

Abstract
A 4-year-old girl presented with non-bilious vomiting and loss of appetite and weight. At laparotomy, a non-communicating pyloroduodenal duplication cyst was present. Subtotal excision of the cyst and cauterization of the mucosal lining of the common wall was performed. The post-operative recovery was uneventful.
KEY WORDS: Gastric duplication, gastric outlet obstruction, pyloroduodenal duplication
INTRODUCTION
Duplication cysts in the antral-pyloric region of the stomach are rare and may present as an abdominal mass, gastric outlet obstruction or gastrointestinal hemorrhage. Duodenal duplication cysts generally appear on the first or second portion of the duodenum, and may cause duodenal obstruction, hemorrhage or pancreatitis. Pyloroduodenal duplication cyst is extremely rare and presents as gastric outlet obstruction. Only four cases have been reported in the literature.[1–4] We report a case of non-communicating pyloro-duodenal duplication cyst on the pyloric and first portion of the duodenum. To the best of our knowledge, this is the first documented case of a pyloroduodenal duplication cyst successfully treated by subtotal excision and cauterization of the epithelial lining.
CASE REPORT
A 4-year-old girl was admitted with non-bilious vomiting and loss of appetite and weight for 6 months. The antenatal and family history was unremarkable. She was moderately nourished, weighing 12 kg (expected weight was 16 kg), and there was slight upper abdominal distension with a palpable lump. An ultrasonography (USG) revealed a well-defined cystic lesion measuring 12 cm × 12 cm × 9 cm between the inferior vena cava and the stomach. A contrast-enhanced computed tomography (CECT) scan of the abdomen showed a well-circumscribed, low-attenuation fluid collection seen in relation to the greater curvature of the stomach with rim enhancement, suggestive of an intestinal duplication [Figure 1].
Figure 1.

Contrast-enhanced computed tomography image of the abdomen showing duplication cyst
At laparotomy, the lesser sac was opened and the cyst was seen on the pyloroduodenal region extending onto the first part of the duodenum [Figure 2]. An attempt to develop a plane between the walls of the pyloroduodenum and the adherent cyst was unsuccessful. Hence, the cyst was aspirated and the free wall of the cyst was excised. The epithelial lining of the cyst sharing a common wall with the pyloroduodenal area that was left in situ was cauterized. The histopathological examination revealed gastric and duodenal mucosa with small pancreatic inclusion, and a diagnosis of duplication cyst with an ectopic pancreatic tissue was made. Her recovery was uneventful. Her appetite has improved and she had gained 2 kg in 3 months.
Figure 2.
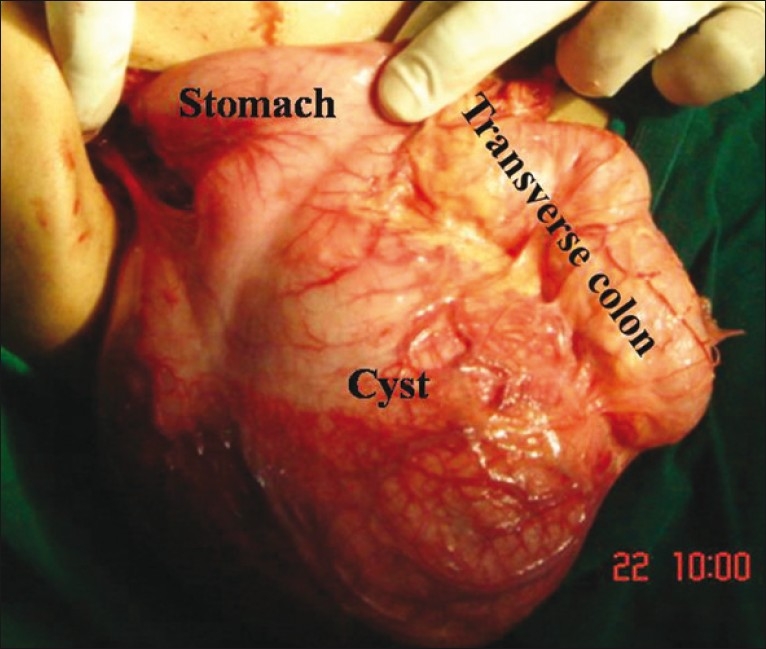
Per-operative photograph of the pyloroduodenal duplication cyst
DISCUSSION
Duplication of gastrointestinal tract is a rare congenital anomaly found in about 0.2% of all children.[5–7] The diagnosis should be considered when a child presents with features of gastric outlet obstruction. An USG and CECT scan of the abdomen are highly contributory in the diagnosis of intestinal duplication cysts. The pre-operative CECT scan gave us a fairly accurate diagnosis in addition to the dimensions, location and relations of the duplication cyst. An accurate pre-operative diagnosis helps in planning the surgical procedure and preparing the patient. Gastroduodenal duplications are usually managed surgically by total excision. The common wall between the stomach and the duplication cyst has to be dissected and, usually, it can be done without entering the stomach. But, in cases where one does not get a plane of dissection in the common wall, one should excise the common wall and suture the gastric defect, as leaving behind the common wall (gastric epithelium) would expose the child to inflammatory complications. In our patient, we performed subtotal excision of the cyst and cauterization of the epithelial lining instead of excision as we could not get a plane in the common wall. We felt it appropriate because of three reasons. Firstly, and most importantly, excision of the common wall would have meant gastroduodenectomy (excision of the pylorus and duodenum), which would have exposed the child to associated complications and morbidity of gastroduodenal anastomosis. Secondly, it would have increased the surgical and anesthesia time, and thirdly, it would have increased the hospital stay and the cost of treatment. We have been following the patient; she is growing well and has not experienced any complications so far.
To conclude, pyloroduodenal duplication cysts may be managed by subtotal excision and cauterization of the epithelial lining. It is a simple, safe and effective treatment option wherever it is difficult to find a plane of dissection in the common wall.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Tihansky DP, Sukarochana K, Hanrahan JB. Pyloroduodenal duplication cyst. Am J Gastroenterol. 1986;81:189–91. [PubMed] [Google Scholar]
- 2.Hamada Y, Inoue K, Hioki K. Pyloroduodenal duplication cyst: Case report. Pediatr Surg Int. 1997;12:194–5. [PubMed] [Google Scholar]
- 3.Sjekavica I, Batinica M, Lusic M, Senecic-cala I, Oberman B, Stern-Padovan R. Communicating saccular pyloroduodenal duplication. Radiol Oncol. 2005;39:181–4. [Google Scholar]
- 4.Upadhyaya VD, Srivastava PK, Jaiman R, Gangopadhyay AN, Gupta DK, Sharma SP. Duplication cyst of pyloroduodenal canal: A rare cause of neonatal gastric outlet obstruction: A case report. Cases J. 2009;2:42. doi: 10.1186/1757-1626-2-42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Bjornskov I, Bendsen AK. Cystic gastric leiomyoma: A diagnostic pitfall. Acta Gastroenterol Belg. 1997;60:238–9. [PubMed] [Google Scholar]
- 6.Murty TV, Bhargava RK, Rakas FS. Gastroduodenal duplications. J Pediatr Surg. 1992;4:515–7. doi: 10.1016/0022-3468(92)90351-7. [DOI] [PubMed] [Google Scholar]
- 7.Uzun MA, Koksal N, Kayahan M, Celik A, Kilicoglu G, Ozkara S. A rare case of duodenal duplication treated surgically. World J Gastroenterol. 2009;2:882–4. doi: 10.3748/wjg.15.882. [DOI] [PMC free article] [PubMed] [Google Scholar]