

Abstract
Background
Variations in the timing of dialysis initiation may explain some geographical variations in RRT incidence, but this effect has never been quantified.
Methods
Using data from the French Rein registry, we quantified the association between RRT incidence in 2006–2007 and median eGFR values before starting dialysis at the administrative district level with geographically appropriate methods.
Results
Crude RRT incidence varied from 80.4 pmi to 238.6 pmi between administrative districts, and median eGFR at dialysis initiation from 5.9 to 11.8 ml/min/1.73m2. Age and sex-adjusted RRT incidence associated with a 1.2 ml/min/1.73m2 increase in median eGFR rose 8% (4%–13%) before and 9% (5%–13%) after controlling for the effect of 9 potential socioeconomic and medical risk factors.
Conclusions
The impact of increased eGFR at initiation should be taken into account in guidelines recommending earlier dialysis start.
Keywords: Adult, Glomerular Filtration Rate, Humans, Incidence, Middle Aged, Renal Dialysis, Renal Replacement Therapy, statistics & numerical data, Time Factors
Keywords: Epidemiology, ESRD, glomerular filtration rate, incidence, spatial analysis
INTRODUCTION
In the last decade, incidence rates for renal replacement therapy (RRT) for end-stage renal disease (ESRD) have increased worldwide. Simultaneously, dialysis has tended to start earlier, although the timing of initiation remains controversial (1,2, 3,4,5,6,7,8,9,10). In the US the percentage of patients starting dialysis with an estimated glomerular filtration rate (eGFR) greater than 10 mL/min/1.73 m2 more than doubled from 1996 through 2005, from 25 to 54%. Starting patients at a higher eGFR may increase RRT incidence because some of these might have died in the interval between when they started RRT and when they would have done so with a lower threshold eGFR level (11). But this effect has never been quantified.
Although incident rates vary widely between countries (12,13,14), international comparisons require careful consideration of medical and non-medical factors that may contribute to these variations. Access to treatment, health spending, and resources explain a large part of these disparities. Exploring geographical patterns of RRT incidence within one single country may partially avoid these difficulties and facilitate the study of other determinants, including clinical practices.
We therefore quantified the association between eGFR level at dialysis initiation and RRT incidence rate in 71 French administrative districts, adjusting for potential explanatory variables (15).
MATERIALS AND METHODS
Information about patients with incident ESRD came from the French REIN registry, described in detail elsewhere (16). We extracted data for all patients with incident ESRD from January 1, 2006, to December 31, 2007, in 71 administrative districts (covering 76% of the French population). Information included the patient’s age, sex, district of residence, mean travel time to dialysis center and glomerular filtration rate (eGFR) estimated with the simplified MDRD equation at RRT start. The median value of eGFR at dialysis initiation was calculated for each administrative district.
Administrative districts were characterized by 9 different indicators, all potential confounders (15): rurality (population density), precariousness (proportion of people aged 20–59 years receiving minimum guaranteed income allowances), morbidity-mortality (age-adjusted cardiovascular mortality rate, age-adjusted rate of premature mortality due to alcohol in men, age and sex-adjusted prevalence of treated diabetes), health-care resources and supply (number of specialists and of nephrologists per 100 000 inhabitants, proportion of patients whose mean travel time to a dialysis centre exceeds 45 minutes) and clinical practices (proportion of incident patients older than 85 years).
A hierarchical random-effects Poisson regression model with spatially structured residuals (17,18) was used to investigate the association of the indirect age-and-sex-standardized incidence ratios with median eGFR at initiation. A multilevel model was used to take regional and administrative district variability into account. Associations between RRT incidence and eGFR were examined before and after controlling for the effect of other significant characteristics in multivariable models and are expressed as rate ratios of incidence associated with an increase of 1 standard deviation and their 95% credibility intervals. Models were fitted with an iterative stochastic algorithm in WinBUGS V.1.4.3 (19,20). Philcarto 5.05 (http://philgeo.free.fr) and the open source vector graphics editor Inkscape, with Jenks discretisation, produced all maps.
RESULTS
This analysis covers 12,865 patients who began dialysis between 2006 and 2007 in the 71 administrative districts, for a mean number of 181 new patients (range: 19–812). The crude district RRT incidence rate varied from 80.4 pmi to 238.6 pmi (Figure 1). Rates were highest in the northeast and south and lowest in the west and east. Three administrative districts (Haute-Marne, Loir-et-Cher and Ardèche) had unexpectedly high rates.
Figure 1.
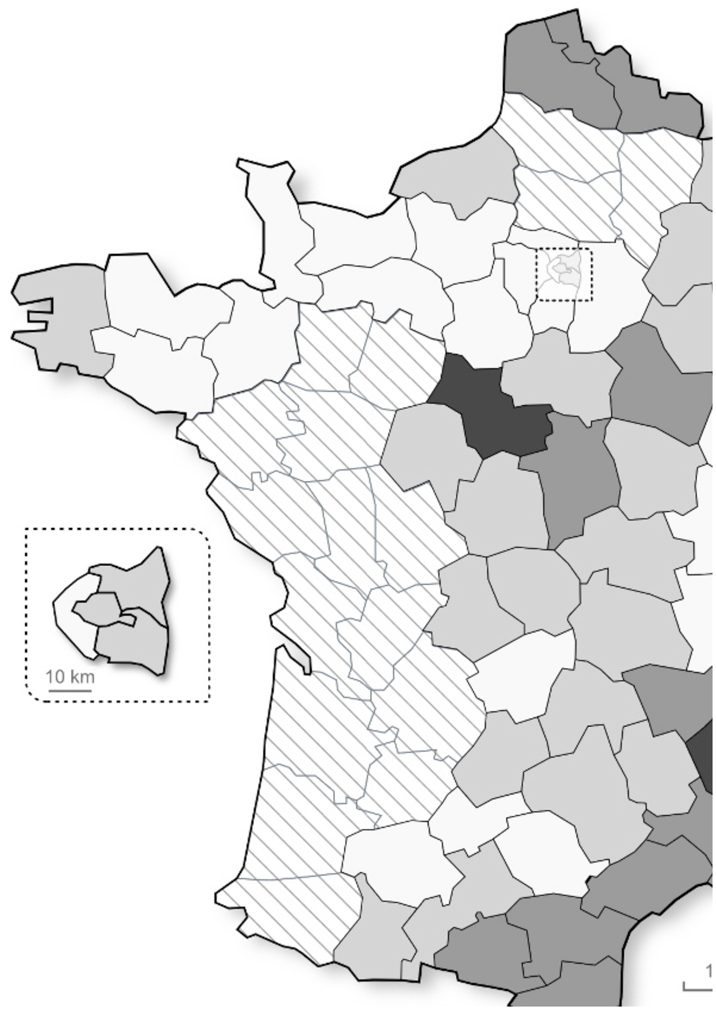
Geographical distribution of the crude RRT incidence by administrative districts
The median eGFR at dialysis initiation varied from 5.9 to 11.8 ml/min/1.73m2 (mean 8.2, SD 1.2) across administrative districts (Figure 2). Age- and sex-adjusted RRT incidence associated with a 1.2 ml/min/1.73m2 increase in median eGFR rose by 8% (95% credibility interval: 4%–13%) before and 9% (95% CI: 5%–13%) after controlling for the effect of 9 potential socioeconomic and medical risk factors.
Figure 2.
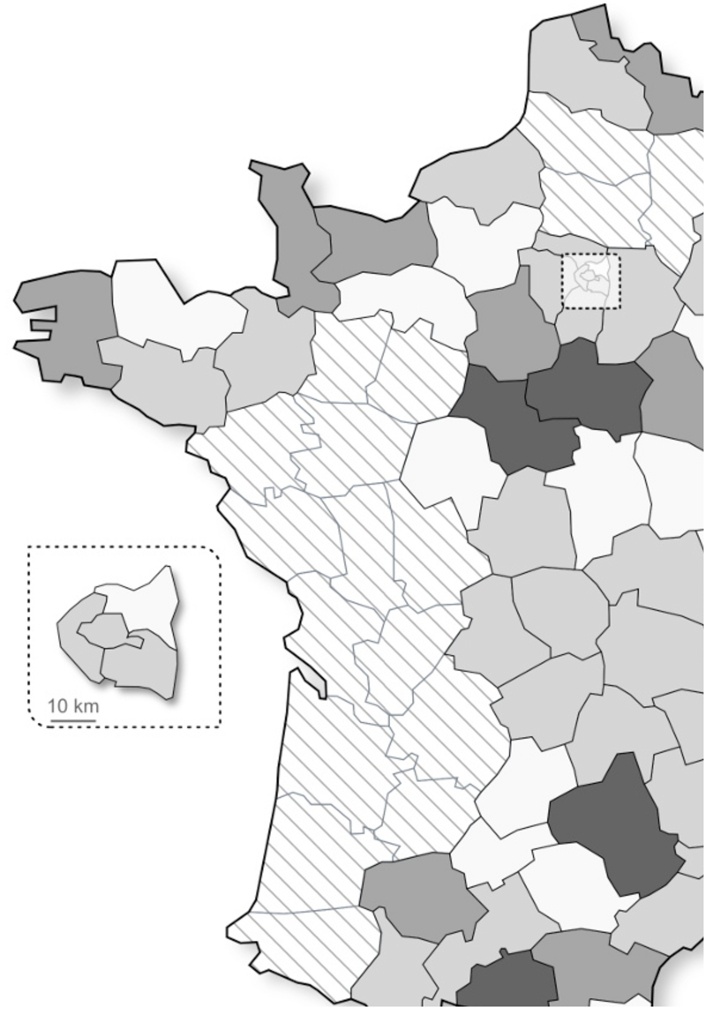
Geographical distribution of the median eGFR at dialysis initiation by administrative districts
The spatial pattern of RRT incidence is nonetheless identical to that of eGFR because other factors, such as diabetes prevalence, also explain geographic variations of RRT incidence.
DISCUSSION
This study shows significant geographical differences in RRT incidence in 71 French administrative districts and an ecological association between median eGFR at RRT start and RRT incidence. Some studies have investigated the possible determinants of these variations (21,22,23,24,25,26), but to our knowledge this is the first report to quantify with geographically appropriate methods the contribution of early dialysis initiation. Moreover, the 3 administrative districts with unexpectedly high incidence rates (over 210 pmi) all had higher median eGFR levels at RRT start (over 10 ml/min/1.73m2).
Lower RRT incidence associated with lower eGFR at initiation reflects mortality associated with decreasing eGFR. Whether all patients with ESRD (eGFR < 15 ml/min/1.73 m2) who die before starting RRT would benefit from dialysis, nevertheless, remains controversial. Earlier studies showed better outcome with early start (3,9), but more recent ones tended to observe the opposite (4–8). Based on Rein registry data, we have recently shown that age and comorbidity strongly determined the level of kidney function at dialysis start and explained most of the association of poor survival with greater eGFR(2).
However, the trends towards older new patients with greater comorbidity and clinical conditions, such as uncontrolled heart failure, may encourage nephrologists to continue starting dialysis at higher eGFR levels. The impact of prevention programs that slow the progression of chronic renal disease may thus be counterbalanced by earlier initiation.
Earlier initiation may increase costs because more patients will be treated by dialysis. Inversely, timely initiation may attenuate the complications of chronic renal failure and consequently reduce total cost (3,10). An appropriate medico-economic study is warranted to answer this critical question and to quantify the implications of early start recommendations for healthcare funding.
Conclusion
This study shows that increased eGFR at initiation may have a substantial impact on RRT incidence. This should be taken into account in guidelines recommending earlier dialysis start and considered for healthcare planning.
Acknowledgments
We acknowledge all registry participants, especially to the nephrologists and the professionals who collected the data and conducted the quality control. The dialysis center participating to the registry are listed in the annual report : http://www.agence-biomedecine.fr/article/142
Contributor Information
Cécile Couchoud, REIN Registry Agence de la biomédecine, La Plaine Saint-Denis, FR.
Chantal Guihenneuc, MAP5, Mathématiques appliquées Paris 5 CNRS : UMR8145, Université Paris Descartes, FR.
Florian Bayer, agence de la biomédecine La Plaine Saint-Denis, FR.
Bénédicte Stengel, Recherche en épidémiologie et biostatistique INSERM : U780, INSERM : IFR69, Université Paris Sud - Paris XI, 16, Avenue Paul Vaillant-Couturier 94807 VILLEJUIF CEDEX,FR.
References
- 1.Rosansky SJ, Clark WF, Eggers P, Glassock RJ. Initiation of dialysis at higher GFRs: is the apparent rising tide of early dialysis harmful or helpful? Kidney Int. 2009;76 (3):245–252. doi: 10.1038/ki.2009.161. [DOI] [PubMed] [Google Scholar]
- 2.Lassalle M, Labeeuw M, Frimat L, et al. Age and comorbidity explain the paradoxical association of poor survival with greater GFR at start of dialysis. doi: 10.1038/ki.2010.14. Article submitted to Kidney International. [DOI] [PubMed] [Google Scholar]
- 3.Churchill DN. An evidence-based approach to earlier initiation of dialysis. Am J Kidney Dis. 1997;30(6):899–906. doi: 10.1016/s0272-6386(97)90102-5. [DOI] [PubMed] [Google Scholar]
- 4.Traynor JP, Simpson K, Geddes CC, Deighan CJ, Fox JG. Early initiation of dialysis fails to prolong survival in patients with end-stage renal failure. J Am Soc Nephrol. 2002;13(8):2125–32. doi: 10.1097/01.asn.0000025294.40179.e8. [DOI] [PubMed] [Google Scholar]
- 5.Beddhu S, Samore MH, Roberts MS, et al. Impact of timing of initiation of dialysis on mortality. J Am Soc Nephrol. 2003;14(9):2305–12. doi: 10.1097/01.asn.0000080184.67406.11. [DOI] [PubMed] [Google Scholar]
- 6.Kazmi WH, Gilbertson DT, Obrador GT, et al. Effect of comorbidity on the increased mortality associated with early initiation of dialysis. Am J Kidney Dis. 2005;46(5):887–96. doi: 10.1053/j.ajkd.2005.08.005. [DOI] [PubMed] [Google Scholar]
- 7.Sawhney S, Djurdjev O, Simpson K, Macleod A, Levin A. Survival and dialysis initiation: comparing British Columbia and Scotland registries. Nephrol Dial Transplant. 2009 Apr 23; doi: 10.1093/ndt/gfp189. [Epub ahead of print] [DOI] [PubMed] [Google Scholar]
- 8.Stel VS, Dekker FW, Ansell D, et al. Residual renal function at the start of dialysis and clinical outcomes. Nephrol Dial Transplant. 2009 Jun 10; doi: 10.1093/ndt/gfp264. [Epub ahead of print] [DOI] [PubMed] [Google Scholar]
- 9.Korevaar JC, van Manen JG, Boeschoten EW, Dekker FW, Krediet RT NECOSAD Study Group. When to start dialysis treatment: where do we stand? Perit Dial Int. 2005 Feb;25(Suppl 3):S69–72. Review. [PubMed] [Google Scholar]
- 10.Obrador TG, Pereira JG. Initiation of dialysis: current trends and the case for timely initiation. Perit Dial Int. 2000;20(suppl 2):S142–9. [PubMed] [Google Scholar]
- 11.McDonald S, McCredie M, Williams S, et al. Factors influencing reported rates of treated end-stage renal disease. Adv Chronic Kidney Dis. 2005;12(1):32–8. doi: 10.1053/j.ackd.2004.10.011. [DOI] [PubMed] [Google Scholar]
- 12.US Renal Data System. National Institute of Diabetes and digestive and Kidney Diseases. National Institute of health; Bethesda, MD: 2008. USRDS 2008 Annual Data Report. [Google Scholar]
- 13.ERA-EDTA. ERA-EDTA Registry 2006 Annual Report. Academic Medical Center, Department of Medical Informatics; Amsterdam, The Netherlands: 2008. [Google Scholar]
- 14.Caskey F, Jager K, Elliot I, et al. The EVEREST Study: an international collaboration. Nephrol Dial Transplant Plus. 2009 doi: 10.1093/ndtplus/sfp146. (in press) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.McClellan WM, Flanders WD. Risk factors for progressive chronic kidney disease. J Am Soc Nephrol. 2003;14(7 Suppl 2):S65–70. doi: 10.1097/01.asn.0000070147.10399.9e. [DOI] [PubMed] [Google Scholar]
- 16.Couchoud C, Stengel B, Landais P, et al. The renal epidemiology and information network (REIN): a new registry for end-stage renal disease in France. Nephrol Dial Transplant. 2006;21(2):411–8. doi: 10.1093/ndt/gfi198. [DOI] [PubMed] [Google Scholar]
- 17.Richardson S. Spatial models in epidemiological applications. In: Green PJ, Hjort NL, Richardson S, editors. Highly structured stochastic systems. Oxford: Oxford University Press; 2003. pp. 237–59. [Google Scholar]
- 18.Besag JE, York JC, Molliè A. Bayesian image restoration, with two applications in spatial statistics (with discussion) Annals of the Institute of Statistical Mathematics. 1991;43:1–59. [Google Scholar]
- 19.Wakefield JC, Best NG, Waller LA. Bayesian approaches to disease mapping. In: Elliott P, Wakefield JC, Best NG, Briggs DJ, editors. Spatial epidemiology: methods and applications. Oxford: Oxford University Press; 2000. pp. 104–27. [Google Scholar]
- 20.Lunn DJ, Thomas A, Best N, et al. WinBUGS -- a Bayesian modelling framework: concepts, structure, and extensibility. Statistics and Computing. 2000;10:325–337. [Google Scholar]
- 21.Fan ZJ, Lackland DT, Lipsitz SR, et al. Geographical patterns of end-stage renal disease incidence and risk factors in rural and urban areas of South Carolina. Health Place. 2007;13:179–187. doi: 10.1016/j.healthplace.2005.12.002. [DOI] [PubMed] [Google Scholar]
- 22.Roderick P, Clements S, Stone N, et al. What determines geographical variation in rates of acceptance onto renal replacement therapy in England? J Health Serv Res Policy. 1999;4(3):139–46. doi: 10.1177/135581969900400304. [DOI] [PubMed] [Google Scholar]
- 23.Caskey FJ, Schober-Halstenberg HJ, Roderick PJ, et al. Exploring the differences in epidemiology of treated ESRD between Germany and England and Wales. Am J Kidney Dis. 2006;47:445–454. doi: 10.1053/j.ajkd.2005.12.026. [DOI] [PubMed] [Google Scholar]
- 24.Stewart JH, McCredie MR, Williams SM ESRD Incidence Study Group. Geographic, ethnic, age-related and temporal variation in the incidence of end-stage renal disease in Europe, Canada and the Asia-Pacific region, 1998–2002. Nephrol Dial Transplant. 2006;21(8):2178–83. doi: 10.1093/ndt/gfl145. [DOI] [PubMed] [Google Scholar]
- 25.Usami T, Koyama K, Takeuchi O, et al. Regional Variations in the Incidence of End-Stage Renal Failure in Japan. JAMA. 2000;284(20):2622–2624. doi: 10.1001/jama.284.20.2622. [DOI] [PubMed] [Google Scholar]
- 26.Cass A, Cunningham J, Wang Z, et al. Regional variation in the incidence of end-stage renal disease in Indigenous Australians. Med J Aust. 2001;175:24–27. doi: 10.5694/j.1326-5377.2001.tb143507.x. [DOI] [PubMed] [Google Scholar]