

Abstract
In this article, the second part of a two-part series on rosacea, emphasis will be placed on persistent facial erythema. Despite variations in the intensity of visible redness, persistent facial erythema is a very common and consistent finding among patients with rosacea, including those with presentations classically defined as papulopustular rosacea, erythematotelangiectatic rosacea, and in many patients with phymatous rosacea. The underlying mechanisms of rosacea and their correlation with specific clinical features have been discussed in Part 1 and are referred to here where applicable. An overview of cutaneous vasculature, role of alpha-adrenoreceptors, and a discussion of available medical therapies and treatment selection are also presented, including emerging topical options for diffuse and persistent facial erythema of rosacea.
The first part of this two-part series provides a thorough update of the underlying patho-physiological mechanisms related to clinical presentations of rosacea, attempts to scientifically “connect the dots” with discussion of the likely sequence of earlier pathophysiological events, describes how clinical features manifest over time, and explains how some mechanisms may be modified by available therapies, with several reference sources provided.1–35 The relevant benefit to the clinician of understanding these mechanisms is that many correlate with specific clinical findings of rosacea, which are present in patients with diffuse facial erythema without inflammatory lesions (classically described as erythematotelangiectatic rosacea [ETR] or subypte 1), and in those with inflammatory lesions concomitant with diffuse facial erythema (classically described as papulopustular rosacea [PPR] or subypte 2).2–4,6–13,16–18,20–25,29–59 In addition, both of these presentations, especially PPR, may exhibit concurrent phymatous changes (classic subtype 3) in a subset of cases.2,16 Ocular rosacea (subtype 4) may also be present concurrently in up to one-third of patients affected by either PPR or ETR, most often presenting as blepharitis, conjunctivitis, and/or “irritated, itchy eyes” that may be misdiagnosed as ocular allergy.2,16,60 As patients with ocular involvement often do not voluntarily mention eye-related symptoms at a dermatology clinic, questioning the patient about ocular symptoms and examining the eyelids and conjunctiva assist in detecting the presence of ocular rosacea.
Manifestations of Facial Erythema of Rosacea in Clinical Practice
Any discussion of facial erythema in rosacea must first differentiate perilesional erythema that is directly related to contiguous inflammatory lesions from “background” facial erythema that occurs independent of inflammatory lesions, such as diffuse facial erythema.2,16,17,61 Perilesional erythema is defined in more detail in Part 1 of this series and also in Figure 1, which delineates perilesional erythema versus diffuse facial erythema.
Figure 1.

Perilesional Erythema vs Diffuse Facial Erythema
Despite variations in the intensity of facial redness, diffuse facial erythema, often with persistence between flares, is a very common and consistent finding among patients with rosacea, including those with presentations classically described as PPR, ETR, and in many cases of phymatous rosacea. Diffuse facial erythema present during rosacea flares and diffuse facial erythema that is persistent between rosacea flares both present similarly. The intensity of diffuse facial erythema is more likely to be greater during an exacerbation of rosacea as underlying pathogenic mechanisms are more fully operative during a flare episode. Facial erythema of rosacea, either during a flare or between periods of flaring, is most often confluent and diffuse, hence the common designation of “background erythema.”61 In the majority of cases, diffuse facial erythema exhibits central accentuation involving the inner cheeks, nose, chin, and/or mid-forehead. However, involvement of the peripheral face may also be present.
A very important clinical consideration in rosacea is that patients may present with different clinical manifestations at various timepoints.2,8,10,17,47 The classic subtype designations of rosacea, although very helpful in allowing clinicians to uniformly visualize certain core visible features, do not accurately define the presence and severity of clinical man-ifestations present in an individual patient at a given point in time. In addition, a patient may present with an overlap of man-ifestations that encompass more than one subtype designation.2,16,61,62 Figure 2 depicts a patient with three concurrent rosacea subtypes, PPR (subtype 2), ocular (subtype 4), and phymatous (subtype 3), and contrasts clinical descriptions using subtype designations versus delineation of specific manifestations present on examination of the patient.
Figure 2.

Concurrent Rosacea Subtypes
From a clinical perspective, it is also important to differentiate between the initial (baseline) presentation of rosacea and the follow-up presentations during and after treatment. At a follow-up visit, individual patients often demonstrate a good response of only some clinical features of PPR to topical therapy (i.e., metronidazole, azelaic acid) and/or oral therapy (i.e., tetracyclines, macrolides). Inflammatory lesions (i.e., papules, pustules) are often markedly reduced by proper use of appropriate topical and oral agents, with perilesional erythema also decreasing as the papular and pustular lesions resolve. However, other visible manifestations persist at a level that is bothersome to many patients, especially diffuse facial erythema (Figure 3).
Figure 3.

Change in Clinical Presentation at Follow-up
The scenario of diffuse and persistent facial erythema with central accentuation is a common clinical challenge in rosacea-affected patients who are already using recognized medical therapies, and has been described as an “unmet need” in rosacea therapy.61 Diffuse facial erythema is often persistent in patients with rosacea treated with United States Food and Drug Administration (FDA) approved and/or other recognized medical therapies where the inflammatory lesions and perilesional erythema (PPR) have responded favorably. Conventional medical therapies for rosacea, including agents FDA approved primarily for their ability to reduce inflammatory lesions in patients with PPR, also decrease overall severity of facial erythema by reducing perilesional erythema, but often have little-to-no effect on diffuse facial erythema (background erythema) that is typically persistent after inflammatory lesions clear (Figure 3).3,61,63–70
The current armamentarium of conventional medical therapies that has been used to treat PPR, including FDA-approved agents and other “off-label” therapies (i.e., oral and topical macrolides, topical clindamycin, topical calcineurin inhibitors), have not been adequately studied and/or are generally ineffective in rosacea patients with diffuse facial erythema in the absence of inflammatory lesions (classic ETR).3,61,63–72
At present, there are no topical or oral agents that are FDA approved for the ETR subtype or for facial erythema of rosacea in the absence of inflammatory lesions.
Diffuse and Persistent Facial Erythema: The Common Denominator Among Clinical Features in Rosacea
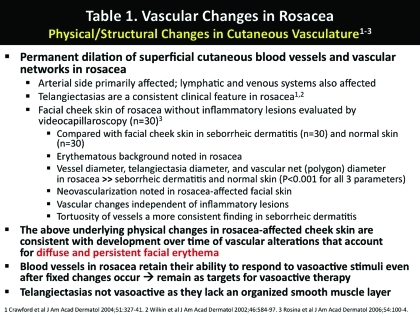
Several underlying pathogenic mech-anisms may contribute to varying degrees in producing diffuse and persistent facial erythema in patients with rosacea both with and without inflammatory lesions (Figure 4). Current research supports that augmented innate immune response and neurovascular/ neuroimmune dysregulation are pivotal components of erythema development in rosacea.7–10,13,18 Both are involved early in the pathophysiological process of rosacea promoting vasodilatory, inflammatory, and physiochemical changes, with other primary and/or downstream mechanisms also contributing to the clinical manifestations of the disease.2,4,6–13,18,23–25,29,33,34,37,41,45–47 A common underlying response in patients presenting with the visible features of PPR and ETR is vasodilation, which is associated with increased cutaneous blood flow at affected sites and enhanced reactivity to noxious heat stimuli; over time, larger-sized cutaneous vessels and neovascularization occur which lead to visibly apparent background facial erythema, with angiogenesis and neo-vascularization correlating clinically with the presence of telangiectasias (Figure 5).2,7–10,13,14,18,24 A more detailed review of pathophysiological mechanisms involved in rosacea and their possible sequence and correlation with clinical manifestations is contained in Part 1 of this two-part series. Figure 5 demonstrates the progression of vascular changes and physical alterations of cutaneous vasculature that develop over time in rosacea and their correlation with visible manifestations, including diffuse and persistent facial erythema. The clinical appearance of a given rosacea-affected patient at any point in time along this continuum is directly influenced by the rate and magnitude of development of the individual underlying changes. Table 1 depicts the physical and structural changes in cutaneous vasculature that develop in rosacea, which account for the clinical feature of diffuse facial erythema and its persistence between flares of the disease.
FIGURE 4.

Figure 5.

Pathophysiologic Vascular Changes Operative Over Time in Rosacea1–9
Table 1.
Vascular Changes in Rosacea
 |
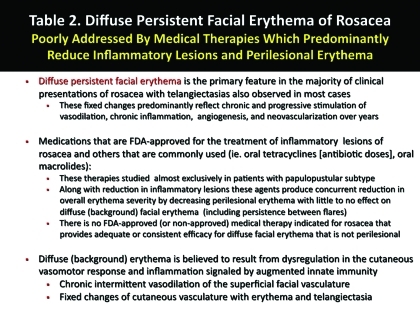
As noted above, currently available medical therapies for the common presentations of rosacea, including those that are FDA approved and those used “off label,” have been studied predominantly in patients with inflammatory lesions. Reduction in overall erythema severity in such patients relates primarily to a decrease in perilesional erythema. Although some of these agents may decrease background facial erythema that is not perilesional, this activity is modest at best in most cases. As a result, the persistence of diffuse facial erythema continues to be an “unmet need” in many patients with rosacea who desire greater reduction in facial redness. Table 2 outlines the underlying sources and clinical challenge of diffuse and persistent facial erythema.
Table 2.
Diffuse Persistent Facial Erythema of Rosacea
 |
Focus on Correlation of Clinical Features with Management and Selection of Medical Therapies
The end result of these dysregulated cutaneous functions and morphological changes that occur over time in patients with presentations consistent with the ETR or PPR subtypes is a spectrum of clinical features that is almost universally characterized by the common denominator of diffuse facial erythema.1,2,10,16,17,29 This erythema is characteristically macular or slightly edematous, confluent and bilaterally symmetric, and persistent, with ac-centuated involvement of the inner cheeks, nose, central forehead, and/or chin. Although the intensity of this erythema may increase during episodes of flaring, there is some degree of persistence during periods of clinical quiescence that varies in severity among different patients.1,2,16 Facial telangiectasias are present concurrently in almost all cases, commonly involving the inner cheeks, nose, and/or perinasal regions. Facial edema of variable magnitude is also a common finding, ranging from mild to severe based on disease activity and severity at the time of evaluation.2,10,16,17 Inflammatory lesions, although a common finding in many patients especially during a flare, are not a mandatory clinical feature of rosacea, and when present indicate the designation of PPR. Phymatous changes in rosacea (subtype 3) are relatively uncommon, develop most often in association with PPR, occur more commonly in males, and exhibit a separate gene array profile and other distinctive histological and immunohistochemical features.10 In occasional cases, phymatous changes develop in the absence of visible inflammation or clinical signs of PPR or ETR.10 Ocular rosacea (subtype 4), most often presenting as blepharitis and conjunctivitis, may be seen in association with cutaneous rosacea, including PPR and ETR, with the timing and severity of ocular and cutaneous flares independent of one another.2,60,62,68
Despite any attempts to diagnostically fit each rosacea patient into an individual subtype based on objective findings and symptomatology, overlap of clinical features and associated symptoms among different rosacea subtypes is relatively common. This is further confounded by considerable interpatient and intrapatient variability regarding the presence of and/or magnitude of both the visible clinical features and associated symptoms of rosacea at any given point in time. The clinician must ultimately evaluate what is present clinically in a given patient rather than force the patient to fit into a presumed diagnostic category.
How are conventional medical therapies utilized to reduce specific clinical features associated with common presentations of rosacea, especially FDA-approved agents? Topical metronidazole 0.75% gel, cream, and lotion twice daily; topical metronidazole 1% gel and cream once daily; azelaic acid 15% gel twice daily; and anti-inflammatory dose doxycycline (40mg modified release capsule) once daily are all FDA approved for the treatment of inflammatory lesions of rosacea (i.e., PPR subtype).73–75 These agents have been evaluated in many studies inclusive of subjects with PPR, but were not evaluated in patients without inflammatory lesions (i.e., ETR) in pivotal trials and in essentially all other studies published in the literature.3,55–57,63–70,73–78 Overall severity of facial erythema, as determined by visual assessment using a protocol-designated severity scale, has been shown to decrease with all of the FDA-approved agents used to treat PPR as well as with other agents used “off label” (i.e., antibiotic doses of tetracyclines), a finding related primarily to reduction in perilesional erythema.3,55–57,63–70,73–79 However, persistence of diffuse facial erythema is frequently noted after clearance of the inflammatory lesions and associated perilesional erythema, even in studies using combinations of topical and oral therapies for PPR.55,56,63–67,76–78,80–82
Both topical metronidazole and azelaic acid have been shown in vitro to inhibit neutrophil functions and the effects of reactive oxygen species (ROS), findings which may correlate with their efficacy in treating PPR and associated perilesional erythema.83–87 Azelaic acid in vitro (murine skin) has also been shown to decrease expression of TLR-2, cathelicidin, and KLK-5, although the magnitude of these effects with relevance to human skin awaits the results of additional studies.87 In a variety of in-vitro, ex-vivo, and in-vivo studies, tetracyclines (including anti-inflammatory dose doxycycline) have been shown to affect several mechanisms that may correlate with therapeutic efficacy in rosacea (i.e., PPR), such as inhibition of several matrix metalloproteinases (MMPs) (i.e., MMP-1, MMP-2, MMP-8, MMP-9, MMP-12, MMP-13), downregulation of several proinflammatory cytokines (i.e., tumor necrosis factor [TNF]-α, interleukin [IL]-1β, IL-8, IL-10, transforming growth factor [TGF]-β1), inhibition of neutrophil chemotaxis, inhibition of granuloma formation, inhibition of ROS, and decreased expression of nitric oxide (NO) synthases and activity of NO.3–15,22,69,70,88,89 In addition, the inhibition of MMPs by doxycycline in human skin and cultured keratinocytes has been shown to indirectly decrease serine protease (KLK-5) activity.90 This indirect reduction of serine protease activity that occurs secondary to MMP inhibition by doxycycline results in downstream prevention of the activation of the cathelicidin cascade with subsequent decrease in the breakdown of cathelicidin into its derived proinflammatory and vasoactive peptides (i.e., LL-37).7,8,18,90
Possible Explanations for the Inadequate Response of Diffuse and Persistent Facial Erythema to Conventional Medical Therapies for Rosacea
Due to a variety of potential modes of action, agents such as topical metronidazole, topical azelaic acid, and oral tetracyclines are capable of reducing some of the clinical features of rosacea, such as inflammatory lesions and perilesional erythema, and in some cases may provide some reduction in the diffuse (background) facial erythema. Although some of their modes of action might be expected to result in a greater reduction in diffuse and persistent facial erythema, this has not been supported overall by available studies and clinical experience to date (Table 2). The following are some possible explanations for the common observation of inadequate response of diffuse and persistent facial erythema to conventional medical therapies for rosacea: (1) some of the modes of action, although expected to reduce background redness, may not translate from in-vitro or ex-vivo observations in research models to positive therapeutic outcomes that are observable clinically; (2) a given mode of action of a drug may be operative in research models and in humans with rosacea; however, the potency of effect is not adequate to produce a visible clinical benefit, including when different agents are used in combination; and (3) some of the physical and structural vascular changes noted in rosacea-affected skin (i.e., enlarged vessels, thickened vessels, dilated vessels, new vessels) are already fixed before the above-mentioned medical therapies are initiated. At this point, those fixed changes in vasculature which cause diffuse and persistent facial erythema are not responsive to the modes of action of the conventional therapies discussed above.
Nevertheless, diffuse and persistent facial erythema associated with rosacea remains as a very apparent unmet medical need. Importantly, the smooth muscle-containing facial vasculature in patients with rosacea remains responsive to vasoactive stimuli, which constrict or dilate peripheral resistance vessels even when fixed structurally.2,13,71,72 As a result, a major focus of research related to this area is studies evaluating cutaneous vascular physiology and patho-physiology, adrenergic receptors, and alpha-adrenergic receptor agonists.
Structure, Function, and Physiological Receptor Modulation of Cutaneous Vasculature
Structure. The detailed structural network of the cutaneous vasculature varies among different body locations; however, the basic vessel components remain relatively constant. The vasculature of the dermis is composed of a superficial horizontal network (subpapillary plexus) located at the juncture of the papillary and reticular dermis and a deep horizontal plexus located at the juncture of the deep reticular dermis and panniculus. The superficial and deep plexuses are connected by vertically arranged vessels that course through the dermis.91 Periadnexal vasculature tends to be well developed and is usually supplied via the deep horizontal plexus, with networks forming around hair follicles and sweat glands. Cutaneous nerves and lymphatics are closely associated with the vessels of this entire network. The subpapillary plexus contains a network of smaller vessels, including post-capillary venules, end arterioles, and capillaries, which supply the dermal papillae. The deep horizontal plexus contains vessels of larger caliber than the subpapillary plexus, including distal resistance vessels that are primarily modulated by peripheral sympathetic (adrenergic) innervation.92
Function. In healthy skin under normal physiological conditions, in addition to providing oxygen and nutrients, the cutaneous vasculature serves a very important homeostatic role in temperature regulation, acting as a radiator (vasodilation) or insulator (vasoconstriction) in order to maintain proper core body temperature.92 Modification and distribution of blood flow is influenced by several factors, including response to postural changes, chemo-reception, and baroreflex response. However, central temperature exerts a dominant influence on reflex alterations of blood flow both centrally and peripherally (reflex thermoregulatory control), with both the arterial and venous systems under the influence of sympathetic adrenergic modulation.71,92 In addition to thermo-regulatory reflex control, local changes in temperature are capable of inducing maximal vasodilation or vasoconstriction via adrenergic, endothelial, and sensory mech-anisms, including via modifications of NO-induced vasodilation and α2-adrenoreceptor upregulation.93
Adrenergic receptors (adrenoreceptors). Regulation of the cutaneous vascular system is highly complex and is mediated primarily by the sympathetic nervous system. Based primarily on animal research, the current model of adrenoreceptors that modulate vasculature include six α-receptor subtypes and three β-receptor subtypes, with two conformational variants also noted.71,72,94–98 Contraction of peripheral vascular smooth muscle is primarily mediated by α-receptor subtypes, with specific receptor subtypes sometimes differing in distribution, function, and affinities for specific stimuli or exogenous agonists.95–97 Also, contracture of smooth muscle, such as in small peripheral arteriolar resistance vessels and venules, is mediated by more than one α-adrenoreceptor subtype, with the majority of ligands capable of recognizing multiple receptor subtypes.95 Although there may be variability among different anatomic regions, multiple studies in several species have demonstrated contraction of peripheral vasculature (vasoconstriction) mediated by α1A- and α1D-adrenoreceptor subtypes. Other studies have shown vasoconstriction of small distal resistance arteries via postsynaptic α2-adrenoreceptor stimulation of vascular smooth muscle, with some experimental models noting the importance of α2A/D- and α2B-adrenoreceptor subtypes in the arterial compartment and α2A/D- and α2C-adrenoreceptor subtypes in the venular compartment of the vascular network.71,94–97 In addition, vasoconstriction related to local skin cooling appears to be induced at least partially by postsynaptic α2C-adrenoreceptor upregulation.93 With both α1- and α2-adrenoreceptor stimulation inducing contraction of vascular smooth muscle, the potential for variability in anatomic distribution of receptors, and the ability of multiple adrenoreceptor subtypes to induce a specific function, it is not clear whether or not selective stimulation or inhibition of individual adrenoreceptor subtypes will produce clinically relevant or predictable outcomes.
Emerging Topical Approaches to Diffuse Persistent Facial Erythema in Rosacea
As explained above, persistent facial erythema, especially when diffuse (background erythema), is a significant unmet need among the currently available conventional topical and systemic medical options for the treatment of rosacea, especially the common presentations.68 In fact, discussions in the literature of the FDA-approved agents and non-FDA-approved medical therapies (i.e., topical pimecrolimus, topical tacrolimus, topical retinoids, antibiotic doses of oral tetracycline agents, oral macrolides, oral metronidazole, oral isotretinoin) for rosacea rarely address any recognized treatment for the background erythema that persists after inflammatory lesions and perilesional erythema resolve.3,22,57,63,67,68,70–72,99–107 The bottom line is that there is a conspicuous absence of medical therapeutic options for the treatment of diffuse and persistent erythema of rosacea.
α-Adrenoreceptor agonists. Most recently, α-adrenoreceptor agonists (α-agonists) are under evaluation for treatment of diffuse facial erythema associated with rosacea due to their involvement in neurovascular regulation and their ability to reversibly constrict peripheral vasculature (Figure 6).13,92,94–97 Topical application of oxymetazoline 0.05% solution once daily or xylometazoline 0.05% solution once daily have both been shown in case reports to reduce diffuse facial erythema in adult patients with ETR that were unresponsive to several topical therapies and oral antibiotics.71,72 The primary mechanism of diffuse facial erythema reduction with these two agents when applied topically appears to be vasocontriction of peripheral cutaneous arterial vessels primarily through their α1-agonist activity.71,72 Xylometazoline and oxymetazoline (a structural derivative of xylometazoline) are reported to be highly selective for the α1A-adrenoreceptor and partially selective for the α2A-adrenoreceptor.71,72
Figure 6.

Mode of action in cutaneous vasculature of αAdrenergic Receptor Agonists
Both oxymetazoline 0.05% solution and xylometazoline 0.05% solution are not currently FDA approved for treatment of rosacea, including for any symptoms or signs (i.e., erythema), but are commercially available as nasal decongestant formulations that were applied by patients treated for ETR in published case reports.71,72 Large-scale randomized controlled trials are needed in order to fully evaluate dose-response patterns, efficacy, tolerability, and safety with the use of oxymetazoline or xylometazoline for the topical treatment of diffuse facial erythema of rosacea, including evaluation of possible tachyphylaxis, and/or rebound. The latter two assessment parameters are important as tachyphylaxis and rebound (rhinitis medicamentosa) have been associated with the use of α-adrenergic nasal decongestant formulations prompting cautious recommendations to avoid overuse with multiple applications each day and repeated use beyond three consecutive days to nasal mucosa.108,109
The clinical relevance to rosacea therapy of tachyphylaxis and nasal mucosal rebound reported with the use of α-agonist nasal decongestants for rhinitis (such as xylometazoline and oxymetazoline) is not currently known. In the three patients with ETR treated topically with oxymetazoline 0.05% solution once daily (N=2) and xylometazoline 0.05% solution once daily (N=1), reduction in facial erythema was observed within 1 to 3 hours, persisted throughout the day, and continued to remain effective with use over eight months (2 patients, 1 oxymetazoline, 1 xylometazoline) and 17 months (1 patient, oxymetazoline). However, whether or not there is a potential for tachyphylaxis or rebound to occur after controlled repeated application of selective α1-agonists to human skin awaits results from large-scale clinical trials, especially in subjects with rosacea who exhibit diffuse facial erythema. In addition, dose-response patterns need to be determined to assess optimal concentration and frequency of application. At present, topical oxymetazoline is currently undergoing controlled studies evaluating its use in subjects with rosacea.
Another α-agonist that is currently under study for the treatment of facial erythema of rosacea is brimonidine tartrate. Brimonidine tartrate is a highly selective α2-adrenoreceptor agonist that is also not currently FDA approved for the treatment of rosacea, though it is FDA approved as an ophthalmic solution (0.1% and 0.15%) for the treatment of increased intraocular pressure in patients with open angle glaucoma.110 Peripheral vasoconstriction induced by topical application of brimonidine tartrate is reported to occur due to highly selective α2-adrenoreceptor agonist activity (Figure 7).111,112 Two randomized, double-blind, vehicle-controlled Phase 2 studies (Study A and Study B) have been completed evaluating primarily once-daily application of brimonidine tartrate gel for moderate-to-severe facial erythema in adults with rosacea (Figure 7).111 In both studies, patients with rosacea and diffuse facial erythema were enrolled; however, those with Ž3 inflammatory lesions were excluded to avoid the influence of perilesional erythema as a confounding variable.
Figure 7.

Mode of Action in Cutaneous Vasculature of Topic α2-Adrenergic Receptor Agonist in Rosacea
In the Phase 2a dose-response study (Study A, N=122), it was found that a single application of brimonidine tartrate gel (0.5% vs. 0.18% vs. 0.07% vs. vehicle) reduced diffuse facial erythema in a dose-dependent manner over 12 hours as compared to vehicle based on investigator assessments, subject assessments, and chromameter examinations.111 Brimonidine tartrate 0.5% gel exhibited the greatest magnitude of erythema reduction at all time points over 12 hours, which was statistically significant versus vehicle in achieving a 2-grade improvement in erythema by both investigator and subject assessments and by median change in chromameter values (P<0.001). The onset of reduction in erythema occurred within 30 minutes. The peak effect lasted for 4 to 6 hours, covering a duration of peak activity from two hours through eight hours after a single application. As the peak effect started to wane, the erythema progressively reappeared but did not return to the baseline level even at the last time point of evaluation (12 hours). Exacerbation of rosacea (i.e., increase in facial erythema, increase in inflammatory lesions, increase in telangiectasia severity) was not observed and the safety and skin tolerability profile of brimonidine tartrate gel (up to 0.5%) was favorable.111
A Phase 2b dose-response study (Study B, N=269) evaluated application of brimonidine tartrate gel once daily (0.5%, 0.18%, vehicle) and twice daily (0.18%, vehicle) for four weeks, followed by a four-week post-treatment phase.111 As in Study A, adult patients with rosacea defined as moderate-to-severe facial erythema and 2 inflammatory lesions were enrolled. The greatest efficacy in erythema reduction based on both physician and subject assessments was with brimonidine 0.5% gel once daily, which demonstrated efficacy results consistent with what was observed in Study A. Importantly, erythema reduction after 28 days of daily use of brimonidine tartrate 0.5% gel was the same or better than what was achieved on Day 1 of the study, with results significantly superior to vehicle (P<0.001).111 Thus, tachyphylaxis was not observed over at least 28 days of daily use, and worsening of inflammatory lesion counts or telangiectasia severity did not occur over the course of the study. Over the four-week post-treatment phase, clinically relevant rebound (aggravation of facial erythema) was not noted. Safety assessments completed during the course of the study indicated that brimonidine tartrate at all concentrations and application frequencies studied, was safe and well tolerated, including assessments of skin tolerability, intraocular pressure, blood pressure, and heart rate.111
The results from the Phase 2a and Phase 2b studies with brimonidine tartrate gel for facial erythema of rosacea are promising; however, additional studies (i.e., Phase 3) will assist in gathering additional information on the efficacy and safety of this agent in rosacea.
Physical Modalities for Diffuse and Persistent Facial Erythema and Telangiectasias of Rosacea
Although this article emphasizes medical therapy options, a variety of physical modalities have been used with success for the treatment of diffuse facial erythema of rosacea in patients with very few or no inflammatory lesions (i.e., ETR) and for facial telangiectasias. The commonly used description, “physical modalities,” is very general and refers to a wide variety of laser and light-based therapies as well as other technologies. Published studies have incorporated intense pulsed light, pulsed dye laser, and nonpurpuragenic pulsed dye laser for the treatment of facial erythema and telangiectasias in patients with ETR, with reduction in facial erythema, decrease in telangiectasias, improvement in symptomatology, and a favorable impact on quality-of-life parameters reported.113–118 Interestingly, a small study (N=10) of patients with PPR demonstrated that use of the flashlamp pulsed dye laser was of limited value for treatment of papulopustular lesions.119
Concluding Remarks
In this two-part article series, several underlying pathophysiological mechanisms were correlated with common clinical manifestations of rosacea, with early mechanisms defined by several more recent research findings. Both augmented innate immune response and neurovascular/neuroimmune dysregulation appear to work in concert in signaling into motion the underlying vasodilation and cascades of inflammation, which produce intermittent flares of diffuse facial erythema. In some cases, inflammatory lesions develop, likely related at least partially to the chemoattractant effects of IL-8 and LL-37. Over time, several factors including MMP upregulation with dermal matrix degradation, chronic vascular inflammation with perivascular edema, and downstream cascades signaled by cathelicidin-derived peptides (i.e., long form LL-37) stimulate structural changes in cutaneous vasculature. These structural changes progress to become fixed, characterized by larger and more dilated superficial cutaneous vessels and arborizing networks, leading to persistence of facial erythema, which is usually diffuse and central facial in accentuation. Telangiectasias also develop due to neovascularization. These changes occur in varying degrees with regard to magnitude and time course of development. Nevertheless, the diffuse facial erythema transcends from being almost entirely intermittent to a persistent baseline level of background erythema, which may still be intermittently exacerbated by episodic flares of rosacea.
Other factors appear to contribute to facial erythema of rosacea, including stratum corneum permeability barrier impairment and depletion of cutaneous antioxidant reserve by ROS, the latter induced in some cases by ultraviolet-related photodamage. As a result, proper skin care (gentle cleanser use, moisturization) and photoprotection are integral components of the management of rosacea.
As some of the available conventional medical therapies for rosacea are capable of counteracting augmented innate immune response by inhibiting steps involved in cathelicidin processing, it is not entirely clear why these agents would not reduce diffuse facial erythema. It may be because these agents are initiated after structural changes in cutaneous vasculature have already become fixed. Is it possible that very early use of conventional agents, such as topical metronidazole, topical azelaic acid, and/or anti-inflammatory-dose doxycycline could mitigate the development of fixed vascular changes if these therapies were used long term? The answer is hard to determine without substantiation through well-designed clinical studies. Nevertheless, several currently available therapies are effective in decreasing inflammatory lesions and perilesional erythema.
The α-agonists provide hope that a topical therapy may soon be available for reduction of diffuse facial erythema of rosacea. Early results are favorable; however, additional data are needed with more studies ongoing. If any of these agents achieve FDA approval for rosacea, additional information from clinical studies should help clinicians better understand the optimal application of these agents for diffuse facial erythema and how to incorporate them into the overall management of rosacea based on the clinical features present in each case.
Footnotes
DISCLOSURE:Dr. Del Rosso is a consultant, speaker, and/or researcher for Coria/Valeant, Allergan, Galderma, Graceway, Intendis, Medicis, Onset Dermatologics, Obagi Medical Products, Ortho Dermatologics, PharmaDerm/Nycomed, Promius, Ranbaxy, Stiefel/GSK, TriaBeauty, Triax, Unilever, and Warner-Chilcott.
REFERENCES
- 1.Marks R. The enigma of rosacea. J Dermatol Treat. 2007;18:326–328. doi: 10.1080/09546630701485233. [DOI] [PubMed] [Google Scholar]
- 2.Crawford GH, Pelle MT, James WD. Rosacea I: etiology, pathogenesis, and subtype classification. J Am Acad Dermatol. 2004;51:327–341. doi: 10.1016/j.jaad.2004.03.030. [DOI] [PubMed] [Google Scholar]
- 3.Pelle MT, Crawford GH, James WD. Rosacea II: therapy. J Am Acad Dermatol. 2004;51:499–512. doi: 10.1016/j.jaad.2004.03.033. [DOI] [PubMed] [Google Scholar]
- 4.Del Rosso JQ. Update on rosacea pathogenesis and correlation with medical therapeutic agents. Cutis. 2006;78:97–100. [PubMed] [Google Scholar]
- 5.Sapadin AN, Fleischmajer R. Tetracyclines: non-antibiotic properties and their clinical implications. J Am Acad Dermatol. 2006;54:258–265. doi: 10.1016/j.jaad.2005.10.004. [DOI] [PubMed] [Google Scholar]
- 6.Bevins CL, Liu FT. Rosacea: skin innate immunity gone awry? Nat Med. 2007;13(8):904–906. doi: 10.1038/nm0807-904. [DOI] [PubMed] [Google Scholar]
- 7.Yamasaki K, Di Nardo A, Bardan A, et al. Increased serine protease activity and cathelicidin promotes skin inflammation in rosacea. Nat Med. 2007;13(8):975–980. doi: 10.1038/nm1616. [DOI] [PubMed] [Google Scholar]
- 8.Yamasaki K, Gallo RL. The molecular pathology of rosacea. J Dermatol Sci. 2009;55(2):77–81. doi: 10.1016/j.jdermsci.2009.04.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Fleischer AB. Inflammation in rosacea and acne: implications for patient care. J Drugs Dermatol. 2011;10:614–620. [PubMed] [Google Scholar]
- 10.Steinhoff M, Buddenkotte J, Aubert J, et al. Clinical, cellular, and molecular aspects in the pathophysiology of rosacea. J Invest Dermatol. 2011;15:2–11. doi: 10.1038/jidsymp.2011.7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Meyer-Hoffert U, Schroder JM. Epidermal proteases in the pathogenesis of rosacea. J Invest Dermatol. 2011;15:16–23. doi: 10.1038/jidsymp.2011.2. [DOI] [PubMed] [Google Scholar]
- 12.Gerber PA, Buhren BA, Steinhoff M, et al. Rosacea: the cytokine and chemokine network. J Invest Dermatol. 2011;15:40–47. doi: 10.1038/jidsymp.2011.9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Schwab VD, Sulk M, Seeliger S, et al. Neurovascular and neuroimmune aspects in the pathophysiology of rosacea. J Invest Dermatol. 2011;15:53–62. doi: 10.1038/jidsymp.2011.6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Rosina P, Zamperetti M, Giovannini A, et al. Video-capillaroscopic alterations in erythematotelangiectatic rosacea. J Am Acad Dermatol. 2006;54:100–104. doi: 10.1016/j.jaad.2005.10.009. [DOI] [PubMed] [Google Scholar]
- 15.Jang YH, Sim JH, Kang HY, et al. Immunohistochemical expression of matrix metalloproteinases in the granulomatous rosacea compared with the non-granulomatous rosacea. J Eur Acad Dermatol Venereol. 2011;25:544–548. doi: 10.1111/j.1468-3083.2010.03825.x. [DOI] [PubMed] [Google Scholar]
- 16.Wilkin J, Dahl M, Detmar M, et al. Standardized classification system of rosacea: report of the National Rosacea Society Expert Committee on the classification and staging of rosacea. J Am Acad Dermatol. 2002;46:584–587. doi: 10.1067/mjd.2002.120625. [DOI] [PubMed] [Google Scholar]
- 17.Wilkin J, Dahl M, Detmar M, et al. Standard grading system for rosacea: report of the National Rosacea Society Expert Committee on the classification and staging of rosacea. J Am Acad Dermatol. 2004;50:907–912. doi: 10.1016/j.jaad.2004.01.048. [DOI] [PubMed] [Google Scholar]
- 18.Yamasaki K, Gallo RL. Rosacea as a disease of cathelicidins and skin innate immunity. J Invest Dermatol. 2011;15:53–62. doi: 10.1038/jidsymp.2011.4. [DOI] [PubMed] [Google Scholar]
- 19.De Y, Chen Q, Schmidt AP, et al. LL-37, the neutrophil granule- and epithelial cell-derived cathelicidin, utilizes formyl peptide receptor-like 1 (FPRL-1) as a receptor to chemoattract human peripheral blood neutrophils, monocytes, and T cells. J Exp Med. 2000;192:1069–1074. doi: 10.1084/jem.192.7.1069. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Koczulla R, von Degenfeld G, Kupatt C, et al. An angiogenic role for the human peptide antibiotic LL-37/hCAP-18. J Clin Invest. 2003;111:1665–72. doi: 10.1172/JCI17545. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Park HJ, Cho DH, Kim HJ, et al. Collagen synthesis is suppressed in dermal fibroblasts by the human antimicrobial peptide LL-37. J Invest Dermatol. 2009;129:843–50. doi: 10.1038/jid.2008.320. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Korting HC, Schollmann C. Tetracycline actions relevant to rosacea treatment. Skin Pharmacol Physiol. 2009;22:287–294. doi: 10.1159/000235550. [DOI] [PubMed] [Google Scholar]
- 23.Gomaa AH, Yaar M, Eyada MM, et al. Lymphangiogenesis and angiogenesis in non-phymatous rosacea. J Cutan Pathol. 2007;34:748–755. doi: 10.1111/j.1600-0560.2006.00695.x. [DOI] [PubMed] [Google Scholar]
- 24.Guzman-Sanchez DA, Ishiuji Y, et al. Enhanced skin blood flow and sensitivity to noxious heat stimuli in papulopustular rosacea. J Am Acad Dermatol. 2007;57:800–805. doi: 10.1016/j.jaad.2007.06.009. [DOI] [PubMed] [Google Scholar]
- 25.Huggenberger R, Detmar M. The cutaneous vascular system in chronic skin inflammation. J Invest Dermatol. 2011;15:24–32. doi: 10.1038/jidsymp.2011.5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Tjabringa GS, Aarbiou J, Ninaber DK, et al. The antimicrobial peptide LL-37 activates innate immunity at the airway epithelial surface by transactivation of the epidermal growth factor receptor. J Immunol. 2003;171:6690–6696. doi: 10.4049/jimmunol.171.12.6690. [DOI] [PubMed] [Google Scholar]
- 27.Tokumaru S, Sayama K, Skirakata Y, et al. Induction of keratinocyte migration via transactivation of the epidermal growth factor receptor by the antimicrobial peptide LL-37. J Immunol. 2005;175:4662–4668. doi: 10.4049/jimmunol.175.7.4662. [DOI] [PubMed] [Google Scholar]
- 28.Detmar M, Brown LF, Claffey KP, et al. Overexpression of vascular permeability factor/vascular endothelial growth factor and its receptors in psoriasis. J Exp Med. 1994;180:1141–1146. doi: 10.1084/jem.180.3.1141. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Bamford JTM. Rosacea: current thoughts on origin. Semin Cutan Med Surg. 2001;20:199–206. doi: 10.1053/sder.2001.27553. [DOI] [PubMed] [Google Scholar]
- 30.Steinhoff M, Stander S, Seelinger S, et al. Modern aspects of cutaneous neurogenic inflammation. Arch Dermatol. 2003;139:479–488. doi: 10.1001/archderm.139.11.1479. [DOI] [PubMed] [Google Scholar]
- 31.Cevikbas F, Steinhoff A, Homey B, et al. Neuroimmune interactions in allergic skin diseases. Curr Opin Allergy Clin Immunol. 2007;7:365–373. doi: 10.1097/ACI.0b013e3282a644d2. [DOI] [PubMed] [Google Scholar]
- 32.Lazaridou E, Giannopoulou C, Fotiadou C, et al. The potential role of microorganisms in the development of rosacea. J Dtsch Dermatol Ges. 2011;9:21–25. doi: 10.1111/j.1610-0387.2010.07513.x. [DOI] [PubMed] [Google Scholar]
- 33.Yamasaki K, Kanada K, Macleod DT, et al. TLR2 expression is increased in rosacea and stimulates enhanced serine protease production by keratinocytes. J Invest Dermatol. 2011;131:688–697. doi: 10.1038/jid.2010.351. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Dirschka T, Tronnier H, Folster-Holst R. Epithelial barrier function and atopic diathesis in rosacea and perioral dermatitis. Br J Dermatol. 2004;150:1136–1141. doi: 10.1111/j.1365-2133.2004.05985.x. [DOI] [PubMed] [Google Scholar]
- 35.Draelos ZD. Treating beyond the histology of rosacea. Cutis. 2004;74(suppl 3):28–31. [PubMed] [Google Scholar]
- 36.Torok HM. Rosacea skin care. Cutis. 2000;66(4 Suppl):14–16. [PubMed] [Google Scholar]
- 37.McAleer MA, Fitzpatrick P, Powell FC. Papulopustular rosacea: prevalence and relationship to photodamage. J Am Acad Dermatol. 2010;63:33–39. doi: 10.1016/j.jaad.2009.04.024. [DOI] [PubMed] [Google Scholar]
- 38.Martin DB, Gaspari AA. Toll-like receptors. In: Gaspari AA, Tyring SK, editors. Clinical and Basic Immunology. London: Springer-Verlag; 2008. pp. 67–84. [Google Scholar]
- 39.Hansen C, Leitenberger JJ, Jacobe HT, et al. Photoimmunology. In: Gaspari AA, Tyring SK, editors. Clinical and Basic Immunology. London: Springer-Verlag; 2008. pp. 147–155. [Google Scholar]
- 40.Chung J, Cho S, Kang S. Why does the skin age? Intrinsic aging, photoaging, and their pathophysiology. In: Rigel DS, Weiss RA, Lim HW, Dover JS, editors. Photoaging. New York: Marcel Dekker; 2004. pp. 1–13. [Google Scholar]
- 41.Neumann E, Frithz A. Capillaropathy and capillaroneogenesis in the pathogenesis of rosacea. Int J Dermatol. 1998;37:263–266. doi: 10.1046/j.1365-4362.1998.00275.x. [DOI] [PubMed] [Google Scholar]
- 42.Lundwall A, Brattsand M. Kallikrein-related peptidases. Cell Mol Life. 2008;65:2019–2038. doi: 10.1007/s00018-008-8024-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Sotiropoulo G, Pampalakis G, Diamandis EP. Functional roles of human kallikrein-related peptidases. J Biol Chem. 2009;284:32989–32994. doi: 10.1074/jbc.R109.027946. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Lefkove BA, Fried LE, Arbiser JL. Angiogenesis for the clinician. In: Gaspari AA, Tyring SK, editors. Clinical and Basic Immunology. London: Springer-Verlag; 2008. pp. 157–168. [Google Scholar]
- 45.Oztas MO, Balk M, Ogus E, et al. The role of free radicals in the aetiopathogenesis of rosacea. Clin Exp Dermatol. 2003;28:188–192. doi: 10.1046/j.1365-2230.2003.01179.x. [DOI] [PubMed] [Google Scholar]
- 46.Tisma VS, Basta-Juzbasic A, Jaganjac M, et al. Oxidative stress and ferritin expression in the skin of rosacea patients. J Am Acad Dermatol. 2009;60:270276. doi: 10.1016/j.jaad.2008.10.014. [DOI] [PubMed] [Google Scholar]
- 47.McAleer MA, Lacey N, Powell FC. The pathophysiology of rosacea. G Ital Dermatol Venereol. 2009;144:663–671. [PubMed] [Google Scholar]
- 48.Bielenberg DR, Bucana CD, Sanchez R, et al. Molecular regulation of UVB-induced cutaneous angiogenesis. J Invest Dermatol. 1998;111:864–872. doi: 10.1046/j.1523-1747.1998.00378.x. [DOI] [PubMed] [Google Scholar]
- 49.Karincaoglu Y, Bayram N, Aycan O, et al. The clinical importance of Demodex folliculorum presenting with nonspecific facial signs and symptoms. J Dermatol. 2004;31:618–626. doi: 10.1111/j.1346-8138.2004.tb00567.x. [DOI] [PubMed] [Google Scholar]
- 50.Forstinger C, Kittler H, Binder M. Treatment of rosacea-like demodicidosis with oral ivermectin and topical permethrin cream. J Am Acad Dermatol. 1999;41:775–777. doi: 10.1016/s0190-9622(99)70022-8. [DOI] [PubMed] [Google Scholar]
- 51.Larios G, Alevizos A, Perimeni D, et al. Rosacea-like demodicidosis. Lancet Infect Dis. 2008;8:804. doi: 10.1016/S1473-3099(08)70283-4. [DOI] [PubMed] [Google Scholar]
- 52.Segal R, Mimouni D, Feuerman H, et al. Dermoscopy as a diagnostic tool in demodicidosis. Int H Dermatol. 2010;49:1018–1023. doi: 10.1111/j.1365-4632.2010.04495.x. [DOI] [PubMed] [Google Scholar]
- 53.Bikowski JB, Del Rosso JQ. Demodex dermatitis: a retrospective analysis of clinical diagnosis and successful treatment with topical crotamiton. J Clin Aesthet Dermatol. 2009;2:20–25. [PMC free article] [PubMed] [Google Scholar]
- 54. Bonamigo RR, Bakos L, Edelweiss M, et al. Could matrix metalloproteinase-9 be a link between Demodex folliculorum and rosacea? J Eur Dermatol Venereol. 2005. 19 646 647 [DOI] [PubMed] [Google Scholar]
- 55.Thibotout D, Thieroff-Ekerdt R, Graupe K. Efficacy and safety of azelaic acid (15%) gel as a new treatment for papulopustular rosacea: results from two vehicle-controlled randomized phase III studies. J Am Acad Dermatol. 2003;48:836–845. doi: 10.1067/mjd.2003.308. [DOI] [PubMed] [Google Scholar]
- 56.Elewski B, Fleischer AB, Pariser DM, et al. A comparison of 15% azelaic acid gel and 0.75% metronidazole gel in the topical treatment of papulopustular rosacea. Arch Dermatol. 2003;139:1444–50. doi: 10.1001/archderm.139.11.1444. [DOI] [PubMed] [Google Scholar]
- 57.Del Rosso JQ, Baum EW. Comprehensive medical management of rosacea: an interim study report and literature review. J Clin Aesthetic Dermatol. 2008;1:20–25. [PMC free article] [PubMed] [Google Scholar]
- 58.Subramanyan K. Role of mild cleansing in the management of patient skin. Dermatol Ther. 2004;17(4 suppl):26–34. doi: 10.1111/j.1396-0296.2004.04s1003.x. [DOI] [PubMed] [Google Scholar]
- 59.Elias PM. The skin barrier as an innate immune element. Semin Immunopath. 2007;29:3–14. doi: 10.1007/s00281-007-0060-9. [DOI] [PubMed] [Google Scholar]
- 60.Quarterman MJ, Johnson DW, Abela DC, et al. Ocular rosacea: signs, symptoms, and tear studies before and after treatment with doxycycline. Arch Dermatol. 1997;133:49–54. doi: 10.1001/archderm.133.1.49. [DOI] [PubMed] [Google Scholar]
- 61.Odom RDahl M, Dover J, et al. Standard management options for rosacea, part 1: overview and broad spectrum of care. Cutis. 2009;84:43–47. [PubMed] [Google Scholar]
- 62.Bae YI, Yun SJ, Lee JB, et al. Clinical evaluation of 168 Korean patients with rosacea: the sun exposure correlates with the erythematotelangiectatic subtype. Ann Dermatol. 2009;21:243–249. doi: 10.5021/ad.2009.21.3.243. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Del Rosso JQ. Medical treatment of rosacea with emphasis on topical therapies. Expert Opin Pharmacother. 2004;5:5–13. doi: 10.1517/14656566.5.1.5. [DOI] [PubMed] [Google Scholar]
- 64.McClellan KJ, Noble S. Topical metronidazole: a review of its uses in rosacea. Am J Clin Dermatol. 2000;1:191–199. doi: 10.2165/00128071-200001030-00007. [DOI] [PubMed] [Google Scholar]
- 65.Frampton JE, Wagstaff AJ. Azelaic acid 15% gel in the treatment of papulopustular rosacea. Am J Clin Dermatol. 2004;5:57–64. doi: 10.2165/00128071-200405010-00009. [DOI] [PubMed] [Google Scholar]
- 66.Liu RH, Smith MK, Basta SA, et al. Azelaic acid in the treatment of papulopustular rosacea: a systematic review of randomized controlled trials. Arch Dermatol. 2006;142:1047–1052. doi: 10.1001/archderm.142.8.1047. [DOI] [PubMed] [Google Scholar]
- 67.Del Rosso JQ, Baldwin H, Webster G. American Acne & Rosacea Society rosacea medical management guidelines. J Drugs Dermatol. 2008;7:531–533. [PubMed] [Google Scholar]
- 68.Odom RDahl M, Dover J, et al. Standard management options for rosacea, part 2: options according to rosacea subtype. Cutis. 2009;84:97–104. [PubMed] [Google Scholar]
- 69.Del Rosso JQ, Webster GW, Jackson M, et al. Two randomized phase II clinical trials evaluating anti-inflammatory dose doxycycline (40-mg doxycycline, USP capsules) administered once daily for treatment of rosacea. J Am Acad Dermatol. 2007;56:791–801. doi: 10.1016/j.jaad.2006.11.021. [DOI] [PubMed] [Google Scholar]
- 70.Kennedy Carney C, Cantrell W, Elewski BE. Rosacea: a review of current topical, systemic and light based therapies. G Ital Dermatol Venereol. 2009;144:673–688. [PubMed] [Google Scholar]
- 71.Shanler SD, Ondo AL. Successful treatment of erythema and flushing of rosacea using a topically applied selective alpha1-adrenergic receptor antagonist, oxymetazoline. Arch Dermatol. 2007;143:1369–1371. doi: 10.1001/archderm.143.11.1369. [DOI] [PubMed] [Google Scholar]
- 72.Kim JH, Oh YS, Ji JH, et al. Rosacea (erythemato-telangiectatic type) effectively improved by topical xylometazoline. J Dermatol. 2011;38:510–513. doi: 10.1111/j.1346-8138.2010.00999.x. [DOI] [PubMed] [Google Scholar]
- 73.Fort Worth, Texas: Galderma Laboratories LP; Metrogel 1% Gel [package insert] [Google Scholar]
- 74.Morristown, New Jersey: Bayer Dermatology Division (formerly Intendis); 2010. Finacea Gel [package insert] [Google Scholar]
- 75.Fort Worth, Texas: Galderma Laboratories LP; Oracea Capsules [package insert] [Google Scholar]
- 76.Del Rosso JQ. Anti-inflammatory dose doxycycline in the treatment of rosacea. J Drugs Dermatol. 2009;8:664–668. [PubMed] [Google Scholar]
- 77.Webster GF. An open-label, community-based, 12-week assessment of the effectiveness and safety of monotherapy with doxycycline 40 mg (30-mg immediate-release and 10-mg delayed-release beads) Cutis. 2010;86(5 Suppl):7–15. [PubMed] [Google Scholar]
- 78.Del Rosso JQ, Bhatia N. Azelaic acid gel 15% in the management of papulopustular rosacea: a status report on available efficacy data and clinical application. Cutis. 2011;88:67–72. [PubMed] [Google Scholar]
- 79.Gupta AK, Chaudhry MM. Critical review of the manner in which the efficacy of therapies for rosacea are evaluated. Int J Dermatol. 2003;42:909–916. doi: 10.1046/j.1365-4362.2003.01861.x. [DOI] [PubMed] [Google Scholar]
- 80.Fowler JF., Jr Combined effect of anti-inflammatory dose doxycycline (40-mg doxycycline, usp monohydrate controlled-release capsules) and metronidazole topical gel 1% in the treatment of rosacea. J Drugs Dermatol. 2007;6:641–645. [PubMed] [Google Scholar]
- 81.Del Rosso JQ, Schlessinger J, Werschler P. Comparison of anti-inflammatory dose doxycycline versus doxycycline 100 mg in the treatment of rosacea. J Drugs Dermatol. 2008;7:573–576. [PubMed] [Google Scholar]
- 82.Del Rosso JQ, Bruce S, Jarratt M, et al. Efficacy of topical azelaic acid (AzA) gel 15% plus oral doxycycline 40 mg versus metronidazole gel 1% plus oral doxycycline 40 mg in mild-to-moderate papulopustular rosacea. J Drugs Dermatol. 2010;9:607–613. [PubMed] [Google Scholar]
- 83.Miyachi Y. Potential antioxidant mechanism of action for metronidazole: implications for rosacea management. Adv Ther. 2001;18:237–243. doi: 10.1007/BF02850193. [DOI] [PubMed] [Google Scholar]
- 84.Narayanan S, Hünerbein A, Getie M, et al. Scavenging properties of metronidazole on free oxygen radicals in a skin lipid model system. J Pharm Pharmacol. 2007;59:1125–30. doi: 10.1211/jpp.59.8.0010. [DOI] [PubMed] [Google Scholar]
- 85.Akamatsu, H, Oguchi, M, Nishijima S, et al. The inhibition of free radical generation by human neutrophils through the synergistic effects of metronidazole with palmitoleic acid: a possible mechanism of action of metronidazole in rosacea and acne. Arch Dermatol.Res. 1990;282:449–454. doi: 10.1007/BF00402621. [DOI] [PubMed] [Google Scholar]
- 86.Akamatsu, H, Komura J, Asada Y, et al. Inhibitory effect of azelaic acid on neutrophil functions: a possible cause for its efficacy in treating pathogenetically unrelated disease. Arch Dermatol Res. 1991;283:162–166. doi: 10.1007/BF00372056. [DOI] [PubMed] [Google Scholar]
- 87. Yamasaki K, Gallo RK, et al. Effect of azelaic acid on cathelicidin and serine protease expression. Presented at: Fall Clinical Dermatology Conference; October 15-18 2009; Las Vegas, NV. [Google Scholar]
- 88.Webster G, Del Rosso JQ. Anti-inflammatory activity of tetracyclines. Dermatol Clin. 2007;25:122–135. doi: 10.1016/j.det.2007.01.012. [DOI] [PubMed] [Google Scholar]
- 89.Golub LM, Lee HM, Ryan ME, et al. Tetracyclines inhibit connective tissue breakdown by multiple nonantimicrobial mecahanisms. Adv Derm Res. 1998;12:12–26. doi: 10.1177/08959374980120010501. [DOI] [PubMed] [Google Scholar]
- 90.Kanada KN, Nakatsuji T, Gallo RL. Doxycycline indirectly inhibits proteolytic activation of tryptic kallikrein-related peptidases and activation of cathelicidin. J Invest Dermatol. doi: 10.1038/jid.2012.14. 2012 (accepted for publication). [Personal communication, Richard L Gallo, MD; January 5, 2012] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 91. James WD, Berger TG, Elston DM, Skin: basic structure and function. In: James WD, Berger TG, Elston DM. eds. Andrews’ Diseases of the Skin Clinical Dermatology, 10th Edition. Phildelphia: Saunder Elsevier; 2006:12. [Google Scholar]
- 92.Rowell LB. Reflex control of the cutaneous vasculature. J Invest Dermatol. 1977;69:154–166. doi: 10.1111/1523-1747.ep12497938. [DOI] [PubMed] [Google Scholar]
- 93.Johnson JM, Kellogg DL. Local thermal control of human cutaneous circulation. J Appl Physiol. 2010;109:1229–1238. doi: 10.1152/japplphysiol.00407.2010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 94.Piascik MT, Perez DM. Alpha1-adrenergic receptors: new insights and directions. J Pharmacol Exp Ther. 2001;298:403–410. [PubMed] [Google Scholar]
- 95.Civantos Calzada B, Aleixandre de Artinano A. Alpha-adrenoreceptor subtypes. Pharmacol Res. 2001;44:195–208. doi: 10.1006/phrs.2001.0857. [DOI] [PubMed] [Google Scholar]
- 96.Guimaraes S, Moura D. Vascular adrenoreceptors: an update. Pharmacol Rev. 2001;53:319–356. [PubMed] [Google Scholar]
- 97.Leech CJ, Faber JE. Different alpha-adrenoreceptor subtypes mediate constriction of arterioles and venules. Am J Physiol. 1996;270(2, pt 2):H710–H722. doi: 10.1152/ajpheart.1996.270.2.H710. [DOI] [PubMed] [Google Scholar]
- 98.Hieble JP. Subclassification and nomenclature of alpha- and beta-adrenoreceptors. Curr Top Med Chem. 2007;7:129–134. doi: 10.2174/156802607779318172. [DOI] [PubMed] [Google Scholar]
- 99.Kim MB, Kim GW, Park HJ, et al. Pimecrolimus 1% cream for the treatment of rosacea. J Dermatol. 2011;38:1135–1139. doi: 10.1111/j.1346-8138.2011.01223.x. [DOI] [PubMed] [Google Scholar]
- 100.Weissenbacher S, Merkl J, Hildebrandt B, et al. Pimecrolimus cream 1% for papulopustular rosacea: a randomized vehicle-controlled double-blind trial. Br J Dermatol. 2007;156:728–32. doi: 10.1111/j.1365-2133.2006.07669.x. [DOI] [PubMed] [Google Scholar]
- 101.Koca R, Altinyazar HC, Ankarali H, et al. A comparison of metronidazole 1% cream and pimecrolimus 1% cream in the treatment of patients with papulopustular rosacea: a randomized open-label clinical trial. Clin Exp Dermatol. 2010;35:251–256. doi: 10.1111/j.1365-2230.2009.03427.x. [DOI] [PubMed] [Google Scholar]
- 102.Garg G, Thami GP. Clinical efficacy of tacrolimus in rosacea. J Eur Acad Dermatol Venereol. 2009;23:239–240. doi: 10.1111/j.1468-3083.2008.02822.x. [DOI] [PubMed] [Google Scholar]
- 103.Ertl GA, Levine N, Kligman AM. A comparison of the efficacy of topical tretinoin and low-dose oral isotretinoin in rosacea. Arch Dermatol. 1994;130:319–324. [PubMed] [Google Scholar]
- 104.Park H, Del Rosso JQ. Use of oral isotretinoin in the management of rosacea. J Clin Aesthet Dermatol. 2011;4:54–61. [PMC free article] [PubMed] [Google Scholar]
- 105.Rebora A. The management of rosacea. Am J Clin Dermatol. 2002;3:489–496. doi: 10.2165/00128071-200203070-00005. [DOI] [PubMed] [Google Scholar]
- 106.Buechner SA. Rosacea: an update. Dermatology. 2005;210:100–08. doi: 10.1159/000082564. [DOI] [PubMed] [Google Scholar]
- 107.Gupta AK, Chaudhry MM. Rosacea and its management: an overview. J Eur Acad Dermatol Venereol. 2005;19:273–85. doi: 10.1111/j.1468-3083.2005.01216.x. [DOI] [PubMed] [Google Scholar]
- 108.Ramey JT, Bailen E, Lockey RF. Rhinitis medicamentosa. J Investig Allerg Clin Immunol. 2006;16:148–155. [PubMed] [Google Scholar]
- 109.Graf P. Long term use of oxy- and xylometazoline nasal sprays induces rebound swelling, tolerance, and nasal hyper-reactivity. Rhinology. 1996;34:9–13. [PubMed] [Google Scholar]
- 110.California: Allergan Inc.; 2011. Alphagan-P Opthalmic Solution 0.1% and 0.15% [package insert]. Irvine. [Google Scholar]
- 111.Fowler J, Jarratt M, Moore A, et al. Once-daily topical brimonidine tartrate gel 0.5% is a novel treatment of moderate to severe facial erythema of rosacea: results of two multicenter, randomized and vehicle-controlled studies. [2011 Nov 2];Br J Dermatol. doi: 10.1111/j.1365-2133.2011.10716.x. doi: 10.1111/j.1365-2133.2011. 10716.x. [Epub ahead of print] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 112.Rahman MQ, Ramaesh K, Montgomery DNI. Brimonidine for glaucoma. Expert Opin Drug Saf. 2010;9:483–491. doi: 10.1517/14740331003709736. [DOI] [PubMed] [Google Scholar]
- 113.Mark K, Sparacio RM, Voigt A, et al. Objective and quantitative improvement of rosacea-associated erythema after intense pulsed light treatment. Dermatol Surg. 2003;29:600–604. doi: 10.1046/j.1524-4725.2003.29141.x. [DOI] [PubMed] [Google Scholar]
- 114.Papageorgiou P, Clayton W, Norwood S, et al. Treatment of rosacea with intense pulsed light: significant treatment and long-lasting results. Br J Dermatol. 2008;159:628–632. doi: 10.1111/j.1365-2133.2008.08702.x. [DOI] [PubMed] [Google Scholar]
- 115.Neuhaus IM, Zane LT, Tope WD, et al. Comparative efficacy of nonpurpuragenic pulsed dye laser and intense pulsed light for erythematotelangiectatic rosacea. Dermatol Surg. 2009;35:920–928. doi: 10.1111/j.1524-4725.2009.01156.x. [DOI] [PubMed] [Google Scholar]
- 116.Clark SM, Lanigan SW, Marks R. Laser treatment of erythema and telangiectasia associated with rosacea. Lasers Med Sci. 2002;17:26–33. doi: 10.1007/s10103-002-8263-8. [DOI] [PubMed] [Google Scholar]
- 117.Tan SR, Tope WD. Pulsed dye laser treatment of rosacea improves erythema, symptomatology, and quality of life. J Am Acad Dermatol. 2004;51:592–99. doi: 10.1016/j.jaad.2004.04.010. [DOI] [PubMed] [Google Scholar]
- 118.Menezes N, Moreira A, Mota G, et al. Quality of life of rosacea: pulsed dye laser impact. J Cosmet Laser Ther. 2009;11:139–41. doi: 10.1080/14764170902741311. [DOI] [PubMed] [Google Scholar]
- 119.Berg M, Edstrom DW. Flashlamp pulsed dye laser (FPDL) did not cure papulopustular rosacea. Lasers in Surg Med. 2004;34:266–268. doi: 10.1002/lsm.10254. [DOI] [PubMed] [Google Scholar]