

Abstract
Objective
Nitric oxide (NO) deficiency may contribute to microvascular dysfunction in sepsis. Current physiologic paradigms contend that nitrite and/ or S-nitrosohemoglobin (SNOHb) mediate intravascular delivery of NO. These NO metabolites are purportedly consumed during hemoglobin deoxygenation producing NO and coupling intravascular NO delivery with metabolic demand. Systemic nitrite and SNOHb consumption can be assessed by comparing their concentrations in arterial vs. venous blood. We hypothesized that arterial vs. venous (A-V) differences in nitrite and SNOHb are diminished in sepsis and associated with mortality.
Design
Case-control and prospective cohort study
Setting
Adult intensive care units of an academic medical center
Patients and subjects
87 critically ill septic patients and 52 control subjects
Interventions
None
Measurements and Main Results
Nitrite and SNOHb were measured using tri-iodide-based reductive chemiluminescence. In control subjects, arterial plasma, whole blood and red blood cell nitrite levels were higher than the corresponding venous levels. In contrast, SNOHb was higher in venous compared to arterial blood. In septic patients, A-V RBC nitrite and SNOHb differences were absent. Moreover, the plasma nitrite A-V difference was absent in non-survivors.
Conclusions
In health, nitrite levels are higher in arterial vs. venous blood (suggesting systemic nitrite consumption) whereas SNOHb levels are higher in venous vs. arterial blood (suggesting systemic SNOHb production). These A-V differences are diminished in sepsis, and diminished A-V plasma nitrite differences are associated with mortality. These data suggest pathologic disruption of systemic nitrite utilization in sepsis.
Keywords: septic shock, nitric oxide, nitrites, critical care, intensive care, erythrocytes
INTRODUCTION
The purported roles of nitric oxide (NO) in sepsis are contradictory: excessive production causing hypotension (1), and reduced production impairing microvascular blood flow (2). Excessive NO production in human sepsis is suggested by elevated concentrations of plasma nitrate plus nitrite (NOx) (3-6). However, recent metabolic isotope studies indicate reduced NO production in septic patients (7, 8). Moreover, inhibiting NO production increases the risk of mortality in septic patients (9).
Nitric oxide appears to have endocrine activity, with physiologic effects occurring distant from the NO source (10). This presumably occurs by formation of circulating NO metabolites that are consumed as hemoglobin deoxygenates, releasing NO bioactivity and matching blood flow with metabolic need. S-nitrosohemoglobin (SNOHb) (11) and nitrite (12) are postulated mediators of this effect. In vivo, this paradigm is supported by studies showing higher arterial vs. venous concentrations of nitrite and SNOHb (10-14), suggesting consumption of the metabolite (and coincident NO release) in the systemic vasculature. This is analogous to measuring the A-V oxygen content difference, with larger differences suggesting higher systemic oxygen consumption. Although there is general agreement that such intravascular NO delivery occurs, controversy surrounds the identity of responsible metabolite(s) (15).
Reports of nitrite and SNOHb concentrations in septic humans are limited (16-18). There are no reports of paired arterial and venous measurements in sepsis. We hypothesized that systemic consumption of these NO metabolites is impaired in sepsis and associated with mortality. To test this hypothesis, we measured arterial and venous levels of NO metabolites in patients with severe sepsis or septic shock and a control group without acute illness. We reasoned that arteriovenous (A-V) NO metabolite differences should be present in healthy subjects, but not in sepsis patients, despite similar age and gender distributions. We further reasoned that A-V differences should be disrupted to a greater extent in sepsis non-survivors compared to survivors.
MATERIALS AND METHODS
Study design
Consecutive patients meeting diagnostic criteria for severe sepsis or septic shock in the medical or surgical intensive care unit (ICU) of the University of Rochester Medical Center (19) were eligible. Control subjects without acute illness were recruited by age and gender strata approximating the sepsis cohort. Exclusion criteria are listed in Table 1. The primary outcome measures were presence of sepsis and hospital mortality. Written informed consent was obtained from subjects or surrogate decision-makers. This study was approved by the University of Rochester Research Subjects Review Board.
Table 1.
Exclusion criteria
| Code status limitations precluding critical care management (e.g. directives against use of mechanical ventilation or vasopressor agents). |
| Refusal of patient or designated surrogate decision-maker to provide written informed consent, or inability to obtain consent within 48 hours of diagnosis |
| Severe cardiomyopathy with left-ventricular ejection fraction < 30%a |
| Chronic dialysis-dependent renal failurea |
| History of solid organ or bone marrow/ stem cell transplantationa |
| Pre-existing advanced liver disease (Child-Pugh Grade C)a |
| Organic nitrate therapya |
| Current active bleedinga |
| Hematocrit < 22% or <25% while on vasopressorsa |
| Pregnancy or hormone replacement therapy (HRT)a |
| >48 hours since severe sepsis/ septic shock diagnosis |
| Arterial catheter for blood sampling not available |
| Laboratory equipment or staff not available |
Exclusion criteria for both control subjects and sepsis patients. Control subjects were also excluded if they had infections or used antibiotics within 6 weeks of specimen collection.
Measurement of NO Metabolites
Arterial and venous blood samples were obtained within 48 hours of severe sepsis/ septic shock diagnosis, or during an outpatient visit to the Clinical Research Center in control subjects. Nitric oxide metabolites were measured using tri-iodide (I3−) - based reductive chemiluminescence (20-22) (see description of methods in Supplemental Digital Content 1). The assays yielded measurements of plasma, red blood cell (RBC) and whole blood (WB) nitrite, plasma nitrate, SNOHb, RBC XNO (RBC XNO signifies primarily iron-nitrosyl hemoglobin [FeNOHb], but may also include RBC nitrosamines (23, 24)), and the combination of plasma nitrosothiols, metal nitrosyl compounds and nitrosamines.
Statistical Analysis
Nitric oxide metabolite distributions were right-skewed. Normal distributions were approximated by square root transformations of plasma nitrate and log (base 10) transformations of the other NO metabolites. The data were transformed accordingly prior to statistical analysis. Paired t-tests were used to compare arterial and venous NO metabolite concentrations. Unpaired t-tests with unequal variance were used to compare metabolites between cases and controls, and between survivors and non-survivors. Chi-square testing was used for comparison of categorical variables. Two-way analysis of variance (ANOVA) was used to assess differences in NO metabolite concentrations between groups while controlling for potential confounding variables (see statistical methods in Supplemental Digital Content 1). Results are summarized as means with 95% confidence interval (C.I.) after back-transformation to the original scale unless otherwise specified. A p value of ≤ 0.05 was accepted as statistically significant. Statistical analyses were performed using Stata/ SE version 9.2 (Stata Corp., College Station, TX).
RESULTS
Research Subjects
From February 2006 – July 2008, 597 ICU patients were screened and 87 met enrollment criteria (Figure 1). Samples were collected 27 ± 12 (mean ± standard deviation [S.D.]) hours after diagnosis of severe sepsis or septic shock. Fifty-two non-septic control subjects were recruited. Subject characteristics are shown in Table 2. Technical problems precluded measurement of WB nitrite in 3 sepsis patients and SNOHb in 4 subjects (1 control subject, 3 sepsis patients).
Figure 1.
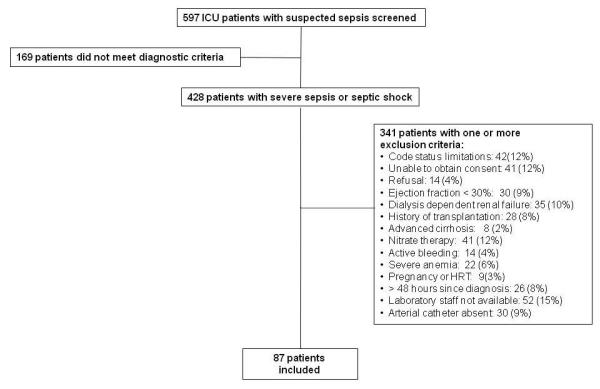
Enrollment flow-diagram for sepsis patients
Table 2.
Baseline characteristics of study subjects a
| Controls (n=52) |
Sepsis (n=87) |
pb | Survivors (n=59) |
Non-survivors (n=28) |
pc | |
|---|---|---|---|---|---|---|
| Aged | 59 ± 12 | 59 ± 18 | 0.86 | 55 ± 17 | 69 ± 16 | 0.0005 |
| Male sex | 26 (50%) | 48 (55%) | 0.55 | 32 (54%) | 16 (57%) | 0.80 |
| Non-Caucasian race | 3 (6%) | 17 (19%) | 0.04 | 10 (17%) | 6 (21%) | 0.61 |
| Pre-existing Conditions | ||||||
| Hypertension | 11 (21%) | 53 (61%) | <0.001 | 29 (49%) | 24 (86%) | 0.001 |
| Diabetes mellitus | 7 (13%) | 22 (25%) | 0.10 | 14 (24%) | 8 (28%) | 0.62 |
| Smoking | 1 (2%) | 30 (34%) | <0.001 | 22 (37%) | 8 (28%) | 0.42 |
| Hypercholesterolemia | 16 (31%) | 26 (30%) | 0.91 | 18 (30%) | 8 (28%) | 0.85 |
| CAD | 3 (6%) | 13 (15%) | 0.10 | 9 (15%) | 4 (14%) | 0.90 |
| Liver disease | 2 (4%) | 5 (6%) | 0.62 | 2 (3%) | 3 (10%) | 0.17 |
| Creatinine (mg/dL) e | 0.7 (0.6-0.8) | 1.3 (0.9 – 2.1) | <0.001 | 1.1 (0.8 – 1.6) | 1.7 (1.3 – 2.5) | 0.004 |
| Admission category | ||||||
| Medical (vs. surgical) | -- | 79 (92%) | -- | 55/59 (93%) | 25/28 (89%) | 0.50 |
| APACHE II Score d | -- | 26 (± 9) | -- | 24 ± 8 | 31 ± 9 | 0.0001 |
| Organ dysfunction (n) f | 0.07 | |||||
| 1 | -- | 10 (12%) | -- | 9 (15%) | 1 (4%) | -- |
| 2 | -- | 26 (30%) | -- | 21 (36%) | 5 (18%) | -- |
| 3 | -- | 20 (23%) | -- | 11 (19%) | 9 (32%) | -- |
| ≥ 4 | -- | 31 (36%) | -- | 18 (30%) | 13 (46%) | -- |
| Site of Infection | 0.75 | |||||
| Pulmonary | -- | 58 (67%) | -- | 41 (69%) | 17 (61%) | -- |
| Intra-abdominal | -- | 12 (14%) | -- | 8 (14%) | 4 (14%) | -- |
| Skin/ catheter | -- | 2 (2%) | -- | 1 (2%) | 1 (4%) | -- |
| Urinary | -- | 11 (13%) | -- | 7 (12%) | 4 (14%) | -- |
| Bloodstream | -- | 3 (3%) | -- | 1 (2%) | 2 (7%) | -- |
| CNS | -- | 1 (1%) | -- | 1 (2%) | -- | -- |
| Microbiology | 0.20 | |||||
| Gram positive | -- | 29 (33%) | -- | 19 (32%) | 10 (36%) | -- |
| Gram negative | -- | 15 (17%) | -- | 10 (17%) | 5 (18%) | -- |
| Mixed | -- | 17 (20%) | -- | 8 (14%) | 9 (32%) | -- |
| Fungal | -- | 3 (3%) | -- | 3 (5%) | -- | -- |
| Other | -- | 4 (5%) | -- | 3 (5%) | 1 (4%) | -- |
| Unknown | -- | 19 (22%) | -- | 16 (27%) | 3 (11%) | -- |
| Positive blood cultures | -- | 31 (36%) | -- | 20 (34%) | 11 (39%) | 0.62 |
| Septic shock g | -- | 80 (92%) | -- | 52 (88%) | 28 (100%) | 0.06 |
| Vasopressor use | -- | 69 (79%) | -- | 41 (69%) | 28 (100%) | 0.001 |
Values are number of subjects (percentage), unless otherwise specified
p value for comparison of sepsis patients to control subjects
p value for comparison of sepsis survivors to sepsis non-survivors
mean ± standard deviation (SD)
median (inter-quartile range)
organ dysfunctions as defined previously (44) with slight modification, including: cardiovascular (hypotension [systolic blood pressure < 90 mm Hg or mean arterial pressure < 60 mm Hg], vasopressor requirement, or clinical evidence of hypoperfusion); acid-base (metabolic acidosis and plasma lactate concentration > 2 mmol/L); renal (urine output < 0.5 mL/kg/hour despite fluid resuscitation); neurologic (altered mental status without other causes); respiratory (P:F ratio < 250, or < 200 if lungs are only dysfunctional organ); hematologic (platelet count < 80,000 or > 50% decrease from baseline)
shock = hypotension or vasopressor dependence that persisted for ≥ 3 hours despite fluid challenge; CAD = coronary artery disease
Sepsis Patients vs. Control Subjects
In control subjects, arterial nitrite was significantly higher than venous nitrite in plasma, whole blood, and RBCs, suggesting nitrite consumption in the systemic circulation, whereas arterial SNOHb was lower than venous SNOHb, suggesting SNOHb production (Table 3 and Figure 2) (25). The A-V difference in RBC XNO was not statistically significant (Table 3).
Table 3.
NO Metabolites in control subjects and sepsis patients
| NO Metabolitea | Controls (n=52) | Sepsis (n=87) | p valueb |
|---|---|---|---|
| Arterial plasma nitrite | 106 (83 - 134) | 106 (85 - 132) | 0.99 |
| Venous plasma nitrite | 67 (55 - 83) | 66 (54 - 81) | 0.90 |
| p valuec | <0.001 | <0.001 | |
|
| |||
| Arterial WB nitrite | 208 (185 - 235) | 237 (212 - 265) | 0.12 |
| Venous WB nitrite | 139 (122 - 161) | 206 (184 - 232) | <0.001 |
| p valuec | <0.001 | <0.001 | |
|
| |||
| Arterial RBC nitrite | 300 (246 - 365) | 374 (282 - 496) | 0.20 |
| Venous RBC nitrite | 165 (109 - 250) | 355 (250 - 504) | 0.006 |
| p valuec | 0.002 | 0.79 | |
|
| |||
| Arterial SNOHb | 45 (32 - 64) | 56 (42 - 76) | 0.31 |
| Venous SNOHb | 123 (96 - 157) | 80 (59 - 110) | 0.03 |
| p valuec | <0.001 | 0.06 | |
|
| |||
| Arterial RBC XNO | 22 (15 - 32) | 19 (13 - 26) | 0.49 |
| Venous RBC XNO | 28 (18 - 45) | 33 (24 - 44) | 0.71 |
| p valuec | 0.27 | <0.001 | |
|
| |||
| Arterial nitrate | 31 (24 - 38) | 43 (34 - 53) | 0.03 |
| Venous nitrate | 24 (19 - 30) | 43 (34 - 52) | <0.001 |
| p valuec | 0.08 | 1.0 | |
All metabolite concentrations are nM, except nitrate which is μM.
Comparison of concentration in control subjects vs. sepsis patients
Comparison of arterial vs. venous concentration
Figure 2.
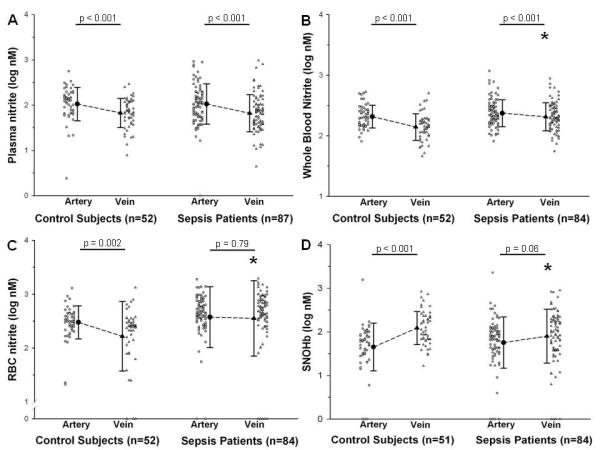
Arterial and venous nitrite and SNOHb concentrations in control subjects vs. sepsis patients. Panel A: plasma nitrite; Panel B: WB nitrite; Panel C: RBC nitrite; Panel D: SNOHb. Concentrations are plotted on the log10 scale. Dot plots show individual data points and corresponding summary plots show mean values with error bars representing standard deviation. Significance values above the bars refer to artery vs. vein comparisons. *p < 0.05 compared to corresponding venous concentration in control subjects.
Comparing sepsis patients to control subjects, there were no differences in arterial or venous plasma nitrite, and the A-V plasma nitrite difference was significant in both groups (Table 3 and Figure 2). In contrast, venous WB and RBC nitrite were significantly higher in septic patients than controls, but arterial WB and RBC nitrite levels were similar. This blunted the WB and RBC nitrite A-V (arterial > venous) nitrite differences in septic patients, suggesting impaired intra-erythrocytic nitrite utilization. Opposite results were observed for venous SNOHb. Compared to controls, sepsis patients had significantly lower venous SNOHb, but arterial levels were similar. This narrowed the A-V (venous > arterial) SNOHb difference in septic patients (Table 3 and Figure 2), suggesting impaired SNOHb production. There were no differences in arterial or venous RBC XNO between controls and sepsis patients. Arterial and venous nitrate were higher in sepsis patients compared to controls (Table 3). The sum concentration of plasma nitrosothiols, metal nitrosyls and nitrosamines was < 12 nM in arterial and venous blood of sepsis and control subjects (data not shown).
Two-way ANOVA showed that renal function confounded the apparent relationship between both arterial and venous nitrate and sepsis (creatinine-adjusted p values for associations between arterial or venous nitrate and sepsis > 0.60, analysis summarized in Table E3 of Supplemental Digital Content 1). In contrast, the association between venous WB nitrite and sepsis persisted after adjustment for possible confounding variables (adjusted p value for association between WB nitrite and sepsis = 0.014).
Multivariate ANOVA indicated that the association between venous SNOHb and sepsis was weakened after controlling for history of hypertension (adjusted p value = 0.194). To ensure that the diminished A-V SNOHb difference in sepsis patients was not confounded by differences in hypertension history between sepsis patients and control subjects, SNOHb A-V differences were examined in sepsis patients and controls stratified by hypertension history. Arterial SNOHb was less than venous SNOHb in controls without hypertension (n=40, arterial = 42 [27-66] vs. venous = 126 [94-168] nM, p < 0.001) and controls with hypertension (n=11, arterial = 56 [35-89] vs. venous = 112 [68-186] nM, p = 0.02). In contrast, arterial and venous plasma nitrite levels were not significantly different in sepsis patients without hypertension (n=32, arterial = 70 [45-110] vs. venous = 104 [71-152] nM, p = 0.09) and sepsis patients with hypertension (n=51, arterial = 49 [33-73] vs. venous = 68[43-107] nM, p = 0.21). This analysis confirms that significant A-V SNOHb differences exist in sepsis patients but not in control subjects, independent of hypertension history.
Hospital Survivors vs. Non-survivors
Twenty-eight patients (32%) with severe sepsis or septic shock died in the hospital (Table 2). The A-V plasma nitrite difference was significant in survivors but not in non-survivors (Figure 3), a consequence of higher venous plasma nitrite in non-survivors (Table 4), suggesting non-survivors have more generalized impairment of nitrite consumption in both plasma and RBC nitrite storage pools. The A-V difference in RBC XNO was significant in survivors but not non-survivors (Table 4).
Figure 3.
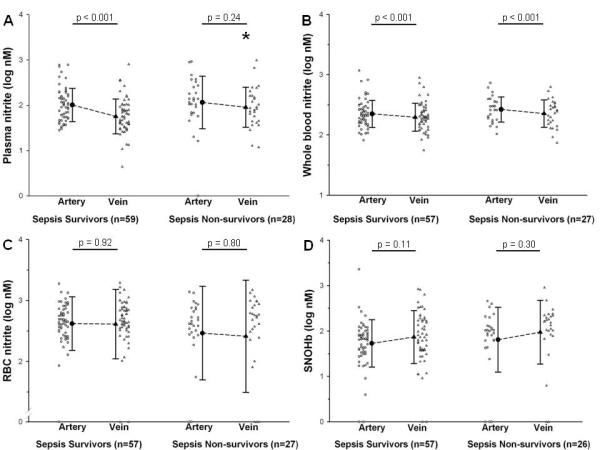
Arterial and venous nitrite and SNOHb concentrations in sepsis survivors vs. non-survivors. Panel A: plasma nitrite; Panel B: WB nitrite; Panel C: RBC nitrite; Panel D: SNOHb. Concentrations are plotted on the log10 scale. Dot plots show individual data points and corresponding summary plots show mean values with error bars representing standard deviation. Significance values above the bars refer to artery vs. vein comparisons. *p < 0.05 compared to corresponding venous concentration in survivors.
Table 4.
NO metabolites in sepsis survivors and non-survivors
| NO Metabolitea | Survivors (n=59b) | Non-survivors (n=28b) | p valuec |
|---|---|---|---|
| Arterial plasma nitrite | 102 (82 - 127) | 116 (69 - 194) | 0.64 |
| Venous plasma nitrite | 57 (45 - 72) | 91 (61 - 134) | 0.04 |
| p valued | <0.0001 | 0.24 | |
|
| |||
| Arterial WB nitrite | 225 (196 - 258) | 265 (219 - 321) | 0.17 |
| Venous WB nitrite | 197 (171 - 227) | 227 (184 - 279) | 0.26 |
| p valued | 0.0002 | <0.0001 | |
|
| |||
| Arterial RBC nitrite | 420 (321 - 549) | 293 (146 - 588) | 0.33 |
| Venous RBC nitrite | 412 (291 - 582) | 260 (112 - 602) | 0.31 |
| p valued | 0.92 | 0.80 | |
|
| |||
| Arterial SNOHb | 54 (39 - 74) | 65 (33 - 124) | 0.60 |
| Venous SNOHb | 74 (52 - 105) | 94 (49 - 181) | 0.50 |
| p valued | 0.11 | 0.30 | |
|
| |||
| Arterial RBC XNO | 16 (11 - 24) | 24 (13 - 44) | 0.30 |
| Venous RBC XNO | 29 (20 - 42) | 38 (23 - 62) | 0.38 |
| p valued | 0.0016 | 0.16 | |
|
| |||
| Arterial nitrate | 42 (32 - 54) | 45 (29 - 64) | 0.79 |
| Venous nitrate | 39 (30 - 49) | 53 (34 -75) | 0.19 |
| p valued | 0.28 | 0.28 | |
All metabolite concentrations are nM, except nitrate which is μM.
Two survivors and 1 non-survivor did not have values for WB and RBC nitrite, 2 survivors and 2 non-survivors did not have values for SNOHb and RBC XNO.
Comparison of concentration in survivors vs. non-survivors
Comparison of arterial vs. venous concentration
Age was a potential confounder of the relationship between higher venous plasma nitrite and hospital mortality (analysis summarized in Table E6 of Supplemental Digital Content 1). To ensure that the diminished A-V plasma nitrite difference in non-survivors was not confounded by differences in age between survivors and non-survivors, plasma nitrite A-V differences were examined in survivors and non-survivors stratified by median age. Arterial plasma nitrite was greater than venous plasma nitrite in the survivors with age ≤ 62 years (n=38, arterial = 89 [70-115] vs. venous = 54 [41-72] nM, p < 0.001) and survivors with age > 62 years (n=21, arterial = 128 [83-198] vs. venous = 62 [41-93] nM, p < 0.001). In contrast, arterial and venous plasma nitrite levels were similar in non-survivors ≤ 62 years (n=8, arterial = 67 [14-321] vs. venous = 54 [22-129] nM, p = 0.63) and non-survivors > 62 years (n=20, arterial = 144 [89-232] vs. venous = 112 [72-174] nM, p = 0.29). This analysis confirms that significant A-V plasma nitrite differences exist in survivors but not in non-survivors, independent of age category.
DISCUSSION
Our results demonstrate that septic patients have elevated venous WB and RBC nitrite concentrations and reduced venous SNOHb concentrations, blunting the A-V nitrite and SNOHb concentration differences observed in non-septic control subjects. In addition, sepsis non-survivors are distinguished from survivors by an isolated rise in venous plasma nitrite that narrows the plasma nitrite A-V difference. These findings have implications for understanding the role of intravascular NO delivery in the pathophysiology of human sepsis.
Sepsis-Associated Disruption of Nitrite-Mediated NO Delivery?
In vitro, nitrite and RBCs together vasodilate vascular tissue preparations, release NO gas, and produce iron-nitrosyl hemoglobin (FeNOHb) in an oxygen-dependent manner that is optimized at the hemoglobin P50 (oxygen tension corresponding to 50% hemoglobin oxygen saturation) (22, 26). This reaction also generates dinitrogen trioxide (N2O3), a potent nitrosating agent that produces nitrosothiols and SNOHb and decomposes to NO and nitrogen dioxide outside the RBC (25).
Our results support this model of NO delivery in humans. In control subjects, we find significant A-V plasma, whole blood, and RBC nitrite concentration differences (arterial > venous), confirming results from previous studies and suggesting systemic nitrite consumption (10, 12, 13). Moreover, we demonstrate significant A-V SNOHb concentration differences (venous > arterial), suggesting production of SNOHb in the systemic circulation. Previous studies of A-V SNOHb differences report conflicting results (14, 22, 27). Our large community-derived control group may have facilitated detection of significant A-V (venous > arterial) SNOHb concentration gradients under basal conditions. These findings underscore the necessity of studying a large healthy control group to establish expected NO metabolite concentrations in those with age and gender distributions similar to the septic cohort.
Venous WB and RBC nitrite levels were higher and venous SNOHb levels were lower in septic patients, narrowing A-V differences observed in control subjects. Additionally, sepsis non-survivors had higher venous plasma nitrite concentration than survivors, without significant A-V difference. These findings suggest impaired nitrite consumption in sepsis that is associated with mortality when involving both plasma and RBC nitrite pools.
The deoxyhemoglobin-mediated nitrite reductase pathway also predicts higher FeNOHb concentrations in vein vs. artery (28), a difference that should be obscured in sepsis patients, particularly non-survivors. The A-V RBC XNO difference (venous > arterial) was statistically significant in sepsis survivors but not in sepsis non-survivors (Table 4), consistent with impaired nitrite reduction according to this model.
We hypothesize that these results reflect dysregulated intra-erythrocytic deoxyhemoglobin-mediated nitrite reduction (Figure 4), a process postulated to occur in an intra-erythrocytic nitrite “metabolon” comprised of the RBC membrane, membrane associated proteins, deoxyhemoglobin, and nitrite (28). We speculate that endotoxin-induced changes in RBC membrane and cytoskeletal proteins (29, 30) may affect the RBC’s ability to facilitate nitrite-mediated NO activity.
Figure 4.
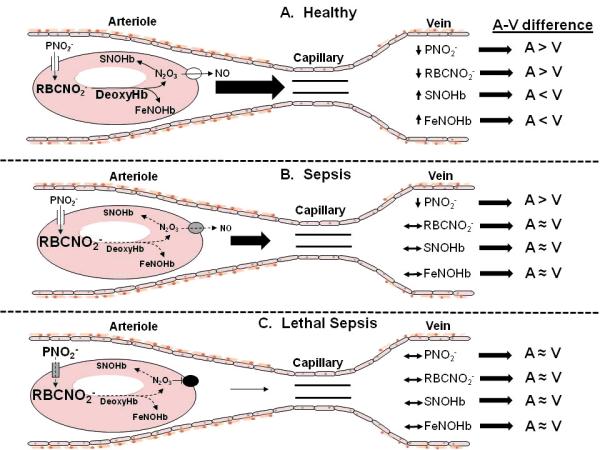
Proposed model for explaining diminished artery-to-vein NO metabolite concentration differences in sepsis. Panel A. Normal physiology. In resistance arterioles, RBCs become partially deoxygenated and the concentration of deoxyHb increases. DeoxyHb catalyzes the reduction of RBC nitrite (RBCNO2−) to form N2O3 and FeNOHb (22, 25). N203 S-nitrosates Hb forming SNOHb, then exits the RBC through a membrane-associated protein complex where it decomposes to NO (and nitrogen dioxide, not shown), augmenting microvascular blood flow (28). Plasma nitrite (PNO2−) enters the RBC to replenish RBCNO2− (42, 43). This metabolic pathway is reflected by NO metabolite concentrations changes in the draining vein. The net result is A-V differences in NO metabolite concentrations, with higher plasma and RBC nitrite (PNO2− and RBCNO2−) in artery vs. vein, but lower SNOHb and FeNOHb in artery vs. vein (10, 12, 13, 22). Panel B. Sepsis. RBC nitrite metabolism is impaired either because of sepsis-associated derangements of the RBC membrane-associated proteins involved in nitrite reduction and NO export (gray color of membrane protein) or lower concentration of deoxyHb (smaller font) (30, 31). The production of SNOHb and FeNOHb decline (dashed arrows and smaller font), and there is diminished RBC NO release (dashed arrows and smaller font), impairing microvascular blood flow (smaller arrow). The defects in membrane-associated proteins and RBCNO2− metabolism are not yet severe enough to affect PNO2− uptake. The net result is diminished A-V differences in all metabolites except PNO2−. Panel C. Lethal sepsis. The membrane-associated protein and metabolic defects are more severe, eliminating NO export (black color of membrane protein complex) and critically reducing blood flow (smaller arrow). The defects are now severe enough to impair PNO2− uptake by the RBC (gray color of membrane channel, larger PNO2− font). The net result is diminished A-V differences for all NO metabolites shown.
Lower availability of deoxyhemoglobin could also impair nitrite biotransformation, since the nitrite reducing capacity of hemoglobin is optimized when the oxygen saturation is approximately 50% (26). Septic shock is characterized by abnormally high mixed venous hemoglobin oxygen saturation (31), which could impair hemoglobin nitrite reductase activity. Sepsis-associated mitochondrial dysfunction or oxidative stress could also disrupt nitrite reductase activity in vascular and extra-vascular tissues (32, 33), independent of RBCs and hemoglobin.
It is possible that higher venous nitrite concentrations and blunted A-V nitrite differences could result from increased systemic nitrite production, rather than impaired nitrite utilization. Ceruloplasmin oxidizes NO to nitrite (34), so elevated systemic NO production and ceruloplasmin could explain the nitrite results (35). However, this mechanism does not explain lower venous SNOHb levels or blunted A-V SNOHb differences. Moreover, increased systemic NO production and oxidation to nitrite would be expected to raise both venous and arterial nitrite concentrations, since the half-life of nitrite in blood is approximately 42 minutes (36). Instead, we found that control subjects, sepsis patients, sepsis survivors and sepsis non-survivors all had similar arterial plasma, WB, and RBC nitrite levels. Impaired nitrite reduction to NO is a more likely explanation for our results, since it accounts for all of these findings.
Another possibility is that elevated nitrate levels cause higher venous nitrite levels. Recent reports indicate that nitrate reductases convert nitrate to nitrite in vivo (37). However, nitrate reduction to nitrite does not explain the absent SNOHb A-V gradient in sepsis, or the similar arterial levels of nitrite in all study groups. Impaired intra-erythrocytic nitrite reduction to NO accounts for all of these findings.
Comparison with Previous Studies
Arterial whole blood nitrite measurements using I3− chemiluminescence were recently reported in 30 ICU patients, including 12 patients with sepsis (17). Consistent with our results, no significant differences in arterial whole blood nitrite between septic and non-septic patients, or between those with and without renal dysfunction, were found.
Two reports describe markedly elevated SNOHb concentrations in six (16) and 12 (18) septic subjects, but artery-to-vein differences were not reported. Discrepancies between the results of Liu, et al. (18) and our SNOHb measurements are likely due to methodological differences (21). The I3− chemiluminescence method used herein has been validated repeatedly (24, 27, 38, 39), and is considered a preferred method for these analyses (40). Differences in sample size, patient characteristics, or the timing of blood sampling relative to sepsis diagnosis may account for discrepancies between our results and those of Doctor, et al (16). Elevated SNOHb concentrations have also been reported in animal models of sepsis (23, 41). However, species variation in NO metabolism makes these findings difficult to apply to humans (24).
Unadjusted arterial and venous nitrate concentrations were higher in sepsis patients compared to control subjects, but these differences were lost after adjustment for renal dysfunction. Villalpando, et al. (7) also found that elevated NOx concentrations in septic patients were tightly correlated with renal function, and further demonstrated that the fractional synthesis rate of NOx is reduced in septic vs. control subjects. Together, these data cast doubt on the commonly held view that human sepsis is characterized by excessive and detrimental NO production (1, 3, 6).
Study Limitations
The limitations of this study included practical constraints on the site and timing of NO metabolite measurements. Venous blood samples were obtained from peripheral veins in control subjects, but usually from central venous catheters in septic patients to minimize discomfort and risk. We are unaware of any published data indicating that venous NO metabolite concentrations differ in peripheral vs. central venous blood. Since venous plasma nitrite concentrations were nearly identical in control subjects (peripheral vein sampling) vs. septic patients (primarily central vein sampling, Figure 2 and Table 3), it is unlikely that there is a systematic difference in the nitrite concentrations of central vs. peripheral blood. Furthermore, venous samples (without matching arterial samples) were obtained in 45 of the sepsis patients just prior to hospital discharge, either peripherally (n=27) or centrally (n=18) depending on available venous access. There were no significant differences between peripherally- and centrally-obtained concentrations of nitrite or SNOHb (see additional results in Supplemental Digital Content 1).
Samples were obtained approximately 27 hours after severe sepsis or septic shock diagnosis. Earlier measurements may have allowed determination of the onset of dysregulated NO metabolism. However, we found no differences in nitrite or SNOHb when analyzed by tertiles of the time interval between sepsis diagnosis and sample collection, suggesting the abnormalities are established early (see Table E7 of Supplemental Digital Content 1).
This study required inclusion of a relatively healthy, non-hospitalized control group to establish baseline NO metabolite values in people of similar age to our sepsis patients. We cannot exclude the possibility that the results observed in our sepsis cohort also apply to other critically ill populations. If so, these results have even greater applicability. This possibility requires further study.
Conclusions
A-V nitrite and SNOHb differences are diminished in patients with severe sepsis and septic shock, and the absence of a significant A-V plasma nitrite difference is associated with mortality. The blunted A-V nitrite and SNOHb differences may signify a detrimental metabolic blockade of nitrite consumption that impairs microvascular blood flow. Further studies are required to determine relationships between nitrite consumption, RBC characteristics, and microvascular blood flow in sepsis. Such information could advance efforts to therapeutically harness NO activity and improve microvascular function in sepsis.
Supplementary Material
ACKNOWLEDGEMENTS
We gratefully acknowledge the trust and generosity of our patients and their families.
Source of support: NIH K23 HL80077 & UL1 RR 024160
Footnotes
LIST OF SUPPLEMENTAL DIGITAL CONTENT • Supplemental Digital Content 1. Contains text and figures describing detailed analytic methods, and tables showing relevant statistical analyses and results. doc
REFERENCES
- 1.Landry D, Oliver JA. The pathogenesis of vasodilatory shock. N Engl J Med. 2001;345:588–595. doi: 10.1056/NEJMra002709. [DOI] [PubMed] [Google Scholar]
- 2.Trzeciak S, Cinel I, Dellinger P, Shapiro NI, Arnold RC, Parrillo JE, Hollenberg SM, on behalf of the Microcirculatory Alterations in Resuscitation and Shock (MARS) Investigators Resuscitating the microcirculation in sepsis: The central role of nitric oxide, emerging concepts for novel therapies, and challenges for clinical trials. Acad Emerg Med. 2008;15:399–413. doi: 10.1111/j.1553-2712.2008.00109.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.MacKanzie I, Garrard CS, Young JD. Indices of nitric oxide synthesis and outcome in critically ill patients. Anaesthesia. 2001;56:326–330. doi: 10.1046/j.1365-2044.2001.01920.x. [DOI] [PubMed] [Google Scholar]
- 4.Gomez-Jimenez J, Salgado A, Mourelle M, Cruz Martin M, Segura RM, Peracaula R, Moncada S. L-arginine: Nitric oxide pathway in endotoxemia and human septic shock. Crit Care Med. 1995;23:253–258. doi: 10.1097/00003246-199502000-00009. [DOI] [PubMed] [Google Scholar]
- 5.Evans T, Carpenter A, Kinderman H, Cohen J. Evidence of increased nitric oxide production in patients with the sepsis syndrome. Circ Shock. 1993;41:77–81. [PubMed] [Google Scholar]
- 6.Groeneveld J, Hartemink KJ, deGroot MCM, Visser J, Thijs LG. Circulating endothelin and nitrate-nitrite relate to hemodynamic and metabolic variables in human septic shock. Shock. 1999;11:160–166. doi: 10.1097/00024382-199903000-00002. [DOI] [PubMed] [Google Scholar]
- 7.Villalpando S, Gopal J, Balasubramanyam A, Bandi VP, Guntupalli K, Jahoor F. In vivo arginine production and intravascular nitric oxide synthesis in hypotensive sepsis. Am J Clin Nutr. 2006;84:197–203. doi: 10.1093/ajcn/84.1.197. [DOI] [PubMed] [Google Scholar]
- 8.Luiking Y, Poeze M, Ramsay G, Deutz NEP. Reduced citrulline production in sepsis is related to diminished de novo arginine and nitric oxide production. Am J Clin Nutr. 2009;89:142–152. doi: 10.3945/ajcn.2007.25765. [DOI] [PubMed] [Google Scholar]
- 9.Lopez A, Lorente JA, Steingrub J, Bakker J, McLuckie A, Willatts S, Brockway M, Anzueto A, Halzapfel L, Breen D, Silverman MS, Takala J, Donaldson J, Ameson C, Grove G, Grossman S, Grover R. Multiple-center, randomized, placebo-controlled, double-blind study of the nitric oxide synthase inhibitor 546c88: Effect on survival in patients with septic shock. Crit Care Med. 2004;32:21–30. doi: 10.1097/01.CCM.0000105581.01815.C6. [DOI] [PubMed] [Google Scholar]
- 10.Cannon R, Schechter AN, Panza JA, Ognibene FP, Pease-Fye ME, Waclawiw MJA, Shelhamer JH, Gladwin MT. Effects of inhaled nitric oxide on regional blood flow are consistent with intravascular nitric oxide delivery. J Clin Invest. 2001;108:279–287. doi: 10.1172/JCI12761. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Jia L, Bonaventura C, Bonaventura J, Stamler JS. S-nitrosohaemoglobin: A dynamic activity of blood involved in vascular control. Nature. 1996;380:221–226. doi: 10.1038/380221a0. [DOI] [PubMed] [Google Scholar]
- 12.Gladwin M, Shelhamer JH, Schechter AN, Pease-Fye ME, Waclawiw MA, Panza JA, Ognibene FP, Cannon RO. Role of circulating nitrite and s-nitrosohemoglobin in the regulation of regional blood flow in humans. Proc Natl Acad Sci U S A. 2000;97:11482–11487. doi: 10.1073/pnas.97.21.11482. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Dejam A, Hunter CJ, Pelletier MM, Hsu LL, Machado RF, Shiva S, Power GG, Kelm M, Gladwin MT, Schechter AN. Erythrocytes are the major intravascular storage sites of nitrite in human blood. Blood. 2005;106:734–739. doi: 10.1182/blood-2005-02-0567. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.McMahon T, Moon RE, Luschinger BP, Carraway MS, Stone AE, Stolp BW, Gow AJ, Pawloski JR, Watke P, Singel DJ, Piantadosi CA, Stamler JS. Nitric oxide in the human respiratory cycle. Nat Med. 2002;8:711–717. doi: 10.1038/nm718. [DOI] [PubMed] [Google Scholar]
- 15.Stamler J. Hemoglobin and nitric oxide (letter) N Engl J Med. 2003;349:402. doi: 10.1056/NEJM200307243490419. [DOI] [PubMed] [Google Scholar]
- 16.Doctor A, Platt R, Sheram ML, Eischeid Anne, McMahon T, Maxey T, Doherty J, Axelrod M, Kline J, Gurka M, Gow A, Gaston B. Hemoglobin conformation couples erythrocyte s-nitrosothiol content to o2 gradients. Proc Natl Acad Sci USA. 2005;102:5709–5714. doi: 10.1073/pnas.0407490102. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Kehmeier E, Kropp M, Kleinbongard P, Lauer T, Balzer J, Merx MW, Heusch G, Kelm M, Lepper W, Rassaf T. Serial measurements of whole blood nitrite in an intensive care setting. Free Radic Biol Med. 2008;44:1945–1950. doi: 10.1016/j.freeradbiomed.2008.02.014. [DOI] [PubMed] [Google Scholar]
- 18.Liu L, Yan Y, Zeng M, Zhang J, Hanes MA, Ahearn G, McMahon TJ, Dickfield T, Marshall HE, Que LG, Stamler JS. Essential role of s-nitrosothiols in vascular homeostasis and endotoxic shock. Cell. 2004;116:617–628. doi: 10.1016/s0092-8674(04)00131-x. [DOI] [PubMed] [Google Scholar]
- 19.Bone R, Balk RA, Cerra FB, Dellinger RP, Fein AM, Knaus WA, Schein RM, Sibbald WJ. Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. Chest. 1992;101:1644–1655. doi: 10.1378/chest.101.6.1644. [DOI] [PubMed] [Google Scholar]
- 20.Yang B, Vivas EX, Reiter CD, Gladwin MT. Methodologies for the sensitive and specific measurement of s-nitrosothils, iron-nitrosyls, and nitrite in biological samples. Free Radical Research. 2003;37:1–10. doi: 10.1080/1071576021000033112. [DOI] [PubMed] [Google Scholar]
- 21.MacArthur P, Shiva S, Gladwin MT. Measurement of nitrite and s-nitrosothiols by reductive chemiluminescence. Journal of Chromatography B. 2007;851:93–105. doi: 10.1016/j.jchromb.2006.12.012. [DOI] [PubMed] [Google Scholar]
- 22.Cosby K, Partovi KS, Crawford JH, Patel RP, Reiter CD, Martyr S, Yang BK, Waclawiw MA, Zalos G, Xu X, Huang KT, Shields W, Kim-Shapiro DB, Schechter AN, Cannon RO, Gladwin MT. Nitrite reduction to nitric oxide by deoxyhemoglobin vasodilates the human circulation. Nat Med. 2003;9:1498–1505. doi: 10.1038/nm954. [DOI] [PubMed] [Google Scholar]
- 23.Crawford J, Chacko BK, Pruitt HM, Piknova B, Hogg N, Patel RP. Transduction of no bioactivity by the red blood cell in sepsis: Novel mechanisms of vasodilation during acute inflammatory disease. Blood. 2004;104:1375–1382. doi: 10.1182/blood-2004-03-0880. [DOI] [PubMed] [Google Scholar]
- 24.Feelisch M, Rassaf T, Mnaimneh S, Singh N, Bryan NS, Jourd’heuil D, Kelm M. Concomitant s-, n-, and heme-nitros(yl)ation in biological tissues and fluids: Implications for the fate of no in vivo. FASEB J. 2002;16:1775–1785. doi: 10.1096/fj.02-0363com. [DOI] [PubMed] [Google Scholar]
- 25.Basu S, Grubina R, Huang J, Conradie J, Huang Z, Jeffers A, Jiang A, He X, Azarov I, Seibert R, Mehta A, Patel R, King SB, Hogg N, Ghosh A, Gladwin MT, Kim-Shapiro DB. Catalytic generation of n2o3 by the concerted nitrite reductase and anhydrase activity of hemoglobin. Nat Chem Biol. 2007;3:785–794. doi: 10.1038/nchembio.2007.46. [DOI] [PubMed] [Google Scholar]
- 26.Crawford J, Isbell ST, Huang Z, Shiva S, Chacko BK, Schechter AN, Darley-Usmar VM, Kerby JD, Lang JD, Kraus D, Ho C, Gladwin MT, Patel RP. Hypoxia, red blood cells, and nitrite regulate no-dependent hypoxic vasodilation. Blood. 2006;107:566–574. doi: 10.1182/blood-2005-07-2668. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Gladwin M, Wang X, Reiter CD, Yang BK, Vivas EX, Bonaventura C, Schechter AN. S-nitrosohemoglobin is unstable in the reductive erythrocyte environment and lacks o2/ no-linked allosteric function. J Biol Chem. 2002;277:27818–27828. doi: 10.1074/jbc.M203236200. [DOI] [PubMed] [Google Scholar]
- 28.Gladwin M, Raat NJH, Shiva S, Dezfulian C, Hogg N, Kim-Shapiro DB, Patel RP. Nitrite as a vascular endocrine nitric oxide reservoir that contributes to hypoxic signaling, cytoprotection, and vasodilation. Am J Physiol Heart Circ Physiol. 2006;291:H2026–H2035. doi: 10.1152/ajpheart.00407.2006. [DOI] [PubMed] [Google Scholar]
- 29.Baskurt O, Gelmont D, Meiselman HJ. Red blood cell deformability in sepsis. Am J Respir Crit Care Med. 1998;157 doi: 10.1164/ajrccm.157.2.9611103. [DOI] [PubMed] [Google Scholar]
- 30.Bellary S, Anderson KW, Arden WA, Butterfield DA. Effect of lipopolysaccharide on the physical conformation of the erythrocyte cytoskeletal proteins. Life Sciences. 1995;56:91–98. doi: 10.1016/0024-3205(94)00418-r. [DOI] [PubMed] [Google Scholar]
- 31.Siegel J, Greenspan M, Del Guercio LRM. Abnormal vascular tone, defective oxygen transport and myocardial failure in human septic shock. Ann Surg. 1967;165:504–517. doi: 10.1097/00000658-196704000-00002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Alzawahra W, Talukder MAH, Liu X, Samouilov A, Zweier JL. Heme proteins mediate the conversion of nitrite to nitric oxide in the vascular wall. Am J Physiol (Heart Circ Physiol) 2008;295:H499–H508. doi: 10.1152/ajpheart.00374.2008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Feelisch M, Fernandez BO, Bryan NS, Garcia-Saura MF, Bauer S, Whitlock DR, Ford PC, Janero DR, Rodriguez J, Ashrafian H. Tissue processing of nitrite in hypoxia: An intricate interplay of nitric oxide-generating and -scavenging systems. J Biol Chem. 2008;283:33927–33934. doi: 10.1074/jbc.M806654200. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Shiva S, Wang X, Ringwood LA, Xu X, Yuditskaya S, Annavajjhala V, Miyajima H, Hogg N, Harris ZL, Gladwin MT. Ceruloplasmin is a no oxidase and nitrite synthase that determines endocrine no homeostasis. Nat Chem Biol. 2006;2:486–493. doi: 10.1038/nchembio813. [DOI] [PubMed] [Google Scholar]
- 35.Chiarla C, Giovannini I, Siegel JH. Patterns of correlation of plasma ceruloplasmin in sepsis. J Surg Res. 2008;144:107–110. doi: 10.1016/j.jss.2007.03.024. [DOI] [PubMed] [Google Scholar]
- 36.Dejam A, Hunter CJ, Tremonti C, Pluta RM, Hon YY, Grimes G, Partovi K, Pelletier MM, Oldfield EH, Cannon RO, Schechter AN, Gladwin MT. Nitrite infusions in humans and nonhuman primates: Endocrine effects, pharmacokinetics, and tolerance formation. Circulation. 2007;116:1821–1831. doi: 10.1161/CIRCULATIONAHA.107.712133. [DOI] [PubMed] [Google Scholar]
- 37.Lundberg J, Weitzberg E, Gladwin MT. The nitrate-nitrite-nitric oxide pathway in physiology and therapeutics. Nature Reviews. 2008;7:156–167. doi: 10.1038/nrd2466. [DOI] [PubMed] [Google Scholar]
- 38.Wang X, Bryan NS, MacArthur PH, Rodriguez J, Gladwin MT, Feelisch M. Measurement of no levels in the red cell: Validation of tri-iodide based chemiluminescence with acid-sulfanilamide pre-treatment. J Biol Chem. 2006;281:26994–27002. doi: 10.1074/jbc.M603953200. [DOI] [PubMed] [Google Scholar]
- 39.Basu S, Wang X, Gladwin MT, Kim-Shapiro DB. Chemiluminescent detection of s-nitrosated proteins: Comparison of tri-iodide, copper/co/cysteine and modified copper/cysteine methods. Methods Enzymol. 2008;440:138–156. doi: 10.1016/S0076-6879(07)00808-7. [DOI] [PubMed] [Google Scholar]
- 40.Rassaf T, Feelisch M, Kelm M. Circulating no pool: Assessment of nitrite and nitrosoproteins in blood and tissue. Free Radic Biol Med. 2004;36:413–422. doi: 10.1016/j.freeradbiomed.2003.11.011. [DOI] [PubMed] [Google Scholar]
- 41.Jourd’heuil D, Gray L, Grisham MB. S-nitrosothiol formation in blood of lipopolysaccharide-treated rats. Biochem Biophys Res Commun. 2000;273:22–26. doi: 10.1006/bbrc.2000.2892. [DOI] [PubMed] [Google Scholar]
- 42.Jensen F. Nitrite transport into pig erythrocytes and its potential biological role. Acta Physiol Scand. 2005;184:243–251. doi: 10.1111/j.1365-201X.2005.01448.x. [DOI] [PubMed] [Google Scholar]
- 43.May J, Qu ZC, Xia L, Cobb CE. Nitrite uptake and metabolism and oxidant stress in human erythrocytes. Am J Physiol (Cell Physiol) 2000;279:C1946–C1954. doi: 10.1152/ajpcell.2000.279.6.C1946. [DOI] [PubMed] [Google Scholar]
- 44.Bernard G, Vincent JL, Laterre PF, LaRosa SP, Dhainaut JF, Lopez-Rodriguez A, Steinbrub JS, Garber GE, Helterbrand JD, Ely W, Fisher CJ, PROWESS Study Group Efficacy and safety of recombinant human activated protein c for severe sepsis. N Engl J Med. 2001;344:699–709. doi: 10.1056/NEJM200103083441001. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.