

Abstract
Objective
The purpose of this case report is to describe a patient who regularly practiced self-manipulation of her neck who presented with shoulder and neck pain and was undergoing a vertebral artery dissection.
Clinical Features
A 42-year-old female patient sought care for left shoulder pain with a secondary complaint of left lower neck pain. Twelve days prior, she had had “the worst headache of her life,” which began in her left lower cervical spine and extended to her left temporal region. The pain was sudden and severe, was described as sharp and burning, and lasted 3 hours. She reported nausea, vomiting, and blurred vision.
Intervention and Outcome
Initial history and examination suggested that the patient's head and neck pain was not musculoskeletal in origin, but vascular. She repeatedly requested that an adjustment be performed, but instead was referred to the local emergency department for further evaluation. Magnetic resonance angiogram revealed a dissection of the left vertebral artery from C6 to the C2-C3 interspace and a 3-mm dissecting pseudoaneurysm at the C3 level. She underwent stent-assisted percutaneous transluminal angioplasty combined with antiplatelet therapy (clopidogrel) and experienced a good outcome.
Conclusion
This case suggests that careful history taking and awareness of the symptoms of VAD are necessary in cases of sudden head and neck pain. More research is needed on the relationship between vertebral artery dissection and self-manipulation of the neck.
Key indexing terms: Vertebral artery dissection, Chiropractic
Introduction
Vertebral artery dissection (VAD) is one cause of stroke in patients who are younger than 45 years old.1-4 It is estimated that 1 to 1.5 per 100 000 individuals in the United States will experience this condition.5,6 Common presenting symptoms are headache and neck pain; thus, many of these patients may present for chiropractic care. As these symptoms are nonspecific and may be related to a number of underlying conditions, it can be difficult to properly diagnose a VAD.7 Currently, medical treatment of this condition includes administration of anticoagulant drugs.8
Vertebral artery dissection is the result of a flap-like tear in the tunica intima of the vertebral artery. Because of this tear, blood enters into the tunica media causing a hematoma in the vessel wall. Although the mechanism of this condition is well documented, little research has been conducted concerning the clinical presentation of VAD.9 Cassidy et al10 and Murphy11 recently suggested that some patients visiting chiropractic clinics with complaints of head and neck pain may have undiagnosed VAD. These patients may undergo cervical spinal manipulation for this pain, further complicating their VAD through a thromboembolic event.10 This can lead to the assumption that manipulation caused the dissection. In light of this, it is critical that doctors of chiropractic be able to differentially diagnose VAD from benign causes of head and neck pain to avoid catastrophic complications. The purpose of this case report is to describe a patient with VAD who reported that she regularly practiced self-manipulation of her neck and to present guidelines to identify and properly manage VAD.
Case report
A 42-year-old female patient complained of left-sided neck pain and shoulder pain at a chiropractic college community outreach clinic. The patient had not seen a chiropractor for 8 years according to records; however, she reported that she would regularly self-manipulate or “crack” her neck to reduce neck pain. She reported that she had performed this self-manipulation of her neck several times a day for the past several years. She was not a chiropractor and had no training in manipulative therapy. When she arrived at the clinic, she appeared tired and distressed. She stated that she had burning, sharp pain and requested that her neck and shoulder be adjusted.
A chiropractic intern performed a routine initial evaluation to determine the diagnosis. Bilateral pulse, respiration, and seated blood pressure were measured within normal limits. Palpation indicated burning on the left side of C7, myospasms on the right side paraspinal muscles between T4-T9, myospasms on the left side paraspinal muscles between L2-L4, and a high right hip. Cervical compression and shoulder depressor test caused pain in the left lower cervical region.
The supervising doctor of chiropractic requested a more detailed history based upon the distressed appearance of the patient. As the patient was further questioned, she reported a persistent headache that started 12 days prior while driving her vehicle. The pain was in her lower neck and shoulder and ascended to the temporal region on her left side. She described her headache as a stabbing pain, worse than she had ever experienced before, that moved throughout her head and occurred for approximately 5 to 10 minutes at a time. This admission raised red flags for both the intern and the supervising chiropractor. The pain was intense and burning, rating a 10/10 on a numerical rating scale. This pain was followed by episodes of nausea and vomiting. She stated that she would have these headaches for 3 hours per day and, for most of the time, she would be on her hands and knees in a dark corner of a room. She denied any tobacco or oral contraceptive use and noted drinking socially. Throughout the visit, she repeatedly requested that she wanted to have her neck manipulated. The supervising chiropractor stated that he would not perform a chiropractic manipulation due to the seriousness of her suspected condition. He quickly referred her out to an emergency department for consult and advised her not to self-manipulate her neck.
The patient refused the immediate emergency attention recommended by the supervising chiropractor and instead waited until the following day because of insurance reasons before she went to a university hospital. At admission to the hospital, she reported no dizziness, lightheadedness, weakness, or other focal motor or sensory changes, consistent with her presentation at the chiropractic clinic. Her physical examination and blood profile showed no abnormalities. A magnetic resonance imaging was conducted to rule out the possibility of stroke, and the findings were negative. A magnetic resonance angiogram with contrast was ordered to evaluate the integrity of the vertebral arteries. The results of this test showed left vertebral artery dissection extending from C6 to the C2-C3 interspace with poststenosis and a 3-mm pseudoaneurysm at the C3 level. The dissection is best visualized in Fig 1 near the arrow as the decreased luminal caliber with increased signal intensity medial to the vessel. The emergency department doctor explained to her that the chiropractor recognized the need for emergency care and referring her to the hospital may have saved her life.
Fig. 1.
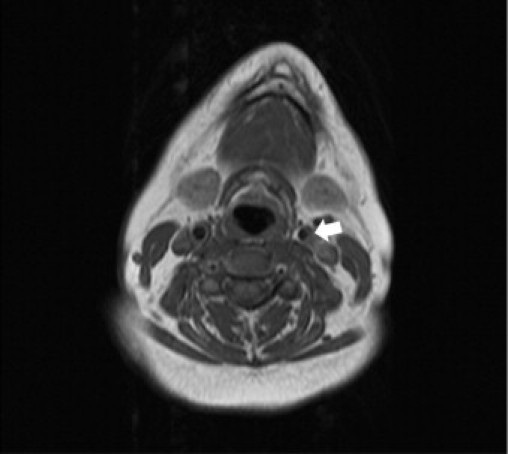
Presurgical magnetic resonance angiogram showing arterial narrowing as indicated by arrow.
The emergency department physician determined that she needed immediate surgical attention. She subsequently underwent diagnostic cerebral angiogram and stent-assisted percutaneous transluminal angioplasty of the dissected left vertebral artery involving 3 overlapping stents Aspirin and clopidogrel were given for blood-clotting protection, and omeprazole was prescribed for stomach protection while on aspirin. She was instructed by her medical physician to avoid abrupt neck maneuvers and only perform physical activity that she could tolerate. As of the submission of this case report, she has resumed her working duties and is living a healthy, normal life.
Discussion
In writing this case, the literature was searched to determine if self-manipulation has been published in relation to VAD. At present, it was determined that this is the first published case of a person who claims to self-manipulate presenting with VAD.
It should be stressed that, although cervical spinal manipulation has been implicated in prior research as a possible causative event in VAD, there are many others including sneezing, violent coughing, turning the head while driving, kneeling at prayer, yoga, and sexual intercourse.12-14 Given the mundane nature of these activities and the fact that the vast majority of the population practices them without ever developing VAD (a rare condition), it is unlikely that they could be considered a “cause” of the condition. Recent research suggests that there may be no causal relationship15 and that general forces of manipulation may not be enough to cause VAD.16 It is more likely that previous damage or a preexisting defect was present and that an otherwise trivial trauma triggered the VAD. This hypothesis fits with new research by Cassidy et al10 who reason that patients who are undergoing a VAD may present to a chiropractic clinic with neck pain and headaches similar to neuromusculoskeletal conditions. Oftentimes, the chiropractor may misdiagnose this as a more benign condition and then adjust the patient, which can complicate the underlying VAD. Thus, chiropractors need to recognize the initial symptoms of VAD so that diagnosis and treatment can be administered without further harm caused by adjusting the patient.11 Cassidy et al10 note risk factors for VAD independent of manipulation. These factors include connective tissue disorders, hypertension, recent infection, vessel abnormalities, and atherosclerosis. A patient who presents with symptoms similar to this patient, or parts of the history in Fig 2, should be screened for these risk factors before cervical manipulation is given to prevent serious complications due to underlying VAD.
Fig. 2.
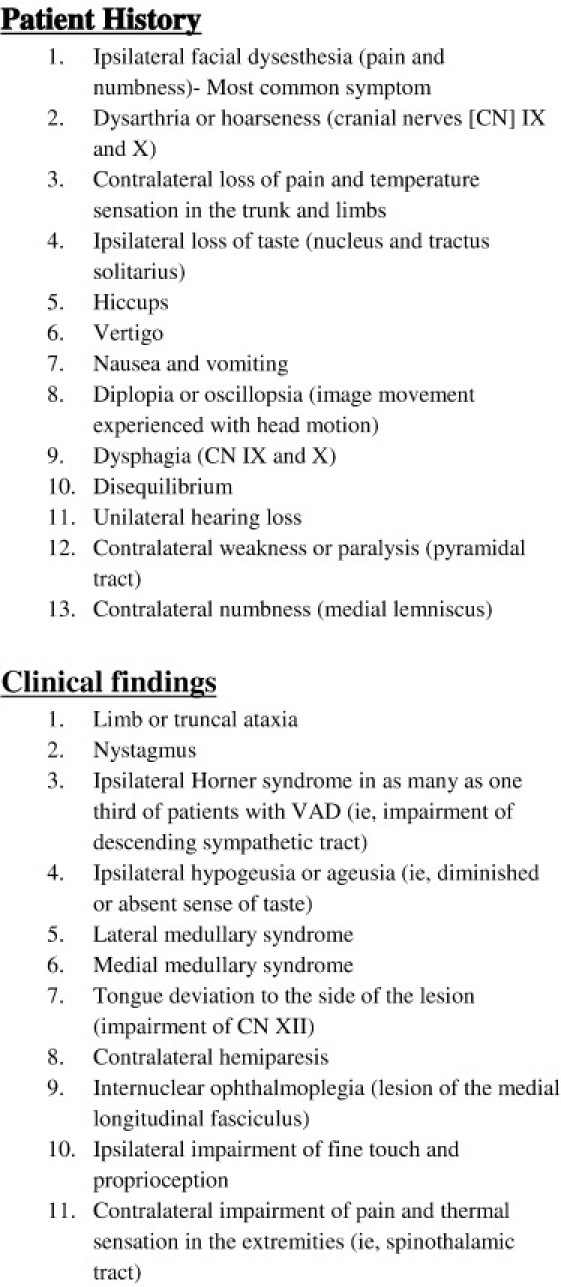
Potential patient history and clinical signs or symptoms indicating possible VAD. Adapted with permission from eMedicine.com, 2010. Available from: emedicine.medscape.com/article/761451-overview.11
Limitations
There are several important limitations to this case report. Although the present report represents the first to describe a case of VAD for a patient who habitually practiced self-manipulation before the onset of symptoms, a sample of 1 cannot “prove” that a relationship exists between self-manipulation of the neck and VAD. It merely suggests a chronological association and need for future studies to determine causality. Second, as this is a retrospective study, it was not possible to determine the exact interval of time between the last cervical self-manipulation and the onset of symptoms. All that is known, as stated earlier, is that the patient reportedly self-manipulated her neck several times a day. This raises the question of whether or not the patient was undergoing a VAD and had resultant head and neck pain for which she tried to self-manipulate, leading to further complication of the condition. This also raises another question of whether her crude attempts at replicating a chiropractic adjustment were the cause of the VAD in the first place. Although this fits the narrative portrayed by Smith, Rothwell, and others, it does not correspond to the recent prevailing thoughts of Cassidy or Murphy. The exact mechanism of any reported case of VAD is beyond the realm of a case study or case series; but because temporality is one of Sir Bradford Hill's requirements for determining causality, manipulation before VAD detection cannot be ruled out as a cause without specific research, which has yet to be conducted.
Conclusion
It is critical for doctors of chiropractic to exercise proper clinical evaluation and treatment when addressing their patients, specifically when dealing with suspected VAD. This case report should serve as a reminder that recognizing “red flags” is critical to a proper diagnosis. By taking a proper history, realizing the warning signs, and performing the right action plan (ie, immediate referral to an emergency department), the chiropractic doctor and intern contributed to the preservation of this patient's life.
Funding sources and potential conflicts of interest
No funding sources or conflicts of interest were reported for this study.
Acknowledgment
The authors thank James Johnson, DC, for his research assistance; Brandon Maki for his editorial assistance; as well as Dana Lawrence, DC, for his review and Terri Cannon for her proofreading and logistics help.
References
- 1.Beletsky V., Nadareishvili Z., Lynch J., Shuaib A., Woolfenden A., Norris J.W. Cervical arterial dissection: time for a therapeutic trial? Stroke. 2003;34(12):2856–2860. doi: 10.1161/01.STR.0000098649.39767.BC. [DOI] [PubMed] [Google Scholar]
- 2.Norris J.W., Beletsky V., Nadareishvili Z.G. Sudden neck movement and cervical artery dissection. The Canadian stroke consortium. CMAJ. 2000;163(1):38–40. [PMC free article] [PubMed] [Google Scholar]
- 3.Rubinstein S.M., Peerdeman S.M., van Tulder M.W., Riphagen I., Haldeman S. A systematic review of the risk factors for cervical artery dissection. Stroke. 2005;36(7):1575–1580. doi: 10.1161/01.STR.0000169919.73219.30. [DOI] [PubMed] [Google Scholar]
- 4.Stahmer S.A., Raps E.C., Mines D.I. Carotid and vertebral artery dissections. Emerg Med Clin North Am. 1997;15(3):677–698. doi: 10.1016/s0733-8627(05)70325-4. [DOI] [PubMed] [Google Scholar]
- 5.Dziewas R., Konrad K., Drager B., Evers S., Besselmann M., Ludemann P. Cervical artery dissection-clinical features, risk factors, therapy, and outcome in 126 patients. J Neurol. 2003;250:1179–1184. doi: 10.1007/s00415-003-0174-5. [DOI] [PubMed] [Google Scholar]
- 6.Haldeman S., Kohlbeck F.J., McGregor M. Risk factors and precipitating neck movements causing vertebrobasilar artery dissection after cervical trauma and spinal manipulation. Spine. 1999;24(8):785–794. doi: 10.1097/00007632-199904150-00010. [DOI] [PubMed] [Google Scholar]
- 7.Santos-Franco J.A., Zenteno M., Lee A. Dissecting aneurysms of the vertebrobasilar system. A comprehensive review on natural history and treatment options. Neurosurg Rev. 2008;31:131. doi: 10.1007/s10143-008-0124-x. [DOI] [PubMed] [Google Scholar]
- 8.National Institute for Health and Clinical Excellence . 2008. Clinical guideline 68: stroke. London. [Google Scholar]
- 9.Wolfson A.B., editor. 4th ed. Lippincott Williams & Wilkins; Philadelphia, PA: 2005. pp. 307–308. (Harwood-Nuss' clinical practice of emergency medicine). [Google Scholar]
- 10.Cassidy J.D., Boyle E. Risk of vertebrobasilar stroke and chiropractic care: results of a population-based case-control and case-crossover study. Spine. 2008;33(4 Suppl):S176–S183. doi: 10.1097/BRS.0b013e3181644600. [DOI] [PubMed] [Google Scholar]
- 11.Murphy D.R. Current understanding of the relationship between cervical manipulation and stroke: what does it mean for the chiropractic profession? Chiropr Osteopat. 2010;18:22. doi: 10.1186/1746-1340-18-22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Smith W.S., Johnston S.C., Skalabrin E.J., Weaver M.S., Azari P., Albers G.W. Spinal manipulative therapy is an independent risk factor for vertebral artery dissection. Neurology. 2003;60:1424–1428. doi: 10.1212/01.wnl.0000063305.61050.e6. [DOI] [PubMed] [Google Scholar]
- 13.Rothwell D.M., Bondy S.J., Williams J.I., Bousser M.G. Chiropractic manipulation and stroke: a population-based case-control study. Stroke. 2001;32:1054–1060. doi: 10.1161/01.str.32.5.1054. [DOI] [PubMed] [Google Scholar]
- 14.Lang E., Afilalo M. Vertebral artery dissection. http://emedicine.medscape.com/article/761451-overview Medscape Reference [Internet]; c1994-2011 [updated 2010 January 12; cited 2010 December 1]. Available from:
- 15.Choi S., Boyle E., Côté P., Cassidy J.D. A population-based case-series of Ontario patients who develop a vertebrobasilar artery stroke after seeing a chiropractor. J Manipulative Physiol Ther. 2011;34(1):15–22. doi: 10.1016/j.jmpt.2010.11.001. [DOI] [PubMed] [Google Scholar]
- 16.Wuest S., Symons B., Leonard T., Herzog W. Preliminary report: biomechanics of vertebral artery segments C1-C6 during cervical spinal manipulation. J Manipulative Physiol Ther. 2010;33(4):273–278. doi: 10.1016/j.jmpt.2010.03.007. [DOI] [PubMed] [Google Scholar]