

Abstract
A case of spontaneous formation of cutaneous fistula from rupture of an infected hydatid cyst of liver in a female child is reported.
KEY WORDS: Fistula, hydatid, rupture
INTRODUCTION
Approximately 70% of hydatid cysts are located in the liver.[1] Hydatid cyst can rupture into any body cavity or any adjacent organ.[2] The physiological channels include the bile duct, the gastrointestinal tract and the bronchus. The free body cavities include the peritoneum and the pleura.[2,3] There are only five case reports of spontaneous fistualization of hydatid cyst into the skin in the literature in adults, but none in children.[4]
CASE REPORT
A 7-year-old female child presented with pain in the right upper quadrant of the abdomen for 1 year and a small opening in the skin just medial to the anterior axillary line in the 8th intercostal space of the right side discharging pus and a white membranous structure. She had no other complaint except intermittent fever.
On physical examination, there was an opening with mildly everted edges accommodating a 10 Fr feeding tube [Figure 1]. A whitish membrane was seen protruding out of the opening. The defect was 5 cm to the right side of the midline and 5 cm above the tip of the 7th costal cartilage. In the past, the patient had undergone exploratory laparotomy for hydatid cyst of liver 2 years back. The routine blood investigations, liver and kidney function tests were normal. The plain abdominal radiograph showed elevated right hemidiaphragm.
Figure 1.

Photograph showing external opening of the fistula
An ultrasonography (USG) of the abdomen revealed hydatid cyst of the liver. The fistula tract was also seen approaching the skin level. A contrast-enhanced computed tomogram showed two hydatid cysts, measuring 4 cm × 5 cm and 2.3 cm × 2.1 cm in diameter [Figure 2]. A fistulogram showed the cutaneous opening communicating with the cyst cavity. Examination of the fluid revealed scolices and pus. Hydatid serology was positive. At surgery, a fistulous communication was identified and a lot of hydatid fluid and membrane were evacuated from the cyst cavity. The fistula tract was closed and excised.
Figure 2.
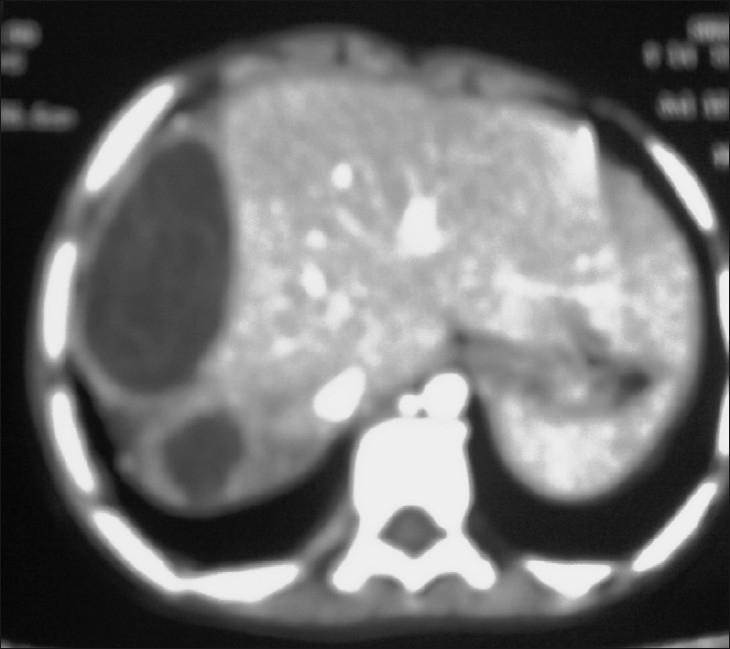
Computed tomogram showing hydatid cyst liver
The cyst was located in segment VIII of the liver just under the diaphragm. Albendazole was administered postoperatively. At 5 months follow-up, the child was doing well. A repeat USG was normal.
DISCUSSION
Spontaneous rupture of the hydatid cyst could be of three types[5–7]: contained, communicating or direct. Direct – when both endo- and ectocysts rupture, causing leak into the pleural or peritoneal cavity or adjacent organs. Communicating rupture – rupture of endocytes with spillage of contents into the small bile ducts incorporated into the pericyst. Although cyst rupture may be clinically asymptomatic, complications like anaphylaxis, obliteration of biliary tree and hydronephrosis due to rupture into the urinary tract can occur.[8–14]
Rupture of hepatic hydatid cyst occurs in 35–58% of the cases, usually into the biliary tract, but the cyst may also rupture into the physiological channels, body cavities or adjacent organs. Rare types of ruptures are fistulization into duodenum, perforation of diaphragm, infiltration of ribs and rupture into the urinary or vascular system. Rupture of hydatid cyst into the liver followed by cystocutaneous fistula is extremely rare. Till now, only six such reports have been published in the literature.[12–14] All the six patients presented in the literature were adults. Two of them are cutaneous – cysto-bronchial fistulas of hydatid disease.[14] Our case is the first in the literature depicting cystocutaneous fistula due to hydatid in a child of 7 years of age. In our patient, the fistula was produced by direct chest wall invasion by a cyst located near the surface of the liver due to increase in the intracystic pressure and, subsequently, due to inflammation and erosion.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Schwartz SI. 7th ed. New York: McGraw-Hill Companies; 1999. Principles of Surgery; pp. 1395–435. [Google Scholar]
- 2.Milicevic MN. Hydatid disease. In: Blumgart LH, Fong Y, editors. Surgery of the liver and biliary tract. 1st ed. London: W.B. Saunders Company Ltd; 2000. pp. 1167–204. [Google Scholar]
- 3.Florea M, Barbu ST, Crisan M, Silaghi H, Butnaru A, Lupsor M. Spontaneous external fistula of a hydatid liver cyst in a diabetic patient. Chirurgia (Bucur) 2008;103:695–8. [PubMed] [Google Scholar]
- 4.Sayek I, Onat D. Diagnosis and treatment of uncomplicated hydatid cyst of the liver. World J Surg. 2001;25:21–7. doi: 10.1007/s002680020004. [DOI] [PubMed] [Google Scholar]
- 5.Koksal N, Muftuoglu T, Gunerhan Y, Uzun MA, Kurt R. Management of intrabiliary ruptured hydatid disease of the liver. Hepatogastroenterol. 2001;48:1094–6. [PubMed] [Google Scholar]
- 6.Sozuer EM, Ok E, Arslan M. The perforation problem in hydatid disease. Am J Trop Med Hyg. 2002;66:575–7. doi: 10.4269/ajtmh.2002.66.575. [DOI] [PubMed] [Google Scholar]
- 7.Grigy-Guillaumot C, Yzet T, Flamant M, Bartoli E, Lagarde V, Brazier F, et al. Cutaneous fistulization of a liver hydatid cyst. Gastroenterol Clin Biol. 2004;28:819–20. doi: 10.1016/s0399-8320(04)95139-1. [DOI] [PubMed] [Google Scholar]
- 8.Schipper HG, Kager PA. Diagnosis and treatment of hepatic echinococcosis: An overview. Scand J Gastroenterol Suppl. 2004;241:50–5. doi: 10.1080/00855920410011004. [DOI] [PubMed] [Google Scholar]
- 9.Bastid C, Pirro N, Sahel J. Cutaneous fistulation of a liver hydatid cyst. Gastroenterol Clin Biol. 2005;29:748–9. doi: 10.1016/s0399-8320(05)88218-1. [DOI] [PubMed] [Google Scholar]
- 10.Sakorafas GH, Stafyla V, Kassaras G. Spontaneous cystcutaneous fistula: An extremely rare presentation of hydatid liver cyst. Am J Surg. 2006;192:205–6. doi: 10.1016/j.amjsurg.2006.02.022. [DOI] [PubMed] [Google Scholar]
- 11.Kehila M, Allegue M, Abdesslem M, Letaief R, Said R, Hadj B, et al. Spontaneous cutaneous-cystic-hepatic-bronchial fistula due to an hydatid cyst. Tunis Med. 1987;65:267–70. [PubMed] [Google Scholar]
- 12.Golematis BC, Karkanias GG, Sakorafas GH, Panoussopoulos D. [Cutaneous fistula of hydatid cyst of the liver] J Chir (Paris) 1991;128:439–4. [PubMed] [Google Scholar]
- 13.Harandou M, el Idrissi F, Alaziz S, Cherkaoui M, Halhal A. [Spontaneous cysto-hepato-bronchial fistula caused by a hydatid cyst.Apropos of a case] J Chir (Paris) 1997;134:31–4. [PubMed] [Google Scholar]
- 14.Paksoy M, Karahasanoglu T, Carkman S, Giray S, Senturk H, Ozcelik F, et al. Rupture of the hydatid disease of the liver into the biliary tracts. Dig Surg. 1998;15:25–9. doi: 10.1159/000018582. [DOI] [PubMed] [Google Scholar]