

Sir,
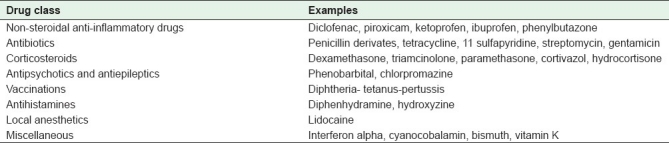
Nicolau syndrome (NS) is a rare cutaneous drug reaction that occurs at the site of an intramuscular drug injection. It was first described in 1924, by Freudenthal, in patients treated with bismuth salts for syphilis. NS has been reported with the administration of various other drugs such as penicillins,[1] local anesthetics, corticosteroids[2] and non-steroidal anti-inflammatory drugs,[3,4] in literature. Table 1 summarizes the causative drugs reported in literature.
Table 1.
Review of causative drugs associated with Nicolau syndrome reported in the literature
Patients with NS experience extremely severe pain around the injection site of the drug immediately after injection, followed by rapid development of erythema, a livedoid reticular patch or a hemorrhagic patch.[3] This skin reaction is pathognomonic. The reaction may result in necrosis and ulceration of the skin, subcutaneous fat, and muscle tissue [Figure 1]. The necrotic ulcer usually heals in several months with an atrophic scar. Various transient neurological complications such as hypoesthesia or paraplegia have been reported in one-third of the patients.[5]
Figure 1.

Large ulcer around the intramuscular injection site of diclofenac on the posteromedial aspect of the right buttock; two weeks after the injection
The pathogenesis of NS is obscure, but in the past it was suggested that it was due to accidental intra-arterial injections.[6] Although several theories have been suggested in literature, the most common hypothesis is direct trauma or irritation of the vascular structures with a compression by the arterial embolism of the drug itself, crystallization of aqueous drugs in the vessels, and arteriovenous shunt development or ischemia following a para-arterial injection. It was reported that cold application for local pain relief caused rapid skin necrosis by increasing the acute local vasospastic effects in a case with NS.[4]
The differential diagnosis of NS includes cutaneous cholesterol embolia, vasculitis, and cutaneous embolization of cardiac myxoma. Cutaneous cholesterol embolia is a disease of the elderly with severe atherosclerotic disease. Skin manifestations in patients with a left atrial myxoma are frequent, usually on acral sites, and accompanied by cardiopulmonary symptoms.[7]
There is no specific therapy for NS. Treatment of NS depends on the extent of the necrosis and ranges from topical to surgical. Conservative treatment with debridement, pain control (analgesics), and dressings is the mainstay of therapy, especially for limited cases. Tissue damage may be reversible in the acute phase of NS. Use of vasoactive agents such as subcutaneous heparin and oral pentoxifylline has been recognized as beneficial.[8] Topical steroids may be worth trying. Surgical intervention is rarely required.
Nicolau syndrome is an avoidable complication. The Z-track injection is a method of intramuscular injection into a large muscle using a needle and syringe and it can minimize or prevent the Nicolau syndrome.[9] Health care personnel should take these precautions:[9,10]
A long (enough to reach muscle) needle should be used. A 90-kg patient requires a 2- or 3-inch (5 – 7.5 cm) needle and a 45-kg patient requires a 1.25- or 1.45-inch needle.
Injection should be applied in the upper outer quadrant of the buttock.
Aspirating the needle before injecting the medication should be performed, to ensure that no blood vessel is hit.
The health care personnel should never inject more than 5 ml of medication at a time when using the Z-track injection method.
If more than one injection or larger dose is required or ordered, different sites should be chosen.
Although NS is an uncommon adverse reaction, clinicians should be aware of this complication and use proper injection procedures.
REFERENCES
- 1.Modzelewska I, Dawidowicz-Szczepanowska A. [Nicolau syndrome following administration of procaine penicillin] Wiad Lek. 1980;33:231–3. [PubMed] [Google Scholar]
- 2.Cherasse A, Kahn MF, Mistrih R, Maillard H, Strauss J, Tavernier C. Nicolau's syndrome after local glucocorticoid injection. Joint Bone Spine. 2003;70:390–2. doi: 10.1016/s1297-319x(03)00137-4. [DOI] [PubMed] [Google Scholar]
- 3.Ezzedine K, Vadoud-Seyedi J, Heenen M. Nicolau syndrome following diclofenac administration. Br J Dermatol. 2004;150:385–7. doi: 10.1111/j.1365-2133.2004.05808.x. [DOI] [PubMed] [Google Scholar]
- 4.Senel E, Ada S, Gulec AT, Caglar B. Nicolau syndrome aggravated by cold application after i.m. diclofenac. J Dermatol. 2008;35:18–20. doi: 10.1111/j.1346-8138.2007.00404.x. [DOI] [PubMed] [Google Scholar]
- 5.Lee DP, Bae GY, Lee MW, Choi JH, Moon KC, Koh JK. Nicolau syndrome caused by piroxicam. Int J Dermatol. 2005;44:1069–70. doi: 10.1111/j.1365-4632.2004.02534.x. [DOI] [PubMed] [Google Scholar]
- 6.Stiehl P, Weissbach G, Schroter K. Nicolau syndrome. Pathogenesis and clinical aspects of penicillin-induced arterial embolism. Schweiz Med Wochenschr. 1971;101:377–85. [PubMed] [Google Scholar]
- 7.Garcia FV, Sanz-Sanchez T, Aragues M, Blasco A, Fraga J, Garcia-Diez A. Cutaneous embolization of cardiac myxoma. Br J Dermatol. 2002;147:379–82. doi: 10.1046/j.1365-2133.2002.04807.x. [DOI] [PubMed] [Google Scholar]
- 8.Ocak S, Ekici B, Cam H, Tastan Y. Nicolau syndrome after intramuscular benzathine penicillin treatment. Pediatr Infect Dis J. 2006;25:749. doi: 10.1097/01.inf.0000226941.85500.9b. [DOI] [PubMed] [Google Scholar]
- 9.Pullen RL., Jr Administering medication by the Z-track method. Nursing. 2005;35:24. doi: 10.1097/00152193-200507000-00018. [DOI] [PubMed] [Google Scholar]
- 10.Lie C, Leung F, Chow SP. Nicolau syndrome following intramuscular diclofenac administration: A case report. J Orthop Surg (Hong Kong) 2006;14:104–7. doi: 10.1177/230949900601400123. [DOI] [PubMed] [Google Scholar]