

SUMMARY
Although benign vascular lesions are frequent in the head and the neck region, clinical evidence of cavernous haemangioma of the external auditory canal is extremely rare; when present, the lesion invades the middle ear space. Herein, a rare case of a soft mass filling the external auditory canal, not involving the tympanic membrane, in a symptomatic 59-year-old male is described. Clinical and audiological characteristics, imaging studies and surgical treatment with histological evaluation are reported, which led to a diagnosis of a cavernous haemangioma. This is only the seventh case described in the literature, to date, not involving the tympanic membrane and the middle ear space. In addition, a review has been made of the relevant literature with respect to epidemiology, presentation, evaluation, pathology, and management options for haemangiomas arising in the external auditory canal.
KEY WORDS: External auditory canal, Vascular lesion, Vascular malformation, Cavernous haemangioma
RIASSUNTO
Le lesioni vascolari benigne sono dei quadri patologici di frequente riscontro nel distretto testa-collo, ma l'evidenza clinica di un emangioma cavernoso limitato al meato acustico esterno è estremamente raro; di solito, infatti, la lesione coinvolge, invadendolo, l'orecchio medio. Gli autori riportano un raro caso di una massa di tessuto a densità della parti molli che occlude il condotto uditivo esterno senza interessamento della membrana timpanica, in un uomo di 59 anni sintomatico, descrivendone le caratteristiche cliniche, audiologiche, radiologiche, e strategia chirurgica 'en bloc' con diagnosi finale di emangioma cavernoso. Questo rappresenta il settimo caso descritto in letteratura senza coinvolgimento della membrana timpanica e dell'orecchio medio. Infine, viene riportata una revisione della letteratura con riferimento alla epidemiologia, presentazione, valutazione clinica e patologica, e possibili opzioni chirurgiche nel trattamento degli emangiomi del condotto uditivo esterno.
Introduction
Haemangiomas are soft tissue tumours, common in children and young adults, belonging to vascular anomalies; more that 60% of these occur in the head and neck region 1. According to Mulliken and Glowacki (1982) haemangiomas are commonly classified as either capillary or cavernous haemangiomas 2. The former consist of closely arranged capillary-like channels, and may typically occur in the skin, subcutaneous tissues, lips, liver, spleen, or kidneys while cavernous haemangiomas are composed of large cavernous vascular spaces and often appear in the skin, mucosal surfaces, and internal organs 1 2.
These tumours, that rarely occur after the sixth decade of life, usually grow intermittently throughout the first year of life and then go through a quiescent period and eventual spontaneous involution, by 5 or 6 years of age 2 3.
Cavernous haemangioma of the external auditory canal (EAC) is a rare entity, and, when present, usually involves the tympanic membrane (TM); so far, only 6 cases have been reported in the literature describing a lesion limited to the EAC.
Although some authors have found elevated serum levels of angiogenic peptide basic fibroblast growth factor (bFGF) revealing possibly a genetic role in the first years of life, the mechanism of occurrence of haemangiomas of the EAC in adult patients remains obscure 4.
Herein, a case is reported of a soft mass filling the EAC, not involving the TM, in a symptomatic adult male that after histopathological evaluation was found to be the 7th case of cavernous haemangioma reported in the literature.
Case report
A 59-year-old male came to our Department with a oneyear history of mono-lateral hearing loss, pulsative tinnitus, intermittent aural pressure associated with episodic otalgia and bleeding from the right external auditory canal. He denied having had vertigo or auricular trauma and had no evidence of facial palsy. His family, medical and otologic history was unremarkable; in particular, until onset of symptoms he had never had hearing muffling or Eustachian tube dysfunction. Upon physical examination, right otoscopy revealed a mass totally filling the EAC, with well-defined margins. The lesion was soft, compressible and non-pulsative with pressure; the base could not be visualized but it was possible to compress the mass and to observe the antero-inferior portion of the TM that appeared normal. The mass did not extend beyond the meatus into the concha and the auricle was normal. Otoscopic examination of the left TM was normal. The findings upon physical examination of the head and neck were not significant; in particular, there was no lymphadenopathy and flexible fiberoptic nasopharyngoscopy and vestibular examination were normal.
Weber test at 512 Hz was to the right side, and bone conduction was greater than air conduction in the same ear. A pure tone audiogram showed right mild mixed hearing loss with an average air-bone gap of 35 dB (pure conductive type at 250-2000 Hz, with a sensorineural hearing loss component at 4000 and 8000 Hz). The discrimination score was 96% at 85 dB in the affected ear. High resolution computed tomography (HRCT) of the temporal bone, without contrast agents, showed a 1.8 cm soft-tissue mass lateral to the tympanic membrane that filled the right external auditory canal without involvement of the epitympanum and adjacent bony wall (Fig. 1). There was no evidence of bone erosion, and the tympanic membrane, the middle ear and the ossicles appeared normal (Fig. 2a-b).
Fig. 1.
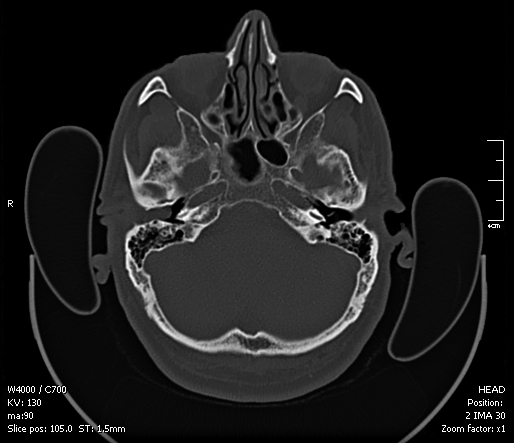
Axial computed tomography, without contrast media, showing a mass lateral to the tympanic membrane filling the right external auditory canal.
Fig. 2.

Coronal computed tomography showing: (a) lesion limited to external auditory canal without involvement of the epi-tympanum and adjacent bony wall; (b) no evidence of bone erosion; tympanic membrane, middle ear and the ossicles appear normal.
Under general anaesthesia, this lesion was smoothly excised, under an otomicroscope, by an endo-aural approach. The mass, based on the postero-inferior portion of the bony canal, was excised en bloc by elevating the skin in continuity with the lesion from the canal without entering the middle ear space; the bone of the EAC was normal in appearance. Bleeding was controlled with cautery.
The histological diagnosis was characteristic of cavernous haemangioma revealing numerous thick-walled blood vessels lined by endothelial cells and containing red blood cells (Fig. 3). The post-operative course was uneventful and the audiogram showed recovery of the conductive component of the hearing loss. Further clinical examinations, until now, show no evidence of the original mass.
Fig. 3.

Pathologic examination revealed numerous thick-walled blood vessels lined by endothelial cells and containing red blood cells. The appearance is characteristic of cavernous haemangioma (haematoxylin and eosin, original magnification × 400).
Discussion
Benign vascular lesions are tumours that frequently involve the head and the neck region. In 1982, Mulliken and Glowacki developed a system of classification that divided these, on the basis of their histological and natural history characteristics, into 2 categories: haemangiomas and vascular malformations 2. Haemangiomas, correctly defined as "capillary haemangiomas", are made up of closed arranged capillary- like channels secondary to a proliferative endothelial process that more frequently occurs in infancy and progressively disappears before the age of 5-6 years 1-4.
In contrast, "cavernous haemangiomas" are made up of large cavernous vascular spaces and more frequently appear after the sixth decade of life; being vascular malformations, their clinical presentation, anatomical changes and progression are strongly correlated to infection, trauma, ligation, attempted excision or changes in serum hormone levels 1-5.
These entities usually occur in the head and neck region, but evidence of a cavernous haemangioma of the EAC, with or without involvement of the TM, are extremely rare. So far, only 19 cases have been described in the literature, and, only in 7 cases, the patients presented a lesion limited to the EAC (Table I) 6-22.
Table I.
Cavernous haemangiomas limited to external auditory canal described in the literature.
| Authors | Year | Age (yr)/Sex | Symptoms | Side | Base implant | Management |
|---|---|---|---|---|---|---|
| Hawke & van Nostrand | 1987 | 55/M | Blood-tinged otorrhoea | Left | Antero-inferior canal wall | Trans-canal excision |
| Limb et al. | 2002 | 67/F | Tinnitus, hearing loss, fullness | Left | Postero-superior canal wall | Endaural excision |
| Reeck et al. | 2002 | 53/M | Tinnitus, hearing loss | Left | Postero-inferior canal wall | Endaural excision |
| Yang et al. | 2006 | 72/F | - | Left | Roof | Trans-canal excision |
| Covelli et al. | 2008 | 45/F | - | Right | - | Endaural excision |
| Rutherford et al. | 2010 | 62/F | Bleeding, aural pressure | Left | Antero-inferior canal wall | 1. Post-auricular excision 2. Trans-cranal excision |
| Martines et al. | 2011 | 59/M | Bleeding, aural pressure, tinnitus, hearing loss | Right | Posterior-inferior canal wall | Endaural Excision |
The first of these cases was described, in 1987, by Hawke and van Nostrand, who reported a 55-year-old male patient in whom a cavernous haemangioma arose from the left antero-inferior canal wall 10. The patient presented blood-tinged otorrhoea and no hearing loss. The lesion was easily removed and bleeding controlled with cautery. Limb et al., in 2002, presented the case of a cavernous haemangioma situated in the postero-superior left ear canal adjacent to the anulus occluding the entire external auditory canal with TM intact, in a 67-year-old female with a history of mixed hearing loss, tinnitus and aural fullness 13. The mass was removed by endaural surgical resection. In the same year, Reeck et al. reported a new case of cavernous haemangioma isolated in the posteroinferior portion of the left EAC in a 53-year-old man with conductive hearing loss and tinnitus, excised by the endoaural approach 14. In 2006, Yang et al. described a lesion occupying the left EAC without involvement of the MT in an asymptomatic 72-year-old female. In this case, excision was through a trans-cranial approach 16. Covelli et al., in 2007, described a small lesion in a 45-year-old female submitted to surgical treatment by endaural excision 20; finally, Rutherford et al., in 2009, reported a new clinical case, in a 62-year-old female, situated in the antero-inferior external auditory canal that, after end-aural excision recurred involving the temporal bone and temporo-mandibular joint (TMJ). It was completely excised by a transcanal approach and TMJ arthrotomy 21.
As stated above, cavernous haemangiomas of the external auditory canal clinically occur in asymptomatic or symptomatic patients with an average age of 59 ± 2.8 years. These lesions appear to affect both sexes, but occur more often in females than in males. As in this case, when present, symptoms are blood-tinged otorrhoea, aural fullness, hearing loss and pulsatile tinnitus. Otoscopic examination reveals the presence of a small sessile or pedunculated, purple mass, based either in the anterior or, as in this patient, in the posterior segments of the EAC, not involving the MT. Diagnostic tests include a pure tone audiometry, HRCT of the temporal bone and\or magnetic resonance imaging (MRI), which are essential to delineate the extent of the tumour, the possible presence of osseous erosions and to perform differential diagnosis, better clarified by a histopathological evaluation that must exclude a malignant lesion (carcinoma) and/or other possible entities such as: glomus tumour, attic chole-steatoma with aural polyp, arterio-venous malformation, granulation tissue. Angiography may be useful to identify and embolize any feeding vessels supplying advanced lesion with excessive bleeding expected. To date, the treatment of choice is complete surgical excision with an end-aural or trans-canal approach, even if watchful waiting is recommended for small asymptomatic lesions 10 13 14 16 20 21 23. The postoperative course is usually uneventful. Recurrence was described in only one of the 7 cases reported, which was probably due to the fact that the implant was based close to the TMJ, and involved the temporal bone, thus requiring a more extensive approach 21.
Conclusions
In summary, the case described here, in accordance with the literature, confirms that external auditory canal haemangiomas, in an adult age, are rare benign lesions and it is necessary to take them into consideration in the differential diagnosis of external auditory canal masses. The diagnostic approach therefore requires the use of physical audiologic and HRCT evaluation, always associated with a histo-pathological study by, when possible, 'en bloc' excision of the lesion that reduces the possibility of recurrence.
References
- 1.McClay JE, Zapalac JS. Skin tumors, vascular lesions, face and neck. emedicine. 2006 http://www.emedicine.com/ent/topic28.htm. [Google Scholar]
- 2.Mulliken JB, Glowacki J. Hemangiomas and vascular malformations in infants and children: a classification based on endothelial characteristics. Plast Reconstr Surg. 1982;69:412–422. doi: 10.1097/00006534-198203000-00002. [DOI] [PubMed] [Google Scholar]
- 3.Yeo A, Majithia A, Kalan A. Haemangioma or vascular malformation of the tympanic membrane? a case report and review of literature. Indian J Otolaryngol Head Neck Surg. 2008;60:59–61. doi: 10.1007/s12070-008-0019-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.McGill TJI, Forsen JWJ, Mulliken JB, et al. Cummings CW. Otolaryngology Head and Neck Surgery. St. Louis: Mosby; 1998. Hemangiomas and vascular anomalies of the head and neck; pp. 66–80. [Google Scholar]
- 5.Martines F, Immordino V. Arteriovenous malformation of the base of tongue in pregnancy: case report. Acta Otorhinolaryngol Ital. 2009;29:274–278. [PMC free article] [PubMed] [Google Scholar]
- 6.Freedman SI, Barton S, Goodhill V. Cavernous angiomas of the tympanic membrane. Arch Otolaryngol. 1972;96:158–160. doi: 10.1001/archotol.1972.00770090232013. [DOI] [PubMed] [Google Scholar]
- 7.Balkany TJ, Meyers AD, Wong ML. Capillary hemangioma of the tympanic membrane. Arch Otolaryngol. 1978;104:296–307. doi: 10.1001/archotol.1978.00790050062015. [DOI] [PubMed] [Google Scholar]
- 8.Andrade JM, Gehris CW, Breitenecker R, et al. Cavernous hemangioma of the tympanic membrane: a case report. Am J Otol. 1983;4:198–199. [PubMed] [Google Scholar]
- 9.Kemink JL, Graham MD, McClatchey KD. Hemangioma of the external auditory canal. Am J Otol. 1983;5:125–126. [PubMed] [Google Scholar]
- 10.Hawke M, Nostrand P. Cavernous hemangioma of the external ear canal. J Otolaryngol. 1987;16:40–42. [PubMed] [Google Scholar]
- 11.Jackson CG, Levine SC, McKennan KX, et al. Recurrent hemangioma of the external auditory canal. Am J Otol. 1990;11:117–118. [PubMed] [Google Scholar]
- 12.Bijelic L, Wei JL, McDonald TJ. Hemangioma of the tympanic membrane. Otolaryngol Head Neck Surg. 2001;125:272–273. doi: 10.1067/mhn.2001.116018. [DOI] [PubMed] [Google Scholar]
- 13.Limb CJ, Mabrie DC, Carey JP, et al. Hemangioma of the external auditory canal. Otolaryngol Head Neck Surg. 2002;126:74–75. doi: 10.1067/mhn.2002.120697. [DOI] [PubMed] [Google Scholar]
- 14.Reeck JB, Yen TL, Szmit A, et al. Cavernous hemangioma of the external ear canal. Laryngoscope. 2002;112:1750–1753. doi: 10.1097/00005537-200210000-00007. [DOI] [PubMed] [Google Scholar]
- 15.Hiraumi J, Miura M, Hirose T. Capillary hemangioma of the tympanic membrane. Am J Otolaryngol. 2005;25:351–352. doi: 10.1016/j.amjoto.2005.02.006. [DOI] [PubMed] [Google Scholar]
- 16.Yang T, Chiang Y, Chao P, et al. Cavernous hemangioma of the bony external auditory canal. Otolaryngol Head Neck Surg. 2006;134:890–891. doi: 10.1016/j.otohns.2005.11.012. [DOI] [PubMed] [Google Scholar]
- 17.Pavamani SP, Surendrababu NRS, Ram TS, et al. Capillary haemangioma involving the middle and external ear: radiotherapy as a treatment method. Australasian Radiol. 2007;51:394–397. doi: 10.1111/j.1440-1673.2007.01733.x. [DOI] [PubMed] [Google Scholar]
- 18.Verret DJ, Cochran S, DeFatta RJ, et al. External auditory canal hemangioma: case report. Skull Base. 2007;17:141–144. doi: 10.1055/s-2006-953512. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Magliulo G, Fusconi M. Capillary hemangioma of the tympanic membrane. Am J Otolaryngol. 2007;28:180–183. doi: 10.1016/S0194-59989770367-X. [DOI] [PubMed] [Google Scholar]
- 20.Covelli E, Seta ED, Zardo F, et al. Cavernous haemangioma of external ear canal. J Laryngol Otol. 2008;122:e19–e19. doi: 10.1017/S0022215108002909. [DOI] [PubMed] [Google Scholar]
- 21.Rutherford KD, Leonard G. Hemangiomas of the external auditory canal. Am J Otolaryngol. 2010;31:384–386. doi: 10.1016/j.amjoto.2009.04.004. [DOI] [PubMed] [Google Scholar]
- 22.Bovo R, Ciorba A, Castiglione A, et al. Cavernous hemangioma of external ear: case report and literature review. BENT. 2010;6:127–130. [PubMed] [Google Scholar]
- 23.Zheng JW, Zhou Q, Yang XJ, et al. Treatment guideline for hemangiomas and vascular malformations of the head and neck. Head Neck. 2010;32:1088–1098. doi: 10.1002/hed.21274. [DOI] [PubMed] [Google Scholar]