence behavior via the social reaction path--including BW--more than the reasoned path. In contrast, the deliberation that leads to BI is prompted by factors such as observation of use by parents or older siblings (cf. Ouellette, Gerrard, Gibbons, & Reis-Bergan, 1999). In other words, frequent observation of use induces reasoning (thought) about the behavior and, for some, this leads to a plan and/or expectation to use. Although consistent with the model, however, this hypothesis that parents will affect BI more than BW has not been tested directly. To test these two hypotheses about antecedents to BW and BI, they were both included as predictors of use in the first study.
What Moderates the Discrimination → Use Relation?
The current studies also looked at a factor thought to moderate the relation between perceived racial discrimination and reports of alcohol and drug use: supportive parenting. In a previous study with the same sample used here, Simons et al. (2006) found that a parenting style characterized by warmth and support buffered against discrimination effects: Black boys whose parents were more supportive were less likely to report anger in response to discrimination. Moreover, this (reduced) anger mediated the effect of discrimination on violent delinquency. Brody, Chen et al. (2006) found similar buffering results with regard to the relation between discrimination and conduct problems. More generally, supportive parenting has been associated with less adolescent substance use in a number of studies (e.g., Caldwell et al., 2006). We examined this buffering process in both of the current studies, with the assumption that supportive parenting would buffer against hostile/angry reactions to discrimination, resulting in less willingness to use substances.
Overview
Participants in both studies were members of the Family and Community Health Study (FACHS). FACHS is an ongoing longitudinal study that is examining psychosocial factors, such as perceived racial discrimination and neighborhood risk, that influence the mental and physical health of African American families. Study 1 involved two different sets of analyses. First, Structural Equation Modeling (SEM) was used to examine the relations among discrimination, different types of negative affect, and use over three waves of data (a five year period). Discrimination and affect were measured at T1; at T2, BI and BW were measured (as mediators) with the adolescents, and affect was measured again with the parents; use was assessed at T3 for both family members. Second, regressions examined parenting style as a moderator of the relations between discrimination and both affect and BW for the adolescents.
The following predictions were made. a) Discrimination effects will follow the social reaction path through affect and (for the adolescents) BW to substance use. b) These effects will involve elevated distress (anxiety and depression) and hostility (anger). However, the relation with substance use will be stronger for hostility than the other two; thus, anger will mediate the discrimination → use relation. c) Parental use will affect adolescent use via the reasoned path-- through BI. d) Discrimination effects will be weaker for adolescents whose parents use a supportive parenting style. Analyses controlled for state of residence and neighborhood risk (e.g., substance availability), parents' SES, financial stress, and parenting style, and adolescents' gender and risk-taking tendencies, all of which have been associated with use in previous research. Study 2 was a lab study conducted with a subset of the same FACHS adolescents. It included a discrimination manipulation intended to examine, experimentally, the role of affect in the mediation of the discrimination/substance use relation that was anticipated in Study 1.
Study 1
Method
Participants
At T1, FACHS included a total of 889 families, 475 living in Iowa and 422 in Georgia. Each family had an adolescent age 10 to 12 (M = 10.5; 46% male) and one primary caregiver (parent), defined as a person living in the same house who was primarily responsible for the child's care. Of the 889 families, 779 remained in the panel at T2 (retention rate = 88%); 767 (86%) remained at T3. Mean age of the parents at T1 was 37. Most (84%) of them were the adolescent's biological mother; 93% were female; 44% were single parents. Their education levels ranged from less than high school diploma (19%) to a BA/BS or graduate degree (9%); income levels also varied considerably. A total of 676 adolescents (308 males) and their parents answered enough questions at all three waves to be included in the analyses.
Sampling Strategy and Recruitment
Unlike many studies of African Americans, which have focused on inner city areas, FACHS recruited participants from the full range of SES levels in rural communities, and small metropolitan and suburban areas. Families were enumerated from lists of all families in a given community with a 5th grade African American child. The lists were compiled by community coordinators in Georgia and school officials in Iowa. Recruitment sites varied on many characteristics including racial composition and economic level. Poverty rates in the neighborhoods sampled ranged from less than 20% to more than 50% of the families. Of those families contacted, 72% agreed to participate; those who declined most often cited the length of the interview (> 3 hours, total) as the reason (for more description of the FACHS sample and its recruitment, see Brody et al., 2001; Cutrona, Russell, Hessling, Brown & Murry, 2000; Simons et al., 2002; Wills, Gibbons, Gerrard, & Brody, 2000).
Interview Procedure
The interviewers were African American, most of whom lived in the communities in which the study took place. The interviews required two visits to the family's home or a nearby location, each about 90 minutes, with two interviewers. Adolescents and their parents were interviewed at the same time in separate rooms. The computer-assisted personal interview (CAPI) technique was used, which included two psychiatric diagnostic assessments: The Diagnostic Interview Schedule for Children (DISC IV; Shaffer et al., 1993) and the Composite International Diagnostic Instrument (UM-CIDI: Kessler, 1991) for the parents. For their participation, at each wave, parents received $100 and adolescents received $70. T2 occurred about 22 months after T1; T3 occurred about 36 months after T2 (M adolescent age: T2 = 12.4; T3 = 15.6). The procedure and interviews were the same at T1 and T2, but several minor changes were implemented at T3; e.g., adolescents were given a keypad to enter their responses (because of sensitive questions), and their compensation was increased to $80.
Measures: Adolescents
T1 discrimination
Adolescents completed 13 items from a revised version of the Schedule of Racist Events (Landrine & Klonoff, 1996). This measure described various discriminatory events and asked participants to indicate how often they had experienced each event in the past; e.g., “How often has someone said something insulting to you just because you are African American?” (from 1 = never to 4 = several times; α = .67).1 The scale has been used in a number of studies of discrimination. As with most of the latent constructs, for the SEM, these items were randomly parceled into three groups, each of which was used as an indicator of the latent construct (cf. Coffman & MacCallum, 2005).
T1 distress and anger
The DISC IV included 12 items measuring anxiety, e.g., “In the last year, was there a time when you… worried about whether other people liked you?” and 22 items measuring depression: e.g., ““In the last year, was there a time when you… often felt sad or depressed?” The 34 items (all yes/no) were combined into an overall measure (α = .85). There were also four anger items, which asked how often during the last year the adolescent: lost his/her temper, felt grouchy or annoyed, felt unfairly treated, and got mad (from 0 = never to 4 = nearly every day; α = .72).
T2 BW and BI
BW and BI were measured for alcohol and drug use, as in previous studies. For BW, participants were presented with a social scenario for each substance, which described an opportunity to use the substance (e.g., alcohol/marijuana available at a party). These were followed by the stem: “How willing would you be to…drink one drink… have more than one drink?” (for alcohol), and “… take some and use it… use enough to get high” (for drugs) (α = .75). There was also a BI and a behavioral expectation item for each substance, which were combined into a BI index; e.g., “Do you plan to use drugs in the next year?” from 1 = do not plan to to 4 = plan to; and “How likely is it that you will use drugs in the next year?” from 1 = definitely will not to 4 = definitely will (α = .72).2
T3 substance use
There were three questions about alcohol use and two questions about marijuana use lifetime and in the last year (yes/no); these seven questions were summed.
Measures: Parents
T1 and T3 substance use
Our focus was on problematic substance use—i.e., more than occasional drug use and problematic (as opposed to “social”) drinking. The CIDI contained four questions about experiencing problems due to alcohol use (lifetime; yes/no); those were: problems at work, being arrested, fighting, and being harmed while under the influence. There was also a list of 22 drugs, including marijuana, heroin, mescaline, and crack. Participants indicated if they had used each more than five times. The 26 items were summed to create an overall score (0 to 26).3
T1 discrimination
Parents also completed the Schedule of Racist Events. Their version was very similar to that used with the adolescents (α = .92).
T1 and T2 distress
The distress items began: “During the past week, how much have you felt..?” followed by five depression items [hopeless, depressed, discouraged, worthless, like a failure] and three anxiety items [tense, keyed up/on edge, uneasy], each from 1 = not at all to 3 = extremely. These were combined into an overall distress measure (α = .69).4
T1 and T2 Hostility
Seven types of anti-social behaviors (called hostility here) were measured in the CIDI, including physical violence, stealing, and reckless driving (e.g., “Since age 15, have you been in physical fights?” yes/no).5 There were several questions for each type of behavior, a total of 35 items. The sum of the 35 was used as the measure of hostility.
T1 supportive parenting
Responses from the adolescents and parents were combined to create a supportive parenting measure similar to that used in previous FACHS studies (Brody et al, 2001; Simons et al., 2006). Adolescents completed a 9-item measure of perceived parental warmth; e.g., “How often during the past 12 months did (parent) tell you she loves you” from 1 = never to 4 = always; plus two communication items (e.g., “How often do you talk to (parent) about things that bother you?”). Parents completed a 6-item measure of consistent discipline (e.g., “When you tell [adolescent name] to stop doing something and [adol.] doesn't stop, how often do you discipline [adol.]?” (same scale). Parents and adolescents both responded to seven questions about the parent's inductive reasoning (e.g., for the parents: “How often do you give reasons to [adol.] for your decisions?”), and their use of problem solving (e.g., “When you and [adol.] have a problem, how often can the two of you figure out how to deal with it?”). Adolescents answered slightly re-worded versions of the same seven questions: Adolescent and parent scores were standardized and added together (α = .84).
Covariates
Parents completed measures of SES (education and income), financial stress (6 items; e.g., difficulty paying for…food, bills, clothing; α = .82), and environmental risk (7 items on crime, gangs, and selling of drugs in their neighborhood; α = .90). In addition, the adolescents completed a 6 item measure of risk-taking tendency (adapted from Eysenck & Eysenck, 1977; e.g., “You enjoy taking risks” “You would enjoy fast driving” α = .58). These measures, which have been linked with substance use in previous research, plus supportive parenting, state,6 and adolescent gender were included as covariates in the SEM. Parenting was also used as a moderator in separate analyses assessing the buffering hypothesis (see below).
Results
Means and Correlations
Table 1 presents Ms and SDs for all of the measures, and for illustration purposes, percentages of respondents at three different levels: low (or none), medium, and high.7 Table 2 includes the correlations. The percentage of parents reporting some drug use and/or alcohol problems increased from 25% to 34% from T1 to T3. There was virtually no adolescent use at T1 (92% said none, 7% said once), so it was not included in the SEM; 41% reported some use at T3. For hostile behavior, the modal response was none at both T1 (44%) and T2 (52%). High levels of hostility (4 or more behaviors) were reported by 24% of the parents at T1 and 17% at T2. About half (53%) of the parents reported more than occasional experiences with discrimination; surprisingly, 22% of the adolescents also reported more than occasional experiences with discrimination at T1 (age 10 or 11).
Table 1. Ms, SDs, and Percentages of Levels for Variables (Study 1).
| Low(None) (%) | Medium (%) | High (%) | Ms | SDs | |
|---|---|---|---|---|---|
| Par 1 Use | 75 | 18 | 7 | .57 | 1.55 |
| Par 1 Disc | 47(8) | 41 | 12 | 26.93 | 9.57 |
| Par 1 Host | (44) | 29 | 24 | 2.41 | 2.92 |
| Par 1 Dep | 65(41) | 25 | 10 | 1.28 | .37 |
| Par 1 Anx | 61(40) | 17 | 22 | 1.44 | .48 |
| Par 2 Host | (52) | 31 | 17 | 2.05 | 2.77 |
| Par 2 Dep | 71(52) | 19 | 10 | 1.23 | .34 |
| Par 2 Anx | 69(52) | 15 | 16 | 1.35 | .45 |
| Par 3 Use | 67 | 26 | 8 | .74 | 1.73 |
| Adol 1 Disc | 78(10) | 20 | 2 | 21.18 | 6.86 |
| Adol 1 Dep | 39(12) | 38 | 23 | 5.97 | 4.71 |
| Adol 1 Anx | 41(13) | 35 | 24 | 3.58 | 2.69 |
| Adol 1 Anger | 82(71) | 10 | 8 | 1.14 | 2.31 |
| Adol 1 Use | 99(89) | 1 | - | .11 | .42 |
| Adol 2 BW | 85 | 7 | 8 | 4.30 | .86 |
| Adol 2 BI | 83 | 8 | 9 | 4.32 | .84 |
| Adol 3 Use | 59 | 24 | 17 | .95 | 1.41 |
Note. Percentage reporting none or zero for each of the variables (if different from Low) is included in the parentheses. Parenting was reported by both the parent and the adolescent. Par = parent,
Adol = adolescent, Par Use = drugs and alcohol problems, Adol Use = drugs and alcohol, Disc = discrimination, Host = hostility, Dep = depression, Anx = anxiety, BW = behavioral willingness, BI = behavioral intention, Parenting = supportive parenting (standardized).
Table 2. Correlations for Major Variables for Parents and Adolescents (Study 1).
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | 18 | 19 | 20 | 21 | 22 | 23 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Parent | |||||||||||||||||||||||
| 1 Par 1 Use | - | ||||||||||||||||||||||
| 2 Par 1 Disc | .24 | - | |||||||||||||||||||||
| 3 Par 1 Host | .44 | .23 | - | ||||||||||||||||||||
| 4 Par 1 Dep | .12** | .09* | .17 | - | |||||||||||||||||||
| 5 Par 1 Anx | .13 | .08* | .18 | .61 | - | ||||||||||||||||||
| 6 T1 Parenting | -.14 | - | -.12** | -.17 | -.15 | - | |||||||||||||||||
| 7 Par 2 Host | .34 | .22 | .53 | .17 | .11** | -.12** | - | ||||||||||||||||
| 8 Par 2 Dep | .14 | .10* | .18 | .46 | .35 | -.12** | .24 | - | |||||||||||||||
| 9 Par 2 Anx | .11** | .10* | .15 | .34 | .38 | -.14* | .22 | .65 | - | ||||||||||||||
| 10 Par 3 Use | .78 | .24 | .36 | .09* | .11** | -.11** | .35 | .15 | .14 | - | |||||||||||||
| 11 Par1 NR | .11** | - | - | .22 | .12** | -.10* | .10** | .14 | .09* | - | - | ||||||||||||
| 12 Par1 SES | - | .25 | -.08* | -.15 | - | - | -.11* | -.14 | - | - | -.23 | - | |||||||||||
| 13 Par1 Fin Str | .10* | - | .16 | .35 | .20 | -.11** | .18 | .18 | .14 | - | .27 | -.41 | - | ||||||||||
| 14 State | .23 | .42 | .15 | - | - | - | .20 | - | - | .23 | - | .12** | - | - | |||||||||
| Adolescent | |||||||||||||||||||||||
| 15 Adol 1 Gender | - | - | - | - | - | - | - | - | - | - | .08* | - | - | - | - | ||||||||
| 16 Adol 1 Disc | - | .14** | - | .13** | .12** | - | - | .09* | - | - | .13** | -.10* | .11** | .17 | - | - | |||||||
| 17 Adol 1 Risk | - | - | - | - | - | -.21 | - | - | - | - | - | - | - | .12** | - | .20 | - | ||||||
| 18 Adol 1 Dep | .09* | .19 | - | .10** | - | -.11** | - | - | - | .09* | .10** | - | .11** | .22 | - | .29 | .13 | - | |||||
| 19 Adol 1 Anx | - | .11* | - | .11** | .09* | -.08* | - | - | - | - | .10* | - | .11** | .15 | - | .30 | .12** | .68 | - | ||||
| 20 Adol 1 Anger | - | .15 | - | - | - | -.10* | .09* | - | - | - | - | - | - | .14 | - | .25 | .13 | .41 | .35 | - | |||
| 21 Adol 2 BW | - | - | - | - | - | - | .11** | - | - | .09* | - | - | - | - | .11** | .08* | .11** | .09* | .10** | .12** | - | ||
| 22 Adol 2 BI | .13 | - | - | - | - | - | - | .08* | - | .12** | - | - | - | - | .11** | - | .11** | - | - | .08* | .69 | - | |
| 23 Adol 3 Use | .08* | .10* | .10* | - | - | - | .09* | - | - | - | - | - | - | .10* | - | .11** | - | .17 | .09* | .13 | .28 | .18 | - |
Note. N = Pair-wise deletion. Only significant rs are presented.
p < .05,
p < .01, all other rs significant at p < .001. Italics = control variables. Par = parent, Adol = adolescent, Par Use = drinking problem & drug use for parent, Adol Use = drinking & drug use for target, Disc = discrimination, Host = hostility, Dep = depression, Anx = anxiety, NR = neighborhood risk, Parenting = supportive parenting style (from parent and adolescent responses), Risk = risk-taking, BW = behavioral willingness, BI = behavioral intention, Fin Str = financial stress, Gender: 0 = male; 1 = female, State: 0 = GA; 1 = IA.
SEM: Measurement Model
A confirmatory factor analysis (CFA) using full information maximum likelihood (FIML) estimation was conducted to determine if the indicators loaded on the constructs as expected. The “count” variables (parent hostility and use) plus parenting were specified as manifest constructs; the other nine constructs were specified as latent. The CFA with all 13 constructs correlated provided a good fit to the data: χ2 (272) = 330.49, p = .01; Root Mean Square Error of Approximation (RMSEA) = .018; Comparative Fit Index (CFI) = .99. All but one standardized factor loadings were > .50.
SEM: Full Model
Mplus
Version 3.11 (Muthén & Muthén, 2007) with FIML was used for the SEM. Paths were specified in the model (see Fig. 1) according to hypotheses and previous research in the FACHS project.8 Nonsignificant paths were trimmed (there was only one: parents' T2 distress → T3 use). Modification indices were used to identify nonspecified paths. There were three, all of which involved parent hostility: T1 hostility to T3 adolescent use, T2 hostility → T2 adolescent BW, and T1 parent use → T2 hostility (see description below). The full model fit the data well: χ2 (469, N = 676) = 650.39, p < .001; Tucker-Lewis Index (TLI) = .97; CFI = .98; RMSEA = .024. For T3 substance use, variance explained was: parent R2 = .61; adolescent R2 = .18.
Figure 1.
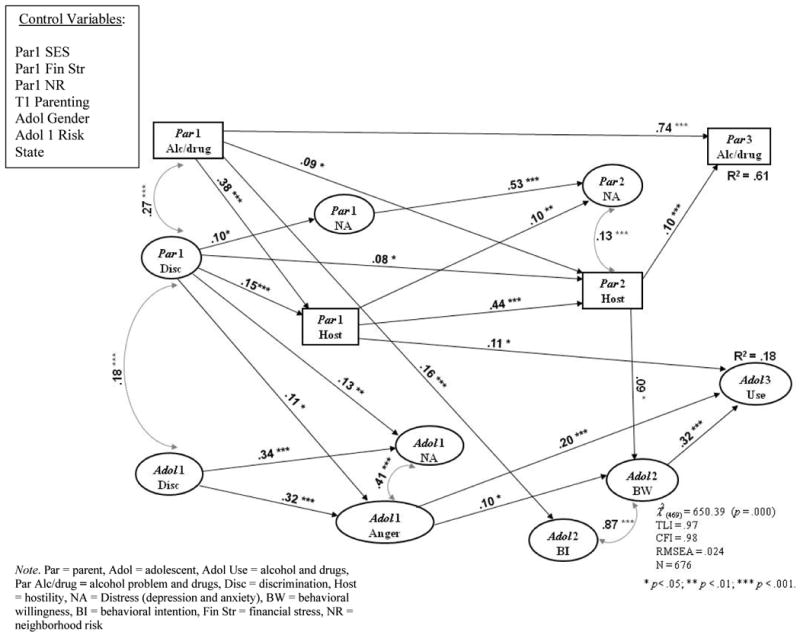
SEM full model (Study 1).
Correlations
Several correlations among the exogenous constructs and controls are worth noting. Parents' use at T1 was positively correlated with their financial stress, discrimination, and neighborhood risk, and negatively correlated with their parenting (all ps < .05). Parents' discrimination was correlated with their child's discrimination (p < .01), and it was strongly correlated with their substance use at T3, five years later (r = .24, p < .001). Adolescents' T1 discrimination was positively correlated with their risk-taking (p < .001), and it was also correlated with their use five years later (r = .11, p < .01).
Mediation and outcome, Parents
T1/T2 correlations (i.e., stability) of both hostility and distress were high for the parents (βs ≥ .44, ps < .001), and the stability of their use was very high (β = .74, p < .001). In spite of the high stability and the strong relation at T1 between hostility and discrimination, T1 discrimination predicted an increase in hostility at T2, as did T1 use (ps < .05). The path from T1 discrimination to T2 distress (i.e., change in distress), which was significant in previous analyses (Gibbons et al., 2004), was no longer significant. The same was true for the path from T2 distress to T3 use, which had been significant (p < .001), but was replaced by the T2 hostility to T3 use path (β = .10, p < .001). As expected, the total indirect effect of T1 discrimination on use was significant (p < .01). Looking at specific indirect paths from discrimination to T3 use (calculated separately by Mplus), the path from discrimination through T1 and T2 hostility to use was significant (z = 2.61, p < .01); and the indirect path to use from T1 discrimination through T2 hostility (i.e., change in hostility) was marginal (z = 1.88, p = .06).
Mediation and outcome, Adolescents
Adolescent distress and anger were correlated at T1 (p < .001), and both of them were correlated with discrimination (both ps < .001). However, T1 distress was not associated with any other construct. In contrast, T1 anger was directly associated with both T2 BW (p < .05) and with use at T3--five years later (p < .001). The overall indirect effect of T1 discrimination on use at T3 was significant (z = 3.30, p = .001). The specific indirect path from discrimination to T3 use through anger was significant: z = 3.02, p < .003; as was the path through T1 anger and then T2 BW: z = 1.97, p < .05. Parent T1 hostility was directly related to adolescent T3 use (p < .05), whereas Parent T2 hostility was directly related to adolescents' T2 BW (p < .05). T2 BW and BI were strongly correlated (p < .001), but when both were in the model, only BW produced a path to use three years later (β = .32, p < .001). Finally, as predicted, parent's T1 use was directly (positively) related to the adolescent's T2 BI (β = .16, z = 3.94, p < .001), but not their BW.
Alternative Models
The following modifications were tried with the SEMs to compare the hypothesized model with other possible models. For the parents: a) separating distress into its two components, anxiety and depression, and then specifying paths from each one to the outcome (use) directly and also through hostility; and b) specifying a path from distress to use instead of hostility to use. Because discrimination was not as strongly related to either anxiety or depression as it was to hostility, and because neither type of distress predicted outcome, these models did not produce evidence of an effect of (T1) discrimination on outcome. In none of the models was the indirect path from discrimination to use through anxiety and/or depression significant (unless hostility was taken out of the model). The same procedure was tried with the adolescents. Neither anxiety nor depression predicted BW, nor did they predict outcome (use) when anger was in the model. In sum, the pattern for the parents and their children was consistent with the belief that it is anger or hostility more than anxiety and depression that links discrimination with substance use.
Moderation by Supportive Parenting
To examine the extent to which the adolescents' reactions to discrimination were buffered by the parenting they received, regression analyses were conducted in which their T1 anger and T2 BW were regressed on the relevant predictors in the SEM: adolescent and parent discrimination, parenting, and the adolescent Discrimination× Parenting interaction. The anger regression revealed main effects of both the adolescents' and their parent's perceived discrimination (as in the SEM; both ps < .005), and parenting (t = -2.30, p = .02), as well as the anticipated adolescent Discrimination× Parenting interaction (t = 2.00, p < .05). The interaction pattern reflected buffering: there was less effect of discrimination on anger for those adolescents whose parents used supportive parenting (cf. Simons et al., 2006). The same buffering pattern emerged for T2 BW (see Fig. 2): Parenting again predicted negatively: t = -3.48, p < .001; and the Discrimination× Parenting interaction was significant: t = -3.03, p < .003. When the same analysis was run with T3 Use as a criterion, T1 discrimination predicted use: t = 2.89 (p < .004), and the interaction was marginal: t = 1.85 (p = .06), but it also reflected buffering. Thus, for anger, BW, and, to a lesser extent, use, parenting style buffered against the discrimination effects. Regressions predicting distress did not produce evidence of buffering, however, as the interaction was not significant (p > .20).
Figure 2.
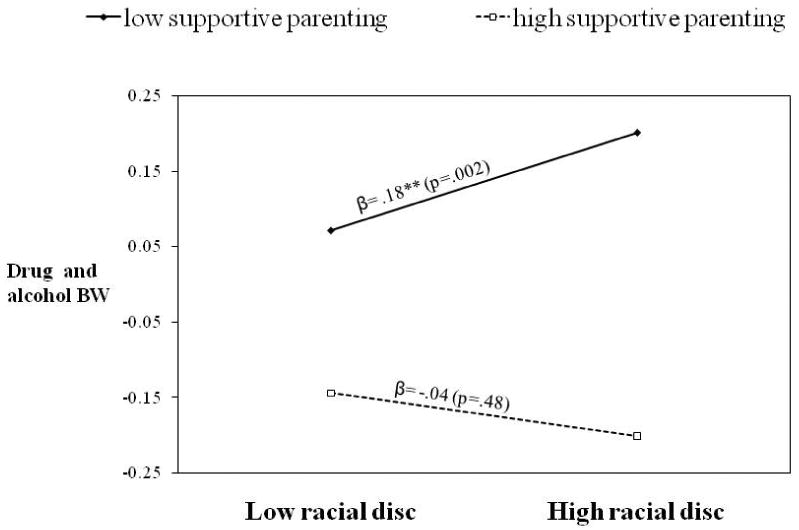
Time 1 discrimination (self-report) predicting Time 2 drug and alcohol behavioral willingness moderated by Time 1 parental support (Study 1).
Discussion
Discrimination, Affect, and Use
Perceived discrimination had an impact on both the parents and their children. For the parents, reports of discrimination were related to their distress and hostility at T1. Discrimination also predicted an increase in their hostility at T2, which then predicted an increase in use three years later. In fact, just as the parents' T1 discrimination had the strongest zero-order correlation with their T2 use of any measure of stress reported in Gibbons et al. (2004a), in the current study, the correlation with T3 use was stronger for parents' T1 discrimination (r = .24, p < .001) than any other risk measure in either T1 or T2, including neighborhood risk; negative life events; low SES; and financial, relationship, and job stress (all 12 rs at T1 and T2 < .15). Moreover, the effects of discrimination on affect and use existed controlling for these other measures, some of which had their own relation with use and/or affect.
The adolescents' reactions to discrimination were very similar to those of their parents. Their own discriminatory experiences and those of their parents both had the same exacerbating impact on their distress and anger. Moreover, for some adolescents, that anger translated into subsequent use. In short, discrimination appears to be an important predictor of stress and use that works independently of other stressors. It also appears that anger/hostility is the central construct that mediates this strong relation between discrimination and use. For the parents, hostility was the factor that linked prior discrimination experiences with subsequent use. For their children, it was anger that was prospectively associated with both their willingness to use and their actual use—assessed five years after the anger measure—taking into account their risk-taking tendencies, neighborhood risk, and their parents' use. Finally, as expected, the impact of discrimination was buffered by supportive parenting. Adolescents whose parents offered more support were less likely to report feeling angry and to report drug and drinking willingness if they had experienced discrimination.
Willingness and Intention
BW and BI were highly correlated for the adolescents; however, as expected, the prospective relation with T3 use was stronger for BW than it was for BI.9 Moreover, the antecedents of BW and BI differed. Anger was more strongly related to BW, which is consistent with the heuristic nature of the social reaction path. Theoretically, given that we were controlling for its relation with BI, the variance left in BW that relates to use should involve components of the social reaction path—affect being a prime example. The relation between adolescent BW and their parents' hostility was not anticipated, but it is consistent with this general perspective. It suggests that the adolescents had an affective response to observing their parents' hostile actions and, for some, that affect (like their own anger) translated into a willingness to use substances. Finally, as expected, parental use was related to their child's BI, although more so their (behavioral) expectation than their intention. This finding is consistent with the assumption that BI and behavioral expectation both involve some contemplation of the behavior and its consequences, in this case, apparently contemplation brought on by (perhaps years) of observation of parents' use (Gibbons et al., 2007).
Study 2
Study 1 showed that early experience with discrimination (by age 11) predicted adolescent substance use five years later, and that anger appeared to be the most important mediator of that relation. There were, however, some aspects of the first study that limit our ability to conclude that anger is the primary factor. First, there was no direct measure of anger for the parents; instead, we assumed that their hostility reflected their anger. Second, anger was directly related to the adolescents' BW at T2 and their use at T3; but they were only 12 or 13 at T2 and 15 or 16 at T3, so there was not much BW or use reported. Third, although prospective, this study, like other studies of discrimination and substance use, was correlational. Thus, we cannot rule out the possibility of some unidentified third variable predictor (related to discrimination, anger, and BW) that we did not measure being responsible for the effects, or the possibility that anger or BW lead to discrimination rather than the reverse.
To increase confidence in our belief that it is anger that is central, a study was needed in which different affective reactions to discrimination, as well as its impact on BW, were examined experimentally in an older sample. That was the purpose of Study 2, which included a subset of the FACHS adolescents from Study 1. Some of them were asked to envision being in a situation that involved racial discrimination. The primary prediction was that envisioning discrimination would elevate BW and exacerbate affect—i.e., anger, anxiety, and depression—but it would be anger that mediated the anticipated effect of discrimination on BW. We also expected BW would be higher for those with some history of use (i.e., we did not expect to “create” drug willingness in the lab for those who were not users). Finally, we again looked at parenting style as a moderator of the effects of (manipulated) discrimination on both BW and affect, expecting the same pattern of results as in Study 1.
Method
Participants
Letters were sent to 175 adolescents from the Iowa FACHS sample asking for their participation in a lab study. Because we were interested in studying substance use, we oversampled adolescents who had indicated in an earlier wave of FACHS that they had used drugs or drank heavily. Of these 175, 149 agreed to participate, and 139 completed the study.10 However, only 116 of their parents provided data needed for the supportive parenting variable; these 116 adolescents comprised the sample (75 females; M = 18.5 years old).
Procedure
The study was conducted by two African American experimenters. Participants were told the study was designed to examine health relevant attitudes and behaviors, and also how African Americans respond to stressful and successful experiences. They were randomly assigned to one of three visualization scenarios, which were presented to them on a computer screen. In each case, they were asked to imagine being in the situation and then think about how they would react to it. They responded on the computer and then verbally (those responses were recorded for a different study). All three scenarios were job situations. One involved racial discrimination, including racial insults and unfair treatment from a boss (adapted from King, 2005; cf. Yoo & Lee, 2008). The second also involved job stress, but it was unrelated to racial discrimination—i.e., falling behind at work due to a sick co-worker and equipment problems. The third scenario involved a non-stressful work experience: finding an address while working as a delivery person. Afterwards, participants were asked how stressful they would find the experience. They then completed the following measures in this order: current mood, a word association task (intended for another study), a measure of drug willingness, another word association task, and then, finally, the drug use measure . Participants were then debriefed and paid $105 for their time (including travel).
Measures
Parenting and mood
Some of the variables used in the analyses came from T1 of FACHS, and some were collected during the lab study. The same measure of T1 parental support used in Study 1 was again used as a moderator. For mood, participants were presented with 15 negative emotion words (in random order) intended to assess anger, depression, and anxiety, and then asked to indicate whether they would feel each emotion in response to the visualized scenario (0 = no; 1 = yes). A principal components analysis of the 15 items revealed three factors with eigenvalues > 1.4, explaining 53% of the variance; all but three factor loadings were > .59. Factor 1, labeled depression, included the emotions: lonely, sad, hopeless, and depressed; Factor 2, labeled anger, included bitter, aggressive, hostile, and angry; Factor 3, labeled anxiety, included tense, stressed, frustrated, and worried. The other three items (helpless, fearful, and discouraged) did not load clearly, and so were dropped.
BW and drug use
Drug willingness was measured as in Study 1, with a description of a hypothetical scenario. Due to the older age of the sample, a third (higher) risk option was added: buy some to use later, and the scale was extended to 7 points (from not at all to very; α = .85). Participants also reported how often they had used marijuana, crack or cocaine, and other illegal drugs in the past six months (three items, from 1 = not at all to 4 = a lot). Because it was assumed that the impact of discrimination on drug cognitions (e.g., drug BW) would vary as a function of previous drug experience, this drug use measure was used to divide participants into a nonuser group (i.e., used once or twice or less) and a user group (Ns = 35 and 81, respectively).
Results
Means and Correlations
Means
Table 3 presents Ms and correlations for the primary measures. Of the 81 users, 75% reported using marijuana; 19% reported using at least one other illegal drug. Initial 3× 2 (Condition× Previous Use) ANOVAs were conducted on the primary measures. A main effect of Condition on the measure asking how stressful participants would find the experience (F[2, 113] = 18.31, p < .001) reflected the fact that stress was higher in the Discrimination (Disc) Condition (M = 3.23) than in both the Non-discrimination stress (Nondisc) Condition (M = 2.81; t = 2.34, p = .02) and the Control Condition (M = 2.17; t = 5.99, p < .001), and it was higher in Nondisc than Control (p < .001). There was also a main effect of Condition on the anger measure: F(2,110) = 3.97, p = .02. The pattern was such that the Disc condition mean (1.50) was significantly higher than each of the other two means (Nondisc = 1.30, Control = 1.29; both ts > 2.50, ps ≤ .01), whereas the other two were very similar (t < .2). The same pattern emerged on the BW item among the users (there was very little BW among nonusers): BW was higher in the Disc than in the Nondisc condition (Ms = 2.87 vs. 1.97, t = 2.58, p = .01) and it was marginally higher in the Disc than the Control condition (M = 2.26, t = 1.80, p = .07); once again, Nondisc and Control did not differ (t = .85, p > .39). Consequently, to simplify analyses, because the Nondisc and Control conditions were very similar on all of the primary measures, they were combined into a single Nondisc group (Ns: Nondisc = 76; Disc = 40).
Table 3. Correlations, Means, and SDs of Variables (Study 2).
| 1. | 2. | 3. | 4. | 5. | 6. | ||
|---|---|---|---|---|---|---|---|
| 1. Use | - | ||||||
| 2. Anger | .05 | - | |||||
| 3. Depression | -.07 | .47*** | - | ||||
| 4. Anxiety | -.06 | .36*** | .48*** | - | |||
| 5 BW | . 43*** | .35*** | .09 | .07 | - | ||
| 6. Supportive Parenting | .00 | -.10 | -.03 | -.07 | -.03 | - | |
| Mean | .70 | 1.36 | 1.24 | 1.61 | 1.98 | 0.00 | |
| SD | - | 0.36 | 0.28 | 0.37 | 1.40 | 1.00 |
Note. N = 116.
p < .05
p < .01
p < .001. Use = previous use (0 = no, 1 = yes); Scales: Anger, Depression, and Anxiety = 1-2; BW = 1-7; Supportive parenting is standardized.
Correlations
As expected, BW correlated more highly with anger (r = .35, p < .001) than it did with either anxiety or depression (rs = .079 and .09; NS); in both cases, the differences in magnitude of the correlations were significant (zs > 2.77, ps < .005).
Effect of Discrimination on Mood and BW: ANOVAs
Mood
To directly assess whether type of scenario differentially influenced mood levels across the three types of mood, a 2× 2× 3 (Condition× Previous Use× Type of Mood) repeated measures ANOVA on the three mood scales revealed the expected main effect of Condition, as there was more overall negative affect reported in the Disc than the Nondisc conditions: F(1,112) = 4.97, p < .03. There was also a large effect of mood type: (F = 48.38, p < .001), as well as a marginal Condition× Mood interaction (p = .08), and a significant Condition× Mood× Use interaction (F = 4.08, p < .05). The mood main effect reflected the fact that reports of anxiety were much higher than reports of either of the other two mood states (both ts > 5.5, ps < .001). Also, anxiety was not differentially affected by Condition (it was high in all conditions; Condition main effect: F = .51, NS), and it was not correlated with any of the other measures (ps > .30), except anger and depression (see Table 3). Consequently, although the 3-way interaction was in the predicted direction (the highest mood mean was anger reported by users in the Disc Condition),11 anxiety was dropped from the list and subsequent analyses were conducted on just depression and anger (see Table 4).
Table 4. Anger, Depression, and Drug BW as a function of condition and level of previous substance use (Study 2).
| Condition | Nondiscrimination (n = 77) | Discrimination (n = 39) | ||||
|---|---|---|---|---|---|---|
| Variable | Anger | Depression | BW | Anger | Depression | BW |
| Substance Use | ||||||
| Lo (n = 35) | 1.26 (.28) | 1.18a (.28) | 1.06d (.22) | 1.46 (.39) | 1.41a, e, i (.30) | 1.10f (.21) |
| Hi (n = 81) | 1.30b (.35) | 1.23i (.26) | 2.13c, d (1.35) | 1.52b (.36) | 1.21e (.28) | 2.87c, f (1.74) |
|
|
|
|
|
|
|
|
| Marginals | 1.29g (.33) | 1.22 (.26) | 1.82 (1.24) | 1.50g, h (.37) | 1.28h (.30) | 2.28 (1.65) |
Note. Standard deviations are in parentheses. Scales: Anger and Depression = 1-2; BW = 1-7. Ns: for low use, nondiscrimination, n = 22; for high use, nondiscrimination, n = 55; for low use, discrimination, n = 13; for high use, discrimination, n = 26.
Significant difference between the cell means at p ≤ .05
Significant difference between the cell means at p ≤ .01
Significant difference between the cell means at p ≤ .001
Anger vs. depression
There were main effects of Mood type and Condition: anger was higher than depression (F = 14.36, p < .001), and negative affect overall (i.e., depression and anger) was elevated in the Disc Condition: F = 7.67, p < .007. The Condition× Mood interaction (see marginals in Table 4) was not significant (p < .14), but the anticipated differences were: the mean for anger in the Disc condition (M = 1.50) was higher than the anger mean in the Nondisc condition and the depression mean in the Disc condition (both ts > 2.80, ps < .005). The Mood× Condition× Use interaction was only marginal: F = 3.48, p = .07; nonetheless, we proceeded with (planned) analyses on reports of anger and depression. As the Table shows, anger was most elevated among users in the Disc condition; their anger was higher than that of the Nondisc group (p < .01), and much higher than their reported depression (p < .001). That was not the case for the nonusers in the Disc Condition, however: their depression was elevated relative to each of the other three groups (all ps ≤ .05), and it was almost as high as their anger. In short, all participants tended to respond to the discriminatory experience by reporting anger, but there was some evidence that nonusers also responded with increased depression.
BW
BW was much lower among nonusers than users (p < .001), and there was no difference due to Condition among the nonusers (p > .90; see Table 4). As expected, however, BW was higher among the users in the Disc Condition than any other group (all three ps ≤ .01).
Mediation of Discrimination Effects on BW by Anger
To assess the primary hypothesis—mediation of the effect of discrimination on BW by anger--a bootstrapping procedure (Preacher, Rucker, & Hayes, 2007) was used. The indirect effect of condition on drug BW through reported anger was significant: point estimate of indirect effect = .255 with a 95% percentile confidence interval of .072 to .537. Similar procedures were run with depression and anxiety, but neither measure was a significant mediator. Further illustration of the anger mediation effect can be seen in Fig. 3, which presents results of the regression-based method described by Baron and Kenny (1986). This indicates that 50% of the effect of Condition on BW was mediated by anger. In short, both methods indicate that anger, not depression, mediated the effect of discrimination on BW.
Figure 3.
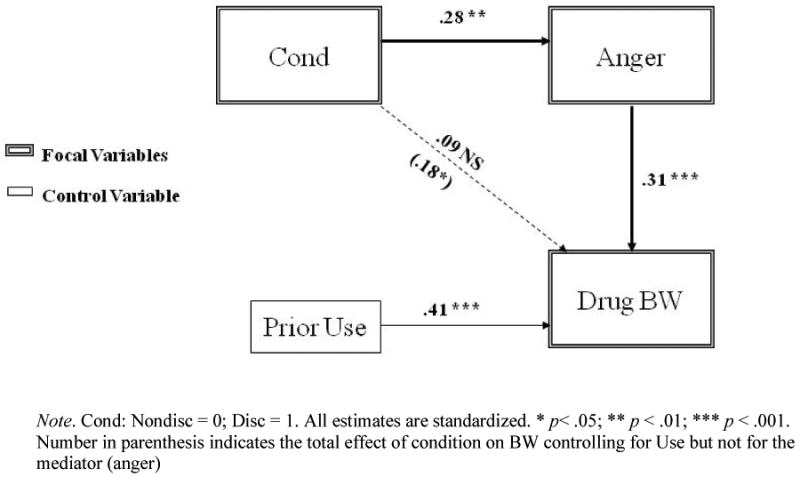
Mediation of the effect of discrimination condition on drug behavioral willingness by anger (Study 2).
Moderation of Discrimination Effects by Parenting: Buffering
Mood ANOVA
To examine the effect of parenting on mood reactions (depression vs. anger) to the discrimination scenario, an ANOVA was first conducted that included the parenting measure, as well as the Parenting× Discrimination Condition (buffering) interaction term, and also type of mood measure as a within-subjects factor. The anticipated Condition× Parenting× Mood measure interaction was significant: (F[1, 108] = 7.30, p < .008), reflecting the fact that reports of anger among those in the Disc Condition, whose parents were less supportive, were significantly higher than all other means (all ts > 2.0, ps < .05). This tendency was more pronounced among the users, but the 4-way interaction was not significant (F = 2.00, p = .16).
Anger regression
Because of the results on the mood ANOVA, the regression was conducted only on anger and not depression. Use, Parenting, and Condition were included as predictors, along with the 2-way and the 3-way interaction terms. The anticipated 3-way interaction was significant: t = 1.95, p = .05, as the most anger was reported by the users in the Disc condition whose parents were less supportive. When the user and nonuser groups were analyzed separately, there was a marginal effect of Condition among the nonusers (p < .10), but no other significant effects. In contrast, the Condition effect was significant among the users (p < .01), as was the Parent × Condition interaction, t = 2.03, p < .05.
BW
The same regression was conducted on BW, and it produced very similar results. Use was significant (p < .001), as was the anticipated 3-way (Condition× Use× Parenting) interaction: t = 2.48, p = .01, which followed the expected pattern. As can be seen in Figure 4, the most BW was reported by users in the Disc Condition whose parents did not use supportive parenting practices. Looking at users and nonusers separately: again, there were no significant effects among the nonusers (all ps > .17). Among the users, the Parenting effect was marginal (p = .08), and the Condition effect was significant (t = 2.43, p < .02). More important, the Parenting× Condition interaction was significant (t = 4.04, p < .001), and it had the same pattern. Thus, supportive parenting was associated with less anger and less BW in response to manipulated discrimination, especially among those with a history of use.
Figure 4.
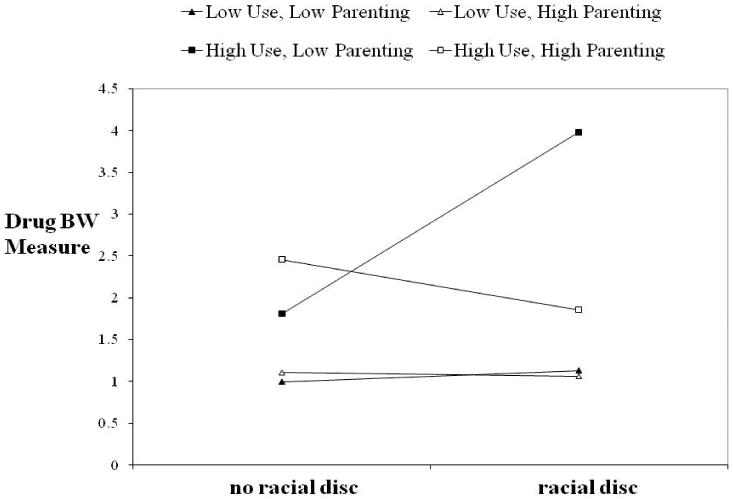
Discrimination condition predicting T2 behavioral willingness moderated by previous use and supportive parenting (Study 2).
Discussion
There was, of course, a lot more BW at this age (18.5) than there was in Study 1 (age 12.5). Still, the pattern was similar: BW was elevated by discrimination (or actually thinking about discrimination), and, as in Study 1, that effect was mediated by reports of anger, but not by depression or anxiety. Participants also reported that they would find the nondiscrimination stress situation stressful, and, as expected, there was some elevated distress in that condition, as well. What was not expected, however, was the absence of elevated BW in the Nondisc condition, in spite of the elevated distress—in other words, the lack of a relation between BW and other types of negative affect. Two explanations seem most plausible for this. One is that the nondiscrimination scenario, although stressful, inhibited thoughts of drug use—thinking about trying to catch up at work is not conducive to thinking about using drugs. A second possibility is that depression and anxiety are not as strongly related to substance BW as is anger. This explanation is consistent with the results in both studies, and with previous research. It is also possible that drug (or alcohol) BW is a unique reaction for African Americans to anger that is produced by discrimination. Perhaps anger produced in other ways, just like other affective responses to discrimination, does not lead to more substance use willingness. This is an important question with many implications; it is worthy of future research.
General Discussion
Many social scientists have speculated that racial discrimination is a source of stress for African Americans that can lead to unhealthy behaviors such as substance use and even abuse (Mays et al., 2007). In fact, a number of surveys have produced evidence of a correlation between reports of discrimination and smoking and drinking. The current studies provide prospective and experimental data that offer further evidence of this presumed relationship. The pattern of results in both studies was consistent: discrimination, whether manipulated or self-reported, was associated with reports of anger or hostility. In Study 1, that anger was predictive of more drug willingness and use in the adolescents and more drug use and/or alcohol problems in their parents. The convergence across family members and methods is rare, and it does add confidence to the contention that discrimination is a causal factor. Moreover, these effects of discrimination existed controlling for the impact of a number of other stressors included in the analyses, such as (low) SES, financial problems, and neighborhood risk (e.g., substance availability), as well as the adolescents' risk-taking tendencies, all of which have been directly linked with substance use in previous research.
Mediation
The results also provide some indication of the kind of affective reaction that links the aversive experiences with substance use. For the parents in Study 1, the zero-order correlations between discrimination and distress at all three waves were significant, but they were also significantly smaller (all ps ≤ .01) than the correlations of discrimination with hostility. The fact that T1 discrimination predicted change in hostility from T1 to T2 in spite of the high stability in the latter (and the strong correlation between discrimination and hostility at T1) provides further evidence of the impact that discrimination was having. Moreover, it appeared to be this anger/hostility that led to the increase in substance use. Discrimination was also associated with both anger and distress in the adolescents. However, at T1, the relation with anger was not any stronger than the relation with distress. The children were only 10 or 11 years old at the time and hadn't had much experience with discrimination. It is possible that this means early discriminatory experiences elicit a variety of emotions in young children, but then, as they get older, for some, that response becomes predominantly hostility and anger. How they respond to that anger may have a significant effect on their health. Several studies have suggested that anger inhibition by Blacks is associated with elevated blood pressure, and, therefore, with cardiovascular disease (Krieger & Sydney, 1996), whereas anger expression is not (Steffen, McNeilly, Anderson, & Sherwood, 2003). Anger expression and hostility are associated with poor health habits, however (Smith, 2003), which--as the current results indicate—can include substance use.
Why does Discrimination Lead to Substance Use?
Coping
Additional analyses with FACHS participants and other samples of African Americans have provided evidence of what many researchers have suggested: that the increased substance use we found was evidence of a coping style that includes use as a means of handling the stress of discrimination. Gerrard et al. (2010) found that the discrimination to use relation is significantly stronger for those Black adolescents and young adults who said they use substances to help them cope with stress. This coping style may have long term effects for some African American adults. Although rates of substance use are lower among Black than White adolescents, there is evidence that rates of substance abuse are higher among Black adults than White adults—what has been termed a “racial cross-over” effect (DHHS, 2004; Gil, Wagner, & Tubman, 2004; NIAAA, 2003). This suggests that for a small percentage of African Americans, the cumulative effects of coping with discrimination may eventually lead to substance abuse. In fact, very few of the parents in our sample reported serious alcohol problems or heavy drug use. It is worth noting, however, that the relation between discrimination and use was stronger for heavier drugs, such as crack and crack cocaine, than it was for marijuana. FACHS will have additional waves, which will allow us to track the long-term effects of early discrimination (as well as the cumulative effects) as the adolescents enter adulthood.
Self-control
It is also possible that the increased BW in both studies is not just reflective of a coping process. Willingness to engage in risky behaviors is generally stronger among adolescents who are low in self-control (Gerrard et al., 2008). This suggests BW may involve a deficit in self-regulation—i.e., failure to inhibit an impulse to engage in behaviors that one knows are unwise and/or unhealthy. Interactions with Whites have been associated with declines in self-regulatory functioning among Blacks (Bair & Steele, 2010; Richeson, Trawalter, & Shelton, 2005); presumably, that effect would be even stronger when those experiences involve discrimination. Thus, it could be the case that Black adolescents' ability to resist the temptation to use drugs may be depleted by discrimination. This speculation is consistent with work by Leith and Baumeister (1996) indicating that anger impairs self-regulation. By the same token, chronic exposure to racial discrimination may have a cumulative effect in which self-regulation skills are eroded; if so, that may contribute to the increased rate of abuse seen in some Black adults (the racial cross-over effect). This may be one reason why reports of discrimination at T1 predicted increases in use (especially heavier drug use) five years later even for the parents.
Parenting
The moderation analyses involving parenting style also produced similar results across the two studies. Adolescents whose parents used a more supportive parenting style were less likely to report increased anger after either experiencing discrimination (Study 1) or thinking about it (Study 2). The same was true for reports of drug BW in Study 2. A previous study reported that parenting buffered against the effects of discrimination on anger among the boys in the first two waves of FACHS (Simons et al., 2006). The current studies show the same basic effect with the full sample and also with experimental data; more important, these results show the impact that this kind of effective parenting can have in terms of substance willingness and use. The parenting construct did have several components to it—warmth, communication, consistent discipline—and it is possible that the different components have different effects on affect versus use. That issue remains for future research.
Although these salutary parenting effects occurred vis. a vis. racial discrimination, it should be pointed out that the effects are not unique to African Americans—supportive parenting appears to help children of many different racial/ethnic groups (Brody, Dorsey, Forehand, & Armistead, 2002; Simons, Simons, & Wallace, 2004; Wills & Cleary, 1996). It is worth mentioning that another study conducted with the same sample found that ethnic identity was also a buffer against discrimination for these adolescents (Stock, Gibbons, Walsh, & Gerrard, 2010). Taken together, this series of lab and survey studies presents a clearer picture of the factors that promote and protect against the relations between discrimination and health risk that researchers have found in the past.
Willingness and Intention
Based on previous studies and the prototype model, we had assumed that BW and BI would be highly correlated, but that BW would be a better predictor for these adolescents; this pattern is typical up through about age 17 or 18 (Pomery et al., 2009). That was the case in Study 1. In addition, there was evidence that the discrimination effects followed the social reaction path as laid out in the model. That is also consistent with previous research that has shown that affect is part of the social reaction path, and generally has more impact on BW than on BI (Gibbons et al., 2006). The path from T1 parent use to intention was also anticipated: by the time the adolescents were 12 or 13, they would have had considerable opportunity to observe substance use by their parents and, for some, this led to an expectation of use for themselves. The path from the parent's hostility to their child's BW was not anticipated, but it is not surprising that observing their parent's hostile behavior might have an impact on a child's substance vulnerability, and that this would occur through the social reaction path.
This tendency for parental influence to affect adolescent substance use through the reasoned pathway, whereas social influence (e.g., peers, the media) works through the social reaction pathway, has been incorporated into a dual-focus preventive-intervention that targets both routes to use (the Strong African American Families Program; Brody, Murry et al., 2006). The intervention does appear to affect both pathways—it has a positive effect on parenting, which influences the child's intentions to use, and it has a negative effect on the child's prototypes, which lowers their BW. As a result, it has proven to be effective at slowing the normal escalation of drinking that occurs at this age (Gerrard, Gibbons, Brody, Murry, & Wills, 2006). What the current study adds is evidence that parental negative affect (i.e., hostility) may also influence adolescent risk-taking through the social reaction pathway. This possibility has numerous implications for basic and applied research and so also seems worthy of future attention.
Limitations
There are several limitations for the two studies, some of which have been mentioned, and some of which suggest additional research. First, we are not sure why the reports of anxiety were as high as they were in Study 2. Across the two studies, however, it was clear that anxiety was elevated by discrimination, but this increase was not related to use and willingness as strongly as was anger. Second, we did not have a direct measure of anger for the parents in Study 1, but, instead, assumed that the hostility measure presented a reasonable proxy. The results with the adolescents in Study 2 (who were 18 or 19 at the time) offers some support for that assumption, but it should be examined further in future research. Third, participants in Study 2 only imagined discrimination (cf. King, 2005; Yoo & Lee, 2008), which leaves open the possibility that they might respond differently to an actual experience. Results of Study 1 suggest not, but we don't know for sure; this also appears to be an issue worth examining in the future.
Future Directions
The pattern of results with regard to affect mediation was clear with the parents in Study 1, and with the adolescents in Study 2, when they were older (age 18 or 19)—hostility/anger linked discrimination with use. However, the affect mediation pattern was less clear with the adolescents in Study 1, when they were younger. There is reason to believe that internalizing reactions, such as anxiety and depression, may actually precede development of externalizing reactions, such as hostility and anger for younger adolescents (Zahn-Waxler, Klimes-Dougan, & Slattery, 2000). Because early experience with discrimination appears to be critical (Gibbons et al., 2007), future research should further examine how younger adolescents respond to these aversive experiences, in terms of cognitions (e.g., attributions), as well as affect. It may very well be that the pathways or relations seen in the parents and older adolescents may have started differently when they were younger. Similarly, we only examined anxiety and depression. It is possible that other types of internalizing reactions, such as embarrassment or shame, may be elicited with younger adolescents, and these reactions also are antecedent to health problems. Finally, it is unlikely that the enhanced distress that we observed in all of the participants has no effect on their health status. Longitudinal research should examine these effects of heightened anxiety and depression—perhaps comparing the long-term health effects of a variety of different emotional responses to aversive racial discrimination experiences.
Conclusion
Results across the two studies using different methods converge in suggesting that perceived racial discrimination has an important impact on the mental health and substance use habits of some African Americans. Those effects can be seen in adolescents as young as 13 and in their parents, and the pattern is similar for both: Discrimination leads to anger and hostility, and for some, that affect translates into willingness to use substances and then to actual use. It is the case, however, that these negative effects of discrimination in adolescents can be countered somewhat by supportive parenting from their parents.
Acknowledgments
Support for this research came from NIDA Grants: DA021898 and DA018871. The authors thank Alex Rothman and Thomas Wills for their very helpful comments on the manuscript.
Footnotes
Five items from the scale were dropped because they were inappropriate for the adolescents. The rest of the modifications for the adolescents were minor and involved simplifying the language and replacing items assessing workplace discrimination with discrimination in the community. The parent items were essentially the same but included the original wording.
The “likely” item assesses behavioral expectation (Warshaw & Davis, 1985). These items are often used together with BI measures and are collectively referred to as intentions (Armitage & Conner, 2001), especially when assessing socially undesirable behaviors, like substance use (Parker, Manstead, Stradling, Reason, & Baxter, 1992).
Results were almost identical when regular (i.e., “social”) alcohol use was included in the index. Also, tobacco use was assessed for the adolescents; however, including these items did not change the pattern of results. For simplification, we used only alcohol and drugs in the SEMs for both adolescents and parents. Dichotomous use measures like these are typical of diagnostic instruments.
The correlation between the two internalizing indexes (depression and anxiety) was very high (as is often the case; Anderson & Mayes, in press): .61 at T1 and .65 at T2; consequently, they were combined in the analyses. Results look the same when the combined index is replaced by either affect measure by itself, or both separately—neither relates to T3 use. Similarly, Table 2 presents the correlations for each index separately; but these correlations look very similar for the combined index.
We are defining hostility in a manner similar to Kamarck et al. (2009) as a combination of behavior (aggression), cognition (mistrust of others), and negative emotion (intense anger). The anti-social personality disorder scale includes a number of items that clearly reflect this kind of hostility or anger—e.g., fighting, intentionally harming others (cf. Smith, 1994)—as well as other items that are more reflective of deviant behavior (e.g., “Have you walked off more than on job without giving notice?” “Have you more than once fired a gun to scare someone?”). When the latent construct is defined as just the behavioral and anger items, however, the construct and therefore the model look very similar to the one including all items. Rather than divide the scale, we chose to keep it intact.
There were some differences in the results due to state (e.g., more discrimination and use reported by those living in Iowa), even though the pattern of results was similar. These geographical differences are beyond the scope of this paper, and so are not discussed.
In most instances, low meant either none at all or very little (e.g., use for adolescents); percentage for low and none at all are presented separately in the Table when they differ. Medium level typically reflected occasional use or experience (e.g., some symptoms of anxiety; some BW to use); high level meant more than occasional use, experience, etc.
The paths from T1 parent discrimination to adolescent T1 anger and distress are not part of the prototype model (although they are consistent with the model), but a similar relation was found (and discussed) in previous research (Gibbons et al., 2004), so it was specified in the SEM.
When BW was dropped from the SEM, the path from BI to use became significant (β = .18, p = .05). The path from BW to use remained at the same level (β = .25, p < .001) when BI was dropped from the model.
This is a very mobile population and we know that quite a few of them did not receive the invitation letter. Ten of the 149 who agreed to participate were not available during lab hours.
Ms for the 3 mood factors by Condition were: Anger: Disc = 1.49, Nondisc = 1.28; Depression: Disc = 1.31, Nondisc = 1.21; Anxiety: Disc = 1.65, Nondisc = 1.60. It is possible the high means for Anxiety reflect the specific choice of adjectives; it is also possible that the experimental situation itself made participants nervous/anxious and this affected their responses—this was consistent with some comments made in debriefing, and is consistent with the high anxiety mean (1.60) in the low stress condition. At any rate, the pattern does indicate that relative to the Nondisc condition, anger was elevated more in the Disc condition than the other two types of affect. More important, anger was the only self-reported affect related to BW.
Publisher's Disclaimer: The following manuscript is the final accepted manuscript. It has not been subjected to the final copyediting, fact-checking, and proofreading required for formal publication. It is not the definitive, publisher-authenticated version. The American Psychological Association and its Council of Editors disclaim any responsibility or liabilities for errors or omissions of this manuscript version, any version derived from this manuscript by NIH, or other third parties.The published version is available at www.apa.org/pubs/journals/psp
Contributor Information
Frederick X. Gibbons, Department of Psychology, Iowa State University
Paul E. Etcheverry, Department of Psychology, Southern Illinois University
Michelle L. Stock, Department of Psychology, The George Washington University
Meg Gerrard, Department of Psychology, Iowa State University.
Chih-Yuan Weng, Department of Psychology, Iowa State University.
Marc Kiviniemi, Department of Health Behavior, University at Buffalo.
Ross O'Hara, Department of Psychology, Iowa State University.
References
- Anderson ER, Mayes LC. Race/ethnicity and internalizing disorders in youth: A review. Clinical Psychology Review. doi: 10.1016/j.cpr.2009.12.008. in press. [DOI] [PubMed] [Google Scholar]
- Andrews JA, Hampson SE, Barckley M, Gerrard M, Gibbons FX. The effect of early cognitions on cigarette and alcohol use during adolescence. Psychology of Addictive Behaviors. 2008;22:96–106. doi: 10.1037/0893-164X.22.1.96. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Armitage CJ, Conner M. Efficacy of the theory of planned behaviour: A meta analytic review. British Journal of Social Psychology. 2001;40:471–499. doi: 10.1348/014466601164939. [DOI] [PubMed] [Google Scholar]
- Bair AN, Steele JR. Examining the consequences of exposure to racism for the executive functioning of Black students. Journal of Experimental Social Psychology. 2010;46:127–132. [Google Scholar]
- Baron RM, Kenny DA. The moderator-mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. Journal of Personality and Social Psychology. 1986;51:1173–1182. doi: 10.1037//0022-3514.51.6.1173. [DOI] [PubMed] [Google Scholar]
- Bennett GG, Wolin KY, Robinson EL, Fowler S, Edwards CL. Perceived racial/ethnic harassment and tobacco use among African American young adults. American Journal of Public Health. 2005;95:238–240. doi: 10.2105/AJPH.2004.037812. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bodenhausen GV, Macrae CN, Hugenberg K. Social cognition. In: Millon T, Lerner MJ, editors. Handbook of Psychology: Personality and Social Psychology. Hoboken, NJ: John Wiley & Sons Inc.; 2003. pp. 257–282. [Google Scholar]
- Borrell LN, Kiefe CI, Williams DR, Diez-Roux AV, Gordon-Larsen P. Self-reported health, perceived racial discrimination, and skin color in African Americans in the CARDIA study. Social Science & Medicine. 2006;63:1415–1427. doi: 10.1016/j.socscimed.2006.04.008. [DOI] [PubMed] [Google Scholar]
- Brody GH, Chen Y, Murry VM, Ge X, Simons RL, Gibbons FX, Gerrard M, Cutrona CE. Perceived discrimination and the adjustment of African American youths: A five-year longitudinal analysis with contextual moderation effects. Child Development. 2006;77:1170–1189. doi: 10.1111/j.1467-8624.2006.00927.x. [DOI] [PubMed] [Google Scholar]
- Brody GH, Dorsey S, Forehand R, Armistead L. Unique and protective contributions of parenting and classroom processes to the adjustment of African American children living in single-parent families. Child Development. 2002;73:274–286. doi: 10.1111/1467-8624.00405. [DOI] [PubMed] [Google Scholar]
- Brody GH, Ge X, Conger RD, Gibbons FX, Murry VM, Gerrard M, Simons RL. The influence of neighborhood disadvantage, collective socialization, and parenting on African American children's affiliation with deviant peers. Child Development. 2001;72:1231–1246. doi: 10.1111/1467-8624.00344. [DOI] [PubMed] [Google Scholar]
- Brody GH, Murry VM, Gerrard M, Gibbons FX, Brown AC, Anderson T, Chen YF, Luo Z. The Strong African American Families Program: Long-term effects on adolescent alcohol use and test of a mediational model. Journal of Consulting and Clinical Psychology. 2006;74:356–366. doi: 10.1037/0022-006X.74.2.356. [DOI] [PubMed] [Google Scholar]
- Bynum MS, Burton ET, Best C. Racism experiences and psychological functioning in African American college freshmen: Is racial socialization a buffer? Cultural Diversity and Ethnic Minority Psychology. 2007;13:64–71. doi: 10.1037/1099-9809.13.1.64. [DOI] [PubMed] [Google Scholar]
- Caldwell RM, Sturges SM, Silver NC, Brinson J, Denby-Brinson R, Burgess K. An examination of the influence of perceived parenting practices on depression and substance use among African American juvenile offenders. Journal of Forensic Psychology Practice. 2006;6:31–50. [Google Scholar]
- Clark R. Interethnic group and intraethnic group racism: Perceptions and coping in Black university students. Journal of Black Psychology. 2004;30:506–526. [Google Scholar]
- Clark R, Anderson NB, Clark V, Williams DR. Racism as a stressor for African Americans: A biopsychosocial model. American Psychologist. 1999;54:805–816. doi: 10.1037//0003-066x.54.10.805. [DOI] [PubMed] [Google Scholar]
- Coffman DL, MacCallum RC. Using parcels to convert path analysis models into latent variable models. 2005;40:235–259. doi: 10.1207/s15327906mbr4002_4. Multivariate Behavioral Research. [DOI] [PubMed] [Google Scholar]
- Curry LA, Youngblade LM. Negative affect, risk perception, and adolescent risk behavior. Journal of Applied Developmental Psychology. 2006;27:468–485. [Google Scholar]
- Cutrona CE, Russell DR, Hessling RM, Brown PA, Murry V. Direct and moderating effects of community context on the psychological well-being of African American women. Journal of Personality and Social Psychology. 2000;79:1088–1101. doi: 10.1037//0022-3514.79.6.1088. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Davis GY, Stevenson HC. Racial socialization experiences and symptoms of depression among Black youth. Journal of Child and Family Studies. 2006;15:303–317. [Google Scholar]
- Department of Health and Human Services. Closing the health gap 2004 [Google Scholar]
- DuBois DL, Burk-Braxton C, Swenson LP, Tevendale HD, Hardesty JL. Race and gender influences on adjustment in early adolescence: Investigation of an integrative model. Child Development. 2002;73:1573–1592. doi: 10.1111/1467-8624.00491. [DOI] [PubMed] [Google Scholar]
- Eysenck SB, Eysenck HJ. The place of impulsiveness in a dimensional system of personality description. British Journal of Social & Clinical Psychology. 1977;16:57–68. doi: 10.1111/j.2044-8260.1977.tb01003.x. [DOI] [PubMed] [Google Scholar]
- Fite PJ, Colder CR, O'Connor RM. Childhood behavior problems and peer selection and socialization: Risk for adolescent alcohol abuse. Addictive Behaviors. 2006;31:1454–1459. doi: 10.1016/j.addbeh.2005.09.015. [DOI] [PubMed] [Google Scholar]
- Gerrard M, Gibbons FX, Brody GH, Murry VM, Wills TA. A theory based dual focus alcohol intervention for pre-adolescents: The Strong African American Families Program. Psychology of Addictive Behaviors. 2006;20:185–195. doi: 10.1037/0893-164X.20.2.185. [DOI] [PubMed] [Google Scholar]
- Gerrard M, Gibbons FX, Houlihan AE, Stock ML, Pomery EA. A dual process approach to health risk decision making: The prototype willingness model. Developmental Review Special Issue: Emerging Directions in Risk and Rational Decision Making. 2008;28:29–61. [Google Scholar]
- Gerrard M, Roberts ME, Gibbons FX, Stock ML. Substance use as coping with perceived racial discrimination among African American youth. 2010 Manuscript in preparation. [Google Scholar]
- Gibbons FX, Gerrard M, Cleveland MJ, Wills TA, Brody G. Perceived discrimination and substance use in African American parents and their children: A panel study. Journal of Personality and Social Psychology. 2004a;86:517–529. doi: 10.1037/0022-3514.86.4.517. [DOI] [PubMed] [Google Scholar]
- Gibbons FX, Gerrard M, Lane DJ. A social-reaction model of adolescent health risk. In: Suls JM, Wallston KA, editors. Social Psychological Foundations of Health and Illness. Oxford, England: Blackwell; 2003. pp. 107–136. [Google Scholar]
- Gibbons FX, Gerrard M, Reimer RA, Pomery EA. Unintentional behavior: A subrational approach to health risk. In: de Ridder DTM, de Wit JBF, editors. Self-regulation in health behavior. Chichester, UK: John Wiley & Sons Ltd.; 2006. pp. 45–70. [Google Scholar]
- Gibbons FX, Gerrard M, Vande Lune LS, Wills TA, Brody G, Conger RD. Context and cognition: Environmental risk, social influence, and adolescent substance use. Personality and Social Psychology Bulletin. 2004b;30:1048–1061. doi: 10.1177/0146167204264788. [DOI] [PubMed] [Google Scholar]
- Gibbons FX, Yeh H, Gerrard M, Cleveland MJ, Cutrona C, Simons RL, Brody GH. Early experience with racial discrimination and conduct disorder as predictors of subsequent drug use: A critical period hypothesis. Drug and Alcohol Dependence. 2007;88:S27–S37. doi: 10.1016/j.drugalcdep.2006.12.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gil AG, Wagner EF, Tubman JG. Associations between early-adolescent substance use and subsequent young-adult substance use disorders and psychiatric disorders among a multiethnic male sample in South Florida. American Journal of Public Health. 2004;94:1603–1609. doi: 10.2105/ajph.94.9.1603. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Guthrie BJ, Young AM, Williams DR, Boyd CJ, Kintner EK. African American girls' smoking habits and day-to-day experiences with racial discrimination. Nursing Research. 2002;51:183–190. doi: 10.1097/00006199-200205000-00007. [DOI] [PubMed] [Google Scholar]
- Hockey GRJ, Maule AJ, Clough PJ, Bdzola L. Effects of negative mood states on risk in everyday decision making. Cognition and Emotion. 2000;14:823–856. [Google Scholar]
- Johnson BB. Testing and expanding a model of cognitive processing of risk information. Risk Analysis. 2005;25:631–650. doi: 10.1111/j.1539-6924.2005.00609.x. [DOI] [PubMed] [Google Scholar]
- Kessler RC. UM-CIDI training guide for the national survey of health and stress, 1991-1992. Ann Arbor, MI: Univ of Michigan Institute for Social Research; 1991. [Google Scholar]
- King KR. Why is discrimination stressful? The mediating role of cognitive appraisal. Cultural Diversity and Ethnic Minority Psychology. 2005;11:202–212. doi: 10.1037/1099-9809.11.3.202. [DOI] [PubMed] [Google Scholar]
- Krieger N. Discrimination and health. In: Berkman LF, Kawachi I, editors. Social Epidemiology. Oxford: Oxford University Press; 2000. pp. 36–75. [Google Scholar]
- Krieger N, Sidney S. Racial discrimination and blood pressure: The CARDIA study of young Black and White adults. American Journal of Public Health. 1996;86:1370–1378. doi: 10.2105/ajph.86.10.1370. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Krueger RF. The structure of common mental disorders. Archives of General Psychiatry. 1999;56:921–926. doi: 10.1001/archpsyc.56.10.921. [DOI] [PubMed] [Google Scholar]
- Krueger RF, Hicks BH, Patrick CJ, Carlson SR, Iacono WG, McGue M. Etiological connections among substance dependence, antisocial behavior, and personality: Modeling the externalizing spectrim. Journal of Abnormal Psychology. 2002;111:411–424. [PubMed] [Google Scholar]
- Landrine H, Klonoff EA. Racial segregation and cigarette smoking among Blacks: Findings at the individual level. Journal of Health Psychology. 2000;5:211–219. doi: 10.1177/135910530000500211. [DOI] [PubMed] [Google Scholar]
- Landrine H, Klonoff EA. The schedule of racist events: A measure of racial discrimination and a study of its negative physical and mental health consequences. Journal of Black Psychology. 1996;22:144–168. [Google Scholar]
- Landrine H, Klonoff EA, Corral I, Fernandez S, Roesch S. Conceptualizing and measuring ethnic discrimination in health research. Journal of Behavioral Medicine. 2006;29:79–94. doi: 10.1007/s10865-005-9029-0. [DOI] [PubMed] [Google Scholar]
- Leith KP, Baumeister RF. Why do bad moods increase self-defeating behavior? Emotion, risk tasking, and self-regulation. Journal of Personality and Social Psychology. 1996;71:1250–1267. doi: 10.1037//0022-3514.71.6.1250. [DOI] [PubMed] [Google Scholar]
- Lerner JS, Keltner D. Fear, anger, and risk. Journal of Personality and Social Psychology. 2001;81:146–159. doi: 10.1037//0022-3514.81.1.146. [DOI] [PubMed] [Google Scholar]
- Martin JK, Tuch SA, Roman PM. Problem drinking patterns among African Americans: The impacts of reports of discrimination, perceptions of prejudice, and “risky” coping strategies. Journal of Health and Social Behavior. 2003;44:408–425. [PubMed] [Google Scholar]
- Mays VM, Cochran SD, Barnes NW. Race, race-based discrimination, and health outcomes among African Americans. Annual Review of Psychology. 2007;58:201–225. doi: 10.1146/annurev.psych.57.102904.190212. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Michael K, Ben-Zur H. Risk-taking among adolescents: Associations with social and affective factors. Journal of Adolescence. 2007;30:17–31. doi: 10.1016/j.adolescence.2005.03.009. [DOI] [PubMed] [Google Scholar]
- Minior T, Galea S, Stuber J, Ahern J, Ompad D. Racial differences in discrimination experiences and responses among minority substance users. Ethnicity & Disease. 2003;13:521–527. [PubMed] [Google Scholar]
- Moons WG, Mackie DM. Thinking straight while seeing red: The influence of anger on information processing. Personality and Social Psychology Bulletin. 2007;33:707–720. doi: 10.1177/0146167206298566. [DOI] [PubMed] [Google Scholar]
- Muthén LK, Muthén BO. Mplus User's Guide. 5th. Los Angeles, CA: Muthén & Muthén; 2007. [Google Scholar]
- National Institute on Alcohol Abuse and Alcoholism. Alcohol alert. Vol. 59 2003. Underage drinking: A major public health challenge. [Google Scholar]
- Nyborg VM, Curry JF. The impact of perceived racism: Psychological symptoms among African American boys. Journal of Clinical Child and Adolescent Psychology. 2003;32:258–266. doi: 10.1207/S15374424JCCP3202_11. [DOI] [PubMed] [Google Scholar]
- Ouellette JA, Gerrard M, Gibbons FX, Reis-Bergan M. Parents, peers, and prototypes: Antecedents of alcohol expectancies, willingness to drink, and alcohol consumption. Psychology of Addictive Behaviors. 1999;13:183–197. [Google Scholar]
- Parker D, Manstead A, Stradling S, Reason J, Baxter J. Intention to commit driving violations: An application of the theory of planned behavior. Journal of Applied Psychology. 1992;77:94–101. [Google Scholar]
- Piko BF, Keresztes N, Pluhar ZF. Aggressive behavior and psychosocial health among children. Personality and Individual Differences. 2006;40:885–895. [Google Scholar]
- Preacher KJ, Rucker DD, Hayes AF. Addressing moderated mediation hypotheses: Theory, methods, and prescriptions. Multivariate Behavioral Research. 2007;42:185–227. doi: 10.1080/00273170701341316. [DOI] [PubMed] [Google Scholar]
- Pomery EA, Gibbons FX, Reis-Bergan M, Gerrard M. From willingness to intention: Experience moderates the shift from reactive to reasoned behavior. Personality and Social Psychology Bulletin. 2009;35:894–908. doi: 10.1177/0146167209335166. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Raghunathan R, Pham MT. All negative moods are not equal: Motivational influences of anxiety and sadness on decision making. Organizational Behavior & Human Decision Processes. 1999;79:56–77. doi: 10.1006/obhd.1999.2838. [DOI] [PubMed] [Google Scholar]
- Reyna VF, Farley F. Risk and rationality in adolescent decision making: Implications for theory, practice, and public policy. Psychological Science in the Public Interest. 2006;7:1–44. doi: 10.1111/j.1529-1006.2006.00026.x. [DOI] [PubMed] [Google Scholar]
- Richeson JA, Trawalter S, Shelton NJ. African Americans' implicit racial attitudes and the depletion of executive function after interracial interactions. Social Cognition. 2005;23:336–352. [Google Scholar]
- Richman LS, Bennett GG, Pek J, Siegler I, Williams RB., Jr Discrimination, dispositions, and cardiovascular responses to stress. Health Psychology. 2007;26:675–683. doi: 10.1037/0278-6133.26.6.675. [DOI] [PubMed] [Google Scholar]
- Ryan AM, Gee GC, Laflamme DF. The association between self-reported discrimination, physical health and blood pressure: Findings from African Americans, Black immigrants, and Latino immigrants in New Hampshire. Journal of Health Care for the Poor and Underserved. 2006;17:116–132. doi: 10.1353/hpu.2006.0092. [DOI] [PubMed] [Google Scholar]
- Rydell RJ, Mackie DM, Maitner AT, Claypool HM, Ryan MJ, Smith ER. Arousal, processing and risk-taking: Consequences of intergroup anger. Personality and Social Psychology Bulletin. 2008;34:1141–1152. doi: 10.1177/0146167208319694. [DOI] [PubMed] [Google Scholar]
- Scott LD, Jr, House LE. Relationship of distress and perceived control to coping with perceived racial discrimination among black youth. Journal of Black Psychology. 2005;31:254–272. [Google Scholar]
- Shaffer D, Schwab-Stone M, Fisher P, Cohen P, Placentini J, Davies M, Connors CK, Regier D. The diagnostic interview schedule for children (DISC-R): IV. Preparation, field testing, inter-rater reliability and acceptability. Journal of the American Academy of Child and Adolescent Psychiatry. 1993;32:643–650. doi: 10.1097/00004583-199305000-00023. [DOI] [PubMed] [Google Scholar]
- Simons RL, Lin K, Gordon LC, Brody GH, Murry V, Conger RD. Community differences in the association between parenting practices and child conduct problems. Journal of Marriage and Family. 2002;64:331–345. [Google Scholar]
- Simons RL, Simons LG, Burt CH, Drummund H, Stewart E, Brody GH, Gibbons FX, Cutrona C. Supportive parenting moderates the effect of discrimination upon anger, hostile view of relationships, and violence among African American boys. Journal of Health and Social Behavior. 2006;47:373–389. doi: 10.1177/002214650604700405. [DOI] [PubMed] [Google Scholar]
- Simons RL, Simons LG, Wallace LE. Families, delinquency, and crime: Linking society's most basic institution to antisocial behavior. Los Angeles: Roxbury; 2004. [Google Scholar]
- Smith TW. Hostility and health: Current status of a psychosomatic hypothesis. In: Salovey P, Rothman AJ, editors. Social Psychology of Health: Key Readings. New York: Psychology Press; 2003. pp. 325–341. [DOI] [PubMed] [Google Scholar]
- Steffen PR, McNeilly M, Anderson N, Sherwood A. Effects of perceived racism and anger inhibition on ambulatory blood pressure in African Americans. Psychosomatic Medicine. 2003;65:746–750. doi: 10.1097/01.psy.0000079380.95903.78. [DOI] [PubMed] [Google Scholar]
- Stock ML, Gibbons FX, Walsh L, Gerrard M. The protective effects of racial identity on substance use vulnerability among African American young adults faced with racial discrimination. Manuscript under review 2010 [Google Scholar]
- Swim JK, Hyers LL, Cohen LL, Fitzgerald DC, Bylsma WH. African American college students' experiences with everyday racism: Characteristics of and responses to these incidents. Journal of Black Psychology. 2003;29:38–67. [Google Scholar]
- Terrell F, Miller AR, Foster K, Watkins CE., Jr Racial discrimination induced anger and alcohol use among Black adolescents. Adolescence. 2006;40:485–492. [PubMed] [Google Scholar]
- Trumbo CW. Heuristic-systematic information processing and risk judgment. Risk Analysis. 1999;19:391–400. doi: 10.1023/a:1007092410720. [DOI] [PubMed] [Google Scholar]
- Verdejo-García A, Bechara A, Recknor EC, Pérez-García M. Negative emotion-driven impulsivity predicts substance dependence problems. Drug and Alcohol Dependence. 2007;91:213–219. doi: 10.1016/j.drugalcdep.2007.05.025. [DOI] [PubMed] [Google Scholar]
- Wang XT. Emotions within reason: Resolving conflicts in risk preference. Cognition & Emotion. 2006;20:1132–1152. [Google Scholar]
- Warshaw PR, Davis FD. The accuracy of behavioral intention versus behavioral expectation for predicting behavioral goals. The Journal of Psychology. 1985;119:599–602. [Google Scholar]
- Webb JA, Baer PE, Getz G, McKelvey RS. Do fifth graders' attitudes and intentions toward alcohol use predict seventh-grade use? Journal of the American Academy of Child Adolescent Psychiatry. 1996;35:1611–1617. doi: 10.1097/00004583-199612000-00012. [DOI] [PubMed] [Google Scholar]
- Whitbeck LB, Hoyt DR, McMorris BJ, Chen X, Stubben JD. Perceived discrimination and early substance abuse among American Indian children. Journal of Health and Social Behavior. 2001;42:405–424. [PubMed] [Google Scholar]
- Williams DR, Neighbors HW, Jackson JS. Racial/ethnic discrimination and health: Findings from community studies. American Journal of Public Health. 2003;93:200–208. doi: 10.2105/ajph.93.2.200. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wills TA, Cleary SD. How are social support effects mediated? A test with parental support and adolescent substance use. Journal of Personality and Social Psychology. 1996;71:937–952. doi: 10.1037//0022-3514.71.5.937. [DOI] [PubMed] [Google Scholar]
- Wills TA, Gibbons FX, Gerrard M, Brody GH. Protection and vulnerability processes relevant for early onset of substance use: A test among African American children. Health Psychology. 2000;19:253–263. doi: 10.1037//0278-6133.19.3.253. [DOI] [PubMed] [Google Scholar]
- Yoo HC, Lee RM. Does ethnic identity buffer or exacerbate the effects of frequent racial discrimination on situational well-being of Asian Americans. Journal of Counseling Psychology. 2008;55:63–74. [Google Scholar]
- Zahn-Waxler C, Klimes-Dougan B, Slattery MJ. Internalizing problems of childhood and adolescence: Prospects, pitfalls, and progress in understanding the development of anxiety and depression. Development and Psychpathology. 2000;12:443–466. [PubMed] [Google Scholar]