

Abstract
Purpose
To investigate the effects of four office chairs on the postural angles of the lumbopelvic and cervical regions.
Research question
Which chair(s) produce an “ideal” spinal posture?
Methods
An experimental same subject design was used involving healthy subjects (n = 14) who conducted a typing task whilst sitting on four different office chairs; two “dynamic” chairs (Vari-Kneeler and Swopper), and two static chairs (Saddle and Standard Office with back removed). Data collection was via digital photogrammetry, measuring pelvic and lumbar angles, neck angle and head tilt which were then analysed within MatLab. A repeated measures ANOVA with Bonferroni corrections for multiple comparisons was conducted.
Results
Statistically significant differences were identified for posterior pelvic tilt and lumbar lordosis between the Vari-Kneeler and Swopper chairs (p = 0.006, p = 0.001) and the Vari-Kneeler and Standard Office chairs (p = 0.000, 0.000); and also for neck angle and head tilt between the Vari-Kneeler and Swopper chairs (p = 0.000, p = 0.000), the Vari-Kneeler and Saddle chairs (p = 0.002, p = 0.001), the Standard Office and Swopper chairs (p = 0.000, p = 0.000), and the Standard Office and Saddle chairs (p = 0.005, p = 0.001). This study confirms a within region association between posterior pelvic tilt and lumbar lordosis, and between neck angle and head tilt. It was noted that an ideal lumbopelvic position does not always result in a corresponding ideal cervical position resulting in a spinal alignment mismatch.
Conclusion
In this study, the most appropriate posture for the lumbopelvic region was produced by the Saddle chair and for the cervical region by both the Saddle and Swopper chairs. No chair consistently produced an ideal posture across all regions, although the Saddle chair created the best posture of those chairs studied. Chair selection should be based on individual need.
Keywords: Office seating, Spinal angles, Posture, Photogrammetry
Introduction
The sedentary modern employment lifestyle encourages greater use of computers and subsequent longer periods of sitting. There is a general consensus in the literature that prolonged sitting by itself is not strongly associated with low back pain except when combined with other risk factors [1]. In addition to the physical factors, the psychosocial aspects of low back pain (LBP) are well established [2] resulting in high profile guidelines on the management of LBP [3–5]. It is unclear if there is a strong association between head posture and neck pain and further research is needed [6]. However, the incidence of work-related musculoskeletal disorders remains high, with the Health and Safety Executive identifying 158,000 new cases in 2010/11 of which approximately 40% affect the low back and 40% affect the neck and upper limbs [7]. The high prevalence of neck and back pain and greater computer use have given rise to a wide variety of office chair types, although there is a paucity of literature comparing the postural consequences of them.
A less than ideal sitting posture results in forward leaning and can give rise to a slumped position in the lumbar spine and/or a forward head posture. The upper cervical extension posture is deemed to be poor for the head and neck [8] and sustained lumbar kyphosis is thought to lead to cumulative spinal soft tissue strain [9]. End range positions generally result in reactive forces in the ligamentous system [10]; this has given rise to the concept of “spinal neutral” defined as a region of intervertebral motion around the neutral posture where little resistance is offered by the passive spinal column [11]. This is considered to be important in minimising spinal tissue strain [12] and could therefore be considered as “ideal” posture.
Generally, office seating design aims to position the user in an ideal posture, and can be classified as dynamic or static. The literature on the adverse effect of poor static postures in office workers seems to have been an additional driver for the increase in the variety of office seating now available, particularly the development of dynamic seating where the seat design allows constant active movement by the user.
Two examples of dynamic seating are the Vari-kneeler (Fig. 1, top left) and the Classic Swopper (Fig. 1, top right). The Vari-kneeler chair positions the user in a semi-kneeling position, the chair’s curved runners, which can be raised using blocks to alter the relative height of the seat pad, allowing a gentle rocking motion. The Swopper chair consists of a round padded seat on a central stem, movement being allowed in three dimensions. Two examples of static chair designs are the Bambach Saddle chair (Fig. 1, bottom right) and a Standard Office chair (Fig. 1, bottom left). The Bambach Saddle chair is designed to position the user in an upright posture whilst sitting astride a convex/concave seat pad.
Fig. 1.

The four chairs used in this study (from top left clockwise): Vari-Kneeler, Swopper, Saddle and Standard Office
Although upper body posture has been investigated in relation to subjects performing dental tasks [13] there is limited research in an office environment; the only research appearing to be that by Gadge and Innes [14] using four subjects. Most Standard Office chairs (Fig. 1, bottom left) provided by employers for computer use appear to be of adjustable height with an adjustable backrest to allow for the maintenance of the recommended posture. Bettany-Saltikov et al. [15] investigated lumbar curvature on a static kneeling chair and a Standard Office chair (n = 20) and found a statistically significant difference between lumbar curvature when comparing the two chairs, users of the kneeling chair demonstrating a lumbar lordosis closer to that of standing.
The aim of this pilot study is to investigate if there is a statistically significant difference (p ≤ 0.05) in pelvic tilt, lumbar angle, neck angle and head tilt when comparing four seating designs (Vari-kneeler, Swopper, Saddle and Standard Office), and consider the postures adopted on the four chairs in relation to an “ideal” posture.
Method
A same subject cross over design was used with randomisation of the order of the four chairs. The chairs selected were considered to be representative of the chairs on the market with recognition being given to both dynamic and static designs. A convenience sample of 14 healthy university student subjects was recruited as a minimum of 12 is considered sufficient per group/condition [16]. It was confirmed that subjects did not have a neurological disease, history of spinal pain or surgery, chronic inflammatory disease effecting any joints, current pregnancy or a BMI >25. Permission for the study had been granted by Cardiff University School of Healthcare Studies Ethics Committee and subjects gave informed consent.
Reflective markers were placed, by the same investigator, on the skin overlying anatomical landmarks: C7, L4, anterior superior iliac spine (ASIS) and posterior superior iliac spine (PSIS), and small sticky backed paper dots were placed on the canthus and tragus (Fig. 2). One of the researchers, who was trained by the chair supplier, gave the subjects individual instructions and a demonstration on the adjuster controls for each chair. The subjects then had 3 min to adjust the chair and work station in order to adopt their self-selected comfortable working position. The Standard Office chair was the only chair to be modified, by removing the backrest to allow observation of the markers during photogrammetry. An adjustable hydraulic desk was set at the usual desk height (71.5 cm) for the Vari-kneeler, Swopper and Standard Office chairs but subjects were able to raise the desk height when they used the Saddle Chair, as recommended by the manufacturer due to the rationale of the design of this chair. The monitor height and keyboard position were adjusted to subject preference. The subjects performed a 5-min typing task involving text displayed on a vertically split screen, using only the keyboard. The duration of the task and the use of a single photograph were chosen for pragmatic reasons whilst still allowing the subjects adequate time to engage with the task. Subjects were blinded to the timing of the photograph, which was taken at 4 min on each chair, so their posture could not be purposefully altered. Only one photograph was taken as there is support for the reliability of photogrammetry [17–19], as well as its validity [17, 19].
Fig. 2.
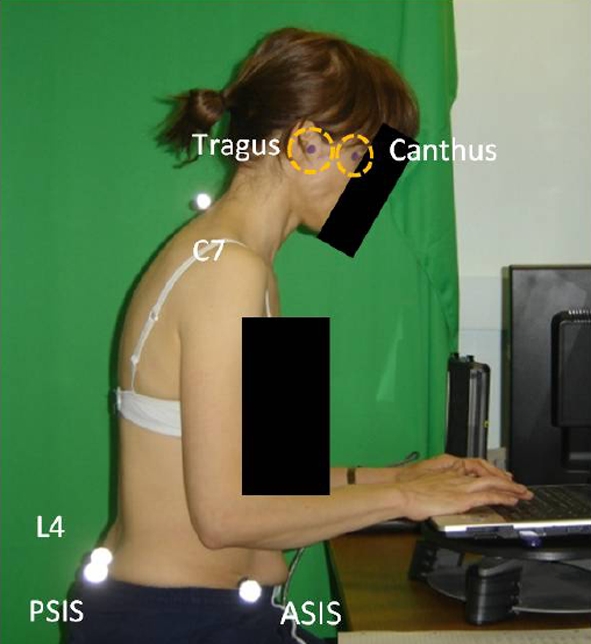
Identification of marker placement on anatomical features: paper markers on canthus and tragus, and reflective markers on C7, L4, PSIS and ASIS
A digital camera was positioned laterally to each subject on a tripod at a standardised distance of 220 cm from the centre of the chair with a standardised zoom to maintain the same perspective and include the markers in the image. Masking tape on the floor determined the position of the centre of the tripod and chair. A contrast drape was used on a screen to enhance the clarification of the markers in the photograph (Fig. 2).
A bespoke MATLAB (The Mathworks Company, Natick, MA, USA) programme was used to calculate spinal angles (Fig. 3a, b): pelvic tilt (a reference line joining the ASIS to PSIS and measured in relation to the horizontal); lumbar angle (calculated using a curved line between T12 and S1, drawn using intersecting circles between L4 and C7); neck angle (the acute angle between a vertical line intersecting C7 and a line from the tragus to C7) measures a forward head position; and head tilt (the angle between the lines from the canthus to tragus, and the tragus to C7) measures the degree of upper cervical extension.
Fig. 3.
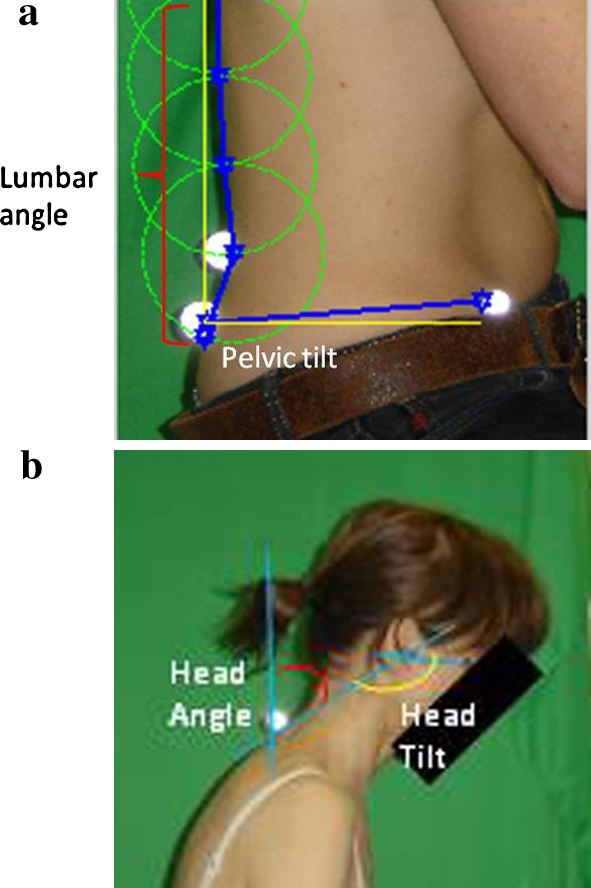
a Diagram illustrating lumbar angle and pelvic tilt. Within the Matlab programme circles were used to identify the spinal curve at fixed distances between L4 and C7 to quantify the lumbar curve (T12 to S1) in degrees. b Diagram illustrating neck angle (the acute angle between a vertical line intersecting C7 and a line from the tragus to C7) and head tilt (the angle between the lines from the canthus to tragus, and the tragus to C7)
The intra-rater reliability of such a MATLAB programme measuring head tilt (0.84) and neck angle (0.91) was determined using intraclass correlation coefficients (ICC) [18], and for the measurement of pelvic obliquity (0.99) and spinal side flexion (0.97) Pearson’s correlation coefficients was used [20]. All results demonstrated very good/excellent reliability.
Data analysis was conducted within Statistical Package for Social Sciences (SPSS) version 16 using a repeated measures ANOVA with a Bonferroni correction for multiple comparisons (p ≤ 0.05).
Results
The sample consisted of 14 subjects, 8 female and 6 male. The subjects were of similar age, within a range of 20–23 (mean 21.1 years).
Figure 4 shows that all chairs resulted in a negative value for the pelvic region indicating a posterior tilt; the Swopper and Standard Office chairs resulted in the greatest posterior tilt and the Vari-kneeler the least. All chairs also resulted in a negative value for the lumbar region indicating a lordotic posture was adopted. Extreme positions were identified with the Vari-kneeler resulting in the greatest lordosis and the Swopper the least. Mid-range values were recorded for the Standard Office chair and the Saddle chair.
Fig. 4.

Spinal angles and standard deviations for pelvic tilt, lumbar angle, neck angle and head tilt for each chair
All chairs resulted in a positive value for neck angle demonstrating the extent of the forward head position. Again extreme positions were recorded, this time with the Vari-kneeler and the Standard Office chairs, resulting in the greatest forward head position whilst the Saddle and Swopper chairs resulted in a less extreme posture. A similar pattern was found with head tilt, which indicated the extent of upper cervical extension.
Figure 4 demonstrates, through using the same scale for all measures (40° range and 5° increments), that the standard deviations for each region are of a similar size. Statistically significant differences were identified for posterior pelvic tilt and lumbar lordosis between the Vari-kneeler and Swopper chairs (p = 0.006, p = 0.001) and the Vari-kneeler and Standard Office chairs (p = 0.000, p = 0.000); and also for neck angle and head tilt between the Vari-Kneeler and Swopper chairs (p = 0.000, p = 0.000), the Vari-kneeler and Saddle chairs (p = 0.002, p = 0.001), the Standard Office and Swopper chairs (p = 0.000, p = 0.000), and the Standard Office and Saddle chairs (p = 0.005, p = 0.001).
Discussion
The study indicated that there were statistically significant differences within pelvic tilt, lumbar lordosis, neck angle and head tilt when comparing four seating designs. There appeared to be a pattern of postures produced for the lumbopelvic and the cervical regions. All sets of data demonstrated comparable standard deviations (Fig. 4) indicating that variability in posture is a natural phenomenon, particularly as subjects were advised to adopt a self-selected position of comfort.
Biomechanically, it would be expected that a large degree of posterior pelvic tilt would give rise to a smaller lordosis, which was indeed the case in this study. The Swopper and Standard Office chairs demonstrated the greatest amount of posterior pelvic tilt and therefore resulted in the least lordosis, the amount of lordosis being negligible in the case of the Swopper chair. The result of the lordosis being greater for the Vari-kneeler, compared with a Standard Office chair, concurs with Bettany-Saltikov et al. [15]. The difference between the Vari-kneeler and Swopper chairs, and Vari-kneeler and Standard Office chairs, was statistically significant for the lumbar lordosis and posterior pelvic tilt, demonstrating the extremes of the ranges measured. If spinal neutral is considered to be an ideal posture, and end range postures undesirable, in our interpretation the Saddle chair could be considered as providing the closest to ideal posture in the lumbopelvic region.
In line with the current understanding of the regional interdependence of spinal alignment, due to the double S-shaped curve of the spine, it was anticipated that the chair that produced the most ideal lumbopelvic posture would also create the most ideal posture in the cervical region. This was apparent in the results for the Saddle chair and the Standard Office chair but discrepancies in the interrelated alignment between the lumbopelvic and the cervical regions were noted in the Vari-kneeler and Swopper chairs in this study. The Vari-kneeler produced a large lumbar lordosis with an unexpectedly large head tilt and neck angle resulting in less than ideal postures for both regions. The Swopper produced a large pelvic tilt and therefore a negligible lumbar lordosis, but a small neck angle and head tilt, suggesting subjects adopted a relatively poor lumbopelvic position but an unexpected comparatively ideal position in the cervical region. The study results challenge the rationale of spinal alignment based on the double S-shaped spinal curve, suggesting that the posture in the cervical region may not be wholly determined by the posture in the lumbopelvic region. This might indicate that individuals’ posture may be determined by other factors, such as knowledge of optimal sitting and anthropometric measurements, and not just by the type of chair.
Postural education often centres around the theoretical premise of the double S spinal curve assuming that a good lumbar posture will create a corresponding correctness within the rest of the spine. Consequently, the results from this study suggest that this is not necessarily the case and concentrating on positioning the lumbopelvic region may have detrimental effects on the other spinal regions. It may therefore be appropriate for advice to address the potential independence of each spinal area.
A pattern of related positions was identified between the neck angle and head tilt which existed in all chairs. This shows that as the neck angle increased, and therefore the forward head posture increased, the amount of head tilt, and therefore upper cervical extension increased in order to keep the head position horizontal. It is postulated that the head tilt increased in response to the increased neck angle in order to maintain the eyes in a horizontal position therefore retaining the ability to look straight ahead at the screen.
The findings of this study suggest that the Saddle chair may be the optimum chair for the lumbopelvic region, and either the Swopper or the Saddle chair for the cervical region. To achieve their optimum posture, the user of this Saddle chair must adopt a hip position of 45° which raises the person above the height of a standard office desk. Therefore to maintain the optimum position, a specialist raised desk was required. It was observed in this study that, although standardised instructions were given for the use of all chairs, the subjects may not have used the dynamic chairs to their full potential. This may have been because subjects were less familiar with the concept of moving while working despite the training, and may have found it challenging to fully synchronise this with the typing task. The modification to the Standard Office chair may have altered the way that this chair was used and suggests that the results for this chair must be considered with some reservation.
These results suggest, therefore, that the selection of a chair must be based on individual need following appropriate assessment, adequate instruction, correct usage and continual evaluation. The data from this pilot study can be used for power calculations for further studies.
Conclusion
This study confirms a within region association between posterior pelvic tilt and lumbar lordosis, and between neck angle and head tilt. It was noted that an ideal lumbopelvic position does not always result in a corresponding ideal cervical position resulting in a spinal alignment mismatch. No chair seemed to consistently produce an ideal posture across all regions and as such chair selection should be based on individual need.
Acknowledgments
Authors thank Back in Action (Bristol) for the loan of the Vari-Kneeler and Swopper and Bambach for loaning the Saddle and adjustable desk.
Conflict of interest
None.
References
- 1.Lis A, Black K, Kom H, Nordin M. Association between sitting and low back pain. Eur Spine J. 2006;16(2):283–298. doi: 10.1007/s00586-006-0143-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Pincus T, Vlaeyen J, Kendall N, Korff M, Kalauokalani D, Reis M. Cognitive-behavioral therapy and psychosocial factors in low back pain: directions for the future. Spine. 2002;27(5):E133–E138. doi: 10.1097/00007632-200203010-00020. [DOI] [PubMed] [Google Scholar]
- 3.Airaksinen O, Brox J, Cedraschi C, Hildebrandt J, Klaber-Moffett J, Kovacs F, Mannion A, Reis S, Staal J, Ursin H, Zanoli G (2004) European Guidelines for the Management of Chronic Non Specific Low Back Pain. http://www.backpaineurope.org/web/files/WG2_Guidelines.pdf. Accessed 25 Jan 2012 [DOI] [PMC free article] [PubMed]
- 4.van Tulder M, Becker A, Bekkering T, Breen A, Teresa Gil del Real M, A, Hutchinson A, Koes B, Laerum E, Malmivaara A (2004) European Guidelines for the Management of Chronic Non Specific Low Back Pain in Primary Care. http://www.backpaineurope.org/web/files/WG1_Guidelines.pdf. Accessed 25 Jan 2012 [DOI] [PMC free article] [PubMed]
- 5.National Institute for Health and Clinical Excellence (2009) Low Back Pain. Early management of persistent non-specific low back pain. http://www.nice.org.uk/nicemedia/live/11887/44343/44343.pdf. Accessed 25 Jan 2012
- 6.Silva A, Punt T, Sharples P, Vilas-Voas J, Johnson M. Head posture assessment for patients with neck pain: is it useful? Int J Ther Rehabil. 2009;16(1):41–53. [Google Scholar]
- 7.Health and Safety Executive (2011) Musculoskeletal disorders. http://www.hse.gov.uk/statistics/causdis/musculoskeletal/msd.pdf. Accessed 25 Jan 2012
- 8.Szeto GPY, Straker L, Raine S. A field comparison of neck and shoulder postures in symptomatic and asymptomatic office workers. Appl Ergonomics. 2002;33:75–84. doi: 10.1016/S0003-6870(01)00043-6. [DOI] [PubMed] [Google Scholar]
- 9.Pynt J, Mackey MG, Higgs J. Kyphosed seated postures: extending concepts of postural health beyond the office. J Occup Rehabil. 2008;18(1):35–45. doi: 10.1007/s10926-008-9123-6. [DOI] [PubMed] [Google Scholar]
- 10.Panjabi M. The stabilizing system of the spine. Part 1: function, dysfunction, application and enhancement. J Spinal Disord. 1992;5(4):383–389. doi: 10.1097/00002517-199212000-00001. [DOI] [PubMed] [Google Scholar]
- 11.Panjabi M. The stabilizing system of the spine. Part II. Neutral Zone and Instability Hypothesis. J Spinal Disord. 1992;5(4):390–396. doi: 10.1097/00002517-199212000-00002. [DOI] [PubMed] [Google Scholar]
- 12.Burnett A, O’Sullivan P, Ankarberg L, Gooding M, Nelis R, Offerman M, Persson J. Lower lumbar spine axial rotation is reduced in end range sagittal postures when compared to a neutral spine posture. Man Ther. 2008;13:300–306. doi: 10.1016/j.math.2007.01.016. [DOI] [PubMed] [Google Scholar]
- 13.Gandavadi A, Ramsay JR, Burke FJ. Assessment of dental student posture in two seating conditions using RULA methodology—a pilot study. Br Dent J. 2006;203(10):601–605. doi: 10.1038/bdj.2007.1047. [DOI] [PubMed] [Google Scholar]
- 14.Gadge K, Innes E. An investigation into the immediate effects on comfort, productivity and posture of the BambachTM saddle seat and a standard office chair. Work. 2006;29(3):189–203. [PubMed] [Google Scholar]
- 15.Bettany-Saltikov J, Warren J, Jobson M. Ergonomically designed kneeling chairs are they worth it?: Comparison of sagittal lumbar curvature in two different seating postures. Stud Health Technol Inform. 2008;140:103–106. [PubMed] [Google Scholar]
- 16.Hicks C. Research methods for clinical therapists: applied project design and analysis. 3. Edinburgh: Churchill Livingstone; 1999. [DOI] [PubMed] [Google Scholar]
- 17.Saad K, Colombo A, Joao S. Reliability and validity of photogrammetry for scoliosis evaluation: a cross sectional prospective study. J Manip Physiol Ther. 2009;32(6):423–429. doi: 10.1016/j.jmpt.2009.06.003. [DOI] [PubMed] [Google Scholar]
- 18.Jones U, Sparkes V, Busse M, Enright S, van Deursen R. (2011) Reliability of digital analysis of thoracic, neck angle and head tilt measurements. J Bone Joint Surg B 93(Suppl IV):490
- 19.vanNiekerk S, Lowe Q, Vaughan C, Grimmer-Somers K, Shreve K. Photographic measurement of upper body posture of high school students: a reliability and validity study. BMC Musculoskelet Disorders. 2008;9:113. doi: 10.1186/1471-2474-9-113. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Sheeran L, Sparkes V (2006) The effect of core stability training on the spinal-pelvic stability during running and on the single leg-hop-for-distance performance test in female runners—preliminary study. http://www.somed.org/symp021206/abstracts.pdf. Accessed 22 Dec 2011