

Abstract
Objective. To assess the magnitude of regional difference in prevalence of short stature in Saudi children and adolescents. Subjects and Methods. A representative sample from three different regions of the Kingdom of Saudi Arabia (KSA) (North, Southwest, and Center) was used to calculate the prevalence of short stature (standard deviation score less than −2) in children 5 to 17 years of age. Results. There were 9018 children and adolescents from 5 to 17 years of age (3366, 2825, and 2827 in the Northern, Southwestern and Central regions, resp.) and 51% were boys. In both school-age children and adolescents, there was a significantly higher prevalence of short stature in the Southwestern than in the Northern or the Central region (P < 0.0001). Conclusion. The finding of significant regional variation between regions helps in planning priorities for research and preventive measures.
1. Introduction
Short stature which is the result of poor linear growth is a common referral of children and adolescents to specialized clinics for investigations. Short stature may be part of well-known syndromes, systemic and endocrine diseases, or an early presentation of treatable conditions such as isolated growth hormone deficiency and celiac disease and inflammatory bowel disease [1–4]. However, the more common isolated, idiopathic short stature in “normal” children is thought to be related more to environmental factors such as chronic under nutrition [5]. Knowledge of the prevalence of short stature is the first step for prevention of this condition and its complications. Although national prevalence data are important, significant regional variations in the prevalence of nutritional disorders such as malnutrition in preschool children have been reported which resulted in recommendations for priorities for further research and preventive programs for regions with high prevalence of malnutrition [6]. These findings suggest that regional variation in prevalence of other nutritional disorders such as short stature may also exist in school-age children and adolescents. Therefore, the objective of this report is to assess the regional variations in prevalence of short stature in the Kingdom of Saudi Arabia.
2. Methods
The prevalence of short stature in Saudi school-age children and adolescents (5–17 years of age) was calculated from the data set of the national Saudi reference. The design and methodology of the survey used to establish the latter reference have been reported in details elsewhere [7]. In brief, a multistage probability procedure was used to randomly select a cross-sectional sample from a stratified listing of the population of the KSA that was available at the time of study design. Therefore, the sample was representative of all the socioeconomic strata including weighted urban rural representation in each region. House-to-house visits were made to all selected houses where a survey questionnaire, clinical examination, and body measurements were completed by primary care physicians and nurses. Stature measurements were performed on all healthy children and adolescents by trained physicians and nurses according to recommended standards [8]. A representative sample from three different regions of the KSA (North, Southwest, and Center) was used to calculate the prevalence of short stature for age for children 5 to 17 years. The 2000 Center for Disease Control and Prevention (CDC) growth reference and related software were used for the calculation of prevalence data [9]. The prevalence of short stature was defined by the proportion of children with height for age below minus 2 standard deviations (<−2 SD). Prevalence data were calculated for three regions from the North (Hail, Jouf, and Northern Borders), two Southwestern regions (Gizan and Aseer), and two Central regions of the kingdom (Riyadh and Qassim). In this study, the combinations of regions were based on population characteristics. Accordingly, the Northern region, represented by Hail, Al Jouf, and the Northern Borders, has a majority of stable tribal population, the Southwestern region represented by Aseer and Gizan also has a majority of stable tribal population different from the North, and the Central region, represented by Riyadh and Qassim, consists of a multiethnic population. Although the population in each combination, such as Riyadh and Qassim, may be considered similar, the Northern, Southwestern, and Central regions are different from each other representing the geographic and ethnic spectrum of the country. Chi-square test was used to assess the difference in prevalence between genders and regions and a P value of <0.05 was considered.
3. Results
The total sample size was 9018 children and adolescents from 5 to 17 years of age (51% boys). The regional distribution of the children was 3366, 2825, and 2827 in the Northern, Southwestern, and Central regions, respectively. The prevalence of moderate short stature in school-age children is presented in Table 1 indicating a significantly higher prevalence in the Southwestern than in the Northern or the Central region (P < 0.0001). The prevalence was not statistically different between the Northern and Central region (P = 0.214). There was no significant difference in prevalence of short stature between adolescent boys and girls in the Northern (P = 0.949), the Southwestern (P = 0.670), or the Central region (P = 0.307). The prevalence data for adolescents are depicted in Table 2 showing a significantly higher prevalence in the Southwestern than in the Northern or the Central region (P < 0.0001). There was no significant difference between the Northern and Central region (P = 0.229). There was no significant difference in prevalence of short stature between boys and girls in the Northern (P = 0.328), the Southwestern (P = 0.731), or the Central region (P = 0.223). In all age groups, there is generally increasing prevalence of short stature with age in both genders and in all regions. These regional variations are summarized in Figure 1.
Table 1.
Regional prevalence of short stature in school-age children.
| Age (years) | North: No (% <2 SD*) | Southwest: No (% <2 SD) | Central: No (% <2 SD) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Boys | Girls | All | Boys | Girls | All | Boys | Girls | All | |
| 5–<6 | 152 (8.6) | 124 (4.8) | 276 (6.7) | 110 (3.6) | 117 (15.4) | 227 (9.5) | 146 (4.8) | 111 (3.6) | 257 (4.2) |
| 6–<7 | 131 (6.1) | 140 (3.6) | 271 (4.9) | 112 (11.6) | 93 (4.3) | 205 (8) | 104 (5.8) | 129 (3.1) | 233 (4.5) |
| 7–<8 | 149 (6) | 141 (8.5) | 290 (7.3) | 111 (13.5) | 113 (16.8) | 224 (15.2) | 124 (6.5) | 120 (3.3) | 244 (4.9) |
| 8–<9 | 150 (3.3) | 133 (6.8) | 283 (5.1) | 118 (16.9) | 94 (14.9) | 212 (15.9) | 129 (15.5) | 118 (5.1) | 247 (10.3) |
| 9–<10 | 136 (4.4) | 145 (5.5) | 281 (5) | 124 (9.7) | 108 (12) | 232 (10.9) | 131 (6.9) | 109 (6.4) | 240 (6.7) |
| 10–<11 | 152 (6.6) | 134 (4.5) | 286 (5.6) | 101 (7.9) | 118 (12.7) | 219 (10.3) | 114 (5.3) | 131 (6.1) | 245 (5.7) |
| 11–<12 | 145 (5.5) | 130 (9.2) | 275 (7.4) | 113 (14.2) | 98 (4.1) | 211 (9.2) | 112 (8.9) | 116 (6) | 228 (7.5) |
| 12–<13 | 123 (12.2) | 126 (8.7) | 249 (10.5) | 106 (12.3) | 116 (13.8) | 222 (13.1) | 117 (9.4) | 102 (5.9) | 219 (7.7) |
|
| |||||||||
| Overall | 1138 (6.5) | 1073 (6.4) | 2211 (6.5) | 895 (11.3) | 857 (12) | 1752 (11.6) | 977 (6) | 936 (4.9) | 1913 (5.5) |
*Standard deviation.
Table 2.
Regional prevalence of short stature in adolescents.
| Age (years) | North: No (% <2 SD*) | Southwest: No (% <2 SD) | Central: No (% <2 SD) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Boys | Girls | All | Boys | Girls | All | Boys | Girls | All | |
| 13–<14 | 110 (9) | 116 (13.8) | 226 (11.4) | 117 (12.8) | 126 (16.7) | 243 (14.8) | 106 (8.5) | 97 (21.6) | 203 (15.1) |
| 14–<15 | 153 (10.5) | 127 (14.2) | 280 (12.4) | 125 (20) | 109 (18.3) | 234 (19.2) | 86 (7) | 112 (15.2) | 198 (11.1) |
| 15–<16 | 115 (14.8) | 107 (8.4) | 222 (11.6) | 95 (12.6) | 102 (19.6) | 197 (16.1) | 97 (15.5) | 85 (16.5) | 18 (16) |
| 16–<17 | 115 (10.4) | 104 (16.3) | 219 (13.4) | 115 (21.7) | 103 (25.2) | 218 (23.5) | 93 (20.4) | 78 (11.5) | 171 (16) |
| 17–<18 | 98 (11.2) | 110 (13.6) | 208 (12.4) | 88 (25) | 93 (17.2) | 181 (21.1) | 68 (13.2) | 72 (15.3) | 140 (14.3) |
|
| |||||||||
| Overall | 591 (11.2) | 564 (13.3) | 1155 (12.2) | 540 (18.3) | 533 (19.3) | 1073 (18.8) | 450 (12.9) | 444 (16.2) | 894 (14.5) |
*Standard deviation.
Figure 1.
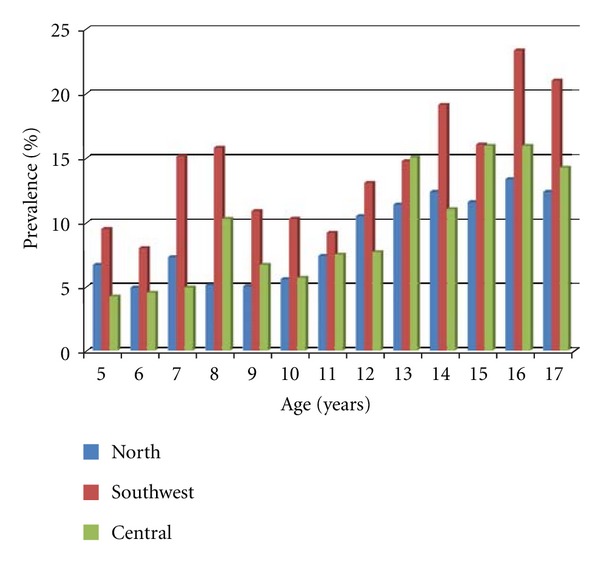
Regional variation in prevalence of short stature according to age.
4. Discussion
The identification of regional differences of nutritional disorders such as short stature in older children and adolescents is important for targeting high-prevalence areas for programs to prevent short stature and its complications such as psychologic disorders and obesity and its complications [10–14]. In this report, there was a significantly higher prevalence of short stature in the Southwestern regions compared to the Northern or Central region which is significant and contrasts with the national prevalence of 11% [15]. Such regional variations have been reported from other countries. In a report from the West Bank, Palestine, the prevalence of stunting in school children aged 13–15 years was 9.2% and 7.3% in boys and girls, respectively, in Ramallah and 9.4% to 4.2% in boys and girls, respectively, in Hebron [16].
In addition to genetic causes, the high altitude, the predominance of rural areas exceeding 60%, and the high prevalence of malnutrition are some of the environmental factors that have been documented in the Southwestern regions and may account at least in part for the high prevalence of short stature [6, 17]. However, further research is needed for identification of the causes and subsequently development of preventive programs.
Among other environmental factors, parental education and socioeconomic status are widely recognized contributing factors to short stature. In a previous report, we have shown that the prevalence of malnutrition was highest among children with limited parental education [18]. In Brazil narrowing socioeconomic inequalities led to reduction of prevalence of short stature [19]. In addition, in a report on stunting in Indian adolescents aged 11–16 living in South India compared with a sample from the same ethnic background but living in Dubai, United Arab Emirates (UAE), a prevalence of stunting 38.8% and 36.9% in boys and girls, respectively, who are living in India, compared to 8.9% and 11.6% for South Indian students living in the UAE [20] was revealed. These reports not only indicate the role of environmental factors but more importantly that improvement in these factors led to reduction of prevalence of short stature and its complications.
In conclusion, this report demonstrates the importance of regional variations in prevalence of short stature in planning priorities for research and prevention.
Acknowledgment
This study was funded by King Abdulaziz City for Science and Technology, Riyadh, Kingdom of Saudi Arabia (Grant no. AR-20-63).
References
- 1.Wit JM, Clayton PE, Rogol AD, Savage MO, Saenger PH, Cohen P. Idiopathic short stature: definition, epidemiology, and diagnostic evaluation. Growth Hormone and IGF Research. 2008;18(2):89–110. doi: 10.1016/j.ghir.2007.11.004. [DOI] [PubMed] [Google Scholar]
- 2.Edouard T, Grünenwald S, Gennero I, Salles JP, Trauber M. Prevalence of IGF1 deficiency in prepubertal children with isolated short stature. European Journal of Endocrinology. 2009;161(1):43–50. doi: 10.1530/EJE-08-0964. [DOI] [PubMed] [Google Scholar]
- 3.Hashemi J, Hajiani E, Shahbazin HBB, Masjedizadeh R, Ghasemi N. Prevalence of celiac disease in Iranian children with idiopathic short stature. World Journal of Gastroenterology. 2008;14(48):7376–7380. doi: 10.3748/wjg.14.7376. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Kanof ME, Lake AM, Bayless TM. Decreased height velocity in children and adolescents before the diagnosis of Crohn’s disease. Gastroenterology. 1988;95(6):1523–1527. doi: 10.1016/s0016-5085(88)80072-6. [DOI] [PubMed] [Google Scholar]
- 5.Frongillo EA, Jr., Hanson KMP. Determinants of variability among nations in child growth. Annals of Human Biology. 1995;22(5):395–411. doi: 10.1080/03014469500004082. [DOI] [PubMed] [Google Scholar]
- 6.El-Mouzan MI, Al-Herbish AS, Al-Salloum AA, et al. Regional disparity in prevalence of malnutrition in Saudi children. Saudi Medical Journal. 2010;31(5):550–554. [PubMed] [Google Scholar]
- 7.El-Mouzan MI, Al-Herbish AS, Al-Salloum AA, Qurachi MM, Al-Omar AA. Growth charts for Saudi children and adolescents. Saudi Medical Journal. 2007;28(10):1555–1568. [PubMed] [Google Scholar]
- 8.Waterlow JC, Buzina R, Keller W. The presentation and use of height and weight data for comparing the nutritional status of groups of children under the age of 10 years. Bulletin of the World Health Organization. 1977;55(4):489–498. [PMC free article] [PubMed] [Google Scholar]
- 9.Center for Disease Control and Prevention. http://www.cdc.gov/growthcharts/
- 10.Frongillo EA, Jr., De Onis M, Hanson KMP. Socioeconomic and demographic factors are associated with worldwide patterns of stunting and wasting of children. Journal of Nutrition. 1997;127(12):2302–2309. doi: 10.1093/jn/127.12.2302. [DOI] [PubMed] [Google Scholar]
- 11.Voss LD. Short normal stature and psychosocial disadvantage: a critical review of the evidence. Journal of Pediatric Endocrinology and Metabolism. 2001;14(6):701–711. doi: 10.1515/jpem.2001.14.6.701. [DOI] [PubMed] [Google Scholar]
- 12.Ulph F, Betts P, Mulligan J, Stratford RJ. Personality functioning: the influence of stature. Archives of Disease in Childhood. 2004;89(1):17–21. doi: 10.1136/adc.2002.010694. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Hoffman DJ, Sawaya AL, Verreschi I, Tucker KL, Roberts SB. Why are nutritionally stunted children at increased risk of obesity? Studies of metabolic rate and fat oxidation in shantytown children from Sao Paulo, Brazil. American Journal of Clinical Nutrition. 2000;72(3):702–707. doi: 10.1093/ajcn/72.3.702. [DOI] [PubMed] [Google Scholar]
- 14.Kruger HS, Pretorius R, Schutte AE. Stunting, adiposity, and low-grade inflammation in African adolescents from a township high school. Nutrition. 2010;26(1):90–99. doi: 10.1016/j.nut.2009.10.004. [DOI] [PubMed] [Google Scholar]
- 15.El Mouzan MI, Al Herbish AS, Al Salloum AA, Foster PJ, Al Omer AA, Qurachi MM. Prevalence of short stature in Saudi children and adolescents. Annals of Saudi Medicine. 2011;31(5):498–501. doi: 10.4103/0256-4947.84628. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Mikki N, Abdul-Rahim HF, Faisal Awartani F, Holmboe-Ottesen G. Prevalence and sociodemographic correlates of stunting, underweight, and overweight among Palestinian school adolescents (13–15 years) in two major governorates in the West Bank. http://www.biomedcentral.com/1471-2458/9/485. [DOI] [PMC free article] [PubMed]
- 17.El Mouzan MI, Al Salloum AA, Al Herbish AS, Qurachi MM, Al Omer AA. Tech. Rep. AR-20-63. Riyadh, Saudi Arabia: King Abdulaziz City for Science and Technology; 2010. Health profile for Saudi children and adolescents. [Google Scholar]
- 18.El-Mouzan MI, Al-Salloum AA, Al-Herbish AS, Qurachi MM, Al-Omar AA. Effects of education of the head of the household on the prevalence of malnutrition in children. Saudi Medical Journal. 2010;31(3):304–307. [PubMed] [Google Scholar]
- 19.Monteiro CA, Benicio MHD, Conde WL, et al. Narrowing socioeconomic inequality in child stunting: the Brazilian experience, 1974–2007. Bulletin of the World Health Organization. 2010;88(4):305–311. doi: 10.2471/BLT.09.069195. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Haboubi GJ, Shaikh RB. A comparison of the nutritional status of adolescents from selected schools of South India and UAE: a cross-sectional study. Indian Journal of Community Medicine. 2009;34(2):108–111. doi: 10.4103/0970-0218.51230. [DOI] [PMC free article] [PubMed] [Google Scholar]