

Abstract
Objective:
The objective of the study was to evaluate the safety and efficacy of atorvastatin compared with simvastatin and pravastatin in patients of hyperlipidemia.
Materials and Methods:
This was a randomized, parallel group, open-label study conducted at KG hospital, Coimbatore, Tamilnadu, India. Twenty hyperlipidemia patients each taking atorvastatin 20 mg, pravastatin 20 mg and simvastatin 20 mg tablets were selected for the study after clinical and baseline investigations. The patients were reviewed after 3rd and 5th month of statin therapy for lipid profile. The liver enzyme levels (SGOT, SGPT, ALP), albumin, bilirubin, protein and biochemical infraction parameters (Creatine Kinase, Creatine Kinase - Myocardial Band) after 5th month of treatment with statins were also reviewed.
Results:
The results showed that atorvastatin significantly reduced the lipid levels (LDL-C, TC, TG, VLDL) when compared to simvastatin and pravastatin after 3rd and 5th month of treatment. Atorvastatin increased the HDL-C levels significantly when compared to simvastatin and pravastatin after 5 months of treatment. Atorvastatin also significantly reduced the CK levels when compared to pravastatin but no increase in liver enzyme levels was observed.
Conclusion:
The study showed that atorvastatin is more effective when compared to simvastatin and pravastatin in patients with hyperlipidemia.
KEY WORDS: Creatine kinase, creatine kinase - myocardial band, pravastatin, simvastatin
Introduction
Hyperlipidemia is a disorder of lipoprotein metabolism, which includes a number of abnormalities such as hypercholesterolemia and hypertriglyceridemia.[1] Recently World Health Organization (WHO) has declared that by 2020, 60% of cardiovascular cases will be of Indian origin.[2] Statins are the first line therapy for lowering lipid levels.[1] Treatment of hyperlipidemia with statins has become an integral part of management of vascular diseases.[3] Statins have become the leading prescription drug.[1] Indications of statins have been greatly extended over the last 5 years subsequent to the publication of many multicenter prospective trials. There are multiple statins available in the Indian market like atorvastatin, simvastatin, pravastatin, pitavastatin, fluvastatin, cerivastatin and rosuvastatin.[4] Most of the trials compared the fixed-dose regimens of more intensive statin therapy with less intensive statin therapy.[5] Recent studies in patients with stable coronary disease showed greater reduction in C-reactive protein (CRP) with higher dose than with lower dose of statins.[6] However, various studies suggest that efficacy and safety of various statins in hyperlipidemia differs considerably.[7] It is difficult for the medical practitioners to select suitable statins for their patients. Hence we have compared the efficacy and safety of atorvastatin with simvastatin and pravastatin in patients of hyperlipidemia.
Materials and Methods
Study Design
The randomized, open label, parallel group study was conducted at KG hospital, Coimbatore, Tamilnadu, India. This study was carried out from June 2009 to January 2010. The protocol was approved by Institutional Ethics Committee (IEC). Informed consent was obtained from the patients prior to the study.
Patient Selection
Twenty patients with hyperlipidemia each taking atorvastatin 20 mg or pravastatin 20 mg or simvastatin 20 mg tablets were selected for the study after clinical and baseline investigations. A family history of premature coronary heart disease (CHD) was given first priority for patient selection (includes parents and siblings). Males with age limit <55 years and females with age limit <65 years were also given first priority.[4] Patient details like body mass index (BMI),[6] education, occupation, smoking, alcohol intake, blood pressure,[8] dietary habits and family history were also considered before selecting the patients.
Inclusion Criteria
Male patients (35 – 55 years) and female patients (45 – 65 years) having low density lipoprotein cholesterol (LDL-C) higher than130 mg/dl and triglycerides (TG) more than 250 mg/dl were included in the study.
Exclusion Criteria
Patients with renal and hepatic failure, diabetes mellitus (I and II), pregnancy, hypothyroidism, uncontrolled hypertension, patients who had undergone bypass surgery, patients taking other lipid lowering agents like fibrates, niacin and patients who were taking cardiac drugs like warfarin, verapamil and amiodarone were excluded from the study.
Study visits and treatment schedule
The patients were randomized into three groups of 20 patients each taking 20 mg of atorvastatin, simvastatin and pravastatin according to the treatment regimen. Initial readings of lipid levels like LDL, TC, TG, HDL, VLDL were taken as baseline. First review values for the lipids were taken at the end of 3rd month, and the second review values were taken at the end of 5th month. For liver enzymes and creatine kinase (CK), creatine kinase – Myocardial Band (CK-MB) levels were taken before treatment and at the end of 5th month. Lipid parameters, liver enzymes, CK and CK-MB were measured by using autoanalyzer (Microlab-300X). Participants on the baseline were advised to take the medication according to treatment schedule.
Statistics
All the values were expressed in mean±SD. The baseline, first review and second review values of atorvastatin were compared with simvastatin and pravastatin by using one-way ANOVA followed by Tukey multiple comparison test. P<0.05 was considered as significant.
Results
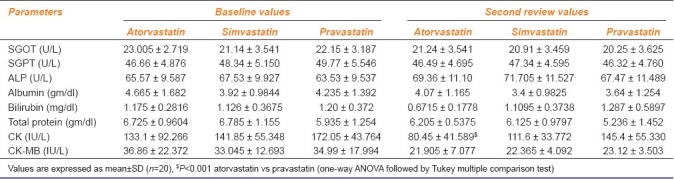
The baseline lipid profile values showed that, there was no significant difference between the groups. Atorvastatin produced significant reduction in lipids levels in comparison with simvastatin (LDL-C P<0.001, TC P<0.001, TG P<0.05, VLDL P<0.05) and pravastatin (LDL-C P<0.001, TC P<0.001, TG P<0.001, VLDL P<0.001) in the first review [Table 1]. The atorvastatin also produced significant reduction in lipid levels in comparison with simvastatin (LDL-C P<0.001, TC P<0.001, TG P<0.05, VLDL P<0.05) and pravastatin (LDL-C P<0.001, TC P<0.001, TG P<0.001, VLDL P<0.001) in the second review [Table 2]. Atorvastatin had increased the HDL-C levels significantly in comparison with simvastatin (P<0.001) and pravastatin (P<0.001) at second review. None of these drugs increase the liver enzyme levels after 5th month of treatment. But atorvastatin significantly (P<0.001) reduced CK levels when compared to pravastatin [Table 3].
Table 1.
Comparison of lipid profile of atorvastatin, simvastatin and pravastatin-treated groups at first review
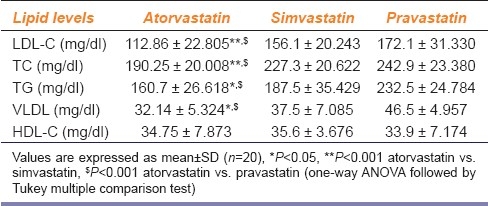
Table 2.
Comparison of lipid profile of atorvastatin, simvastatin and pravastatin-treated groups at second review
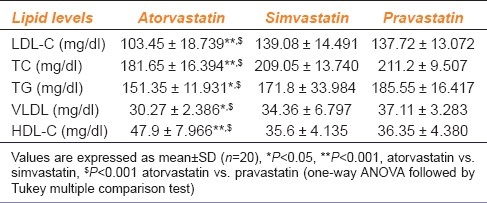
Table 3.
Comparison of enzymes, albumin and bilirubin levels of atorvastatin, simvastatin and pravastatin-treated groups at second review
Discussion
The study was designed to evaluate the safety and efficacy of atorvastatin compared with simvastatin and pravastatin in hyperlipidemia patients considering the previous reports of efficacy and safety of different statins. The results revealed that all three drugs (atorvastatin, simvastatin and pravastatin) reduces the lipid levels (LDL-C, TC, TG, VLDL) but atorvastatin produced significant reduction when compared to simvastatin and pravastatin in both first and second review [Tables 1 and 2]. Our results were consistent with the results of previous authors.[3,4,9] Our results also revealed that atorvastatin increases HDL-C levels significantly when compared to simvastatin and pravastatin at second review. In this study we have also compared the effect of atorvastatin with simvastatin and pravastatin on liver enzyme (SGOT, SGPT, ALP), bilirubin and albumin levels. The study showed that none of these drugs increase the liver enzyme levels significantly as compared with baseline value. None of these drugs damaged the liver in 5 months of treatment. These results contradicted with the results of previous studies.[10] There were no serious adverse events reported in this study. The biochemical markers that are widely used in the detection of infarction are CK, a more sensitive and cardio specific isoform of this enzyme was CK-MB.[10] Our study revealed that atorvastatin reduces the CK levels significantly when compared to pravastatin at second review. The present results were consistent with the result of Pasceri et al., who reported that pretreatment with atorvastatin decreases the incidence of myocardial injury during coronary intervention with placebo.[11] But results of Kernsa et al., contradict our results.[12] To conclude, our study revealed that atorvastatin is a more effective drug when compared to simvastatin and pravastatin in patients of hyperlipidemia. None of these drugs caused hepatotoxicity after 5 months of treatment. These results might be of value to practicing physicians while selecting suitable statins for these patients.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
References
- 1.Ravi GR, Pradeepa R, Mohan V. Hyperlipidemia and coronary artery disease. An Update. Indian Heart J. 2004;56:21–6. [PubMed] [Google Scholar]
- 2.Kumar T, Kapoor A. Premature coronary artery disease in North Indians: An angiography study of 1971 patients. Indian Heart J. 2005;57:311–8. [PubMed] [Google Scholar]
- 3.Wierzbicki AS, Lumb PJ, Semra Y, Chik G, Christ ER, Crook MA. Atorvastatin compared with simvastatin based therapies in the management of severe familial hyperlipidemia. QJM. 1999;92:387–94. doi: 10.1093/qjmed/92.7.387. [DOI] [PubMed] [Google Scholar]
- 4.Fleg JL, Mete M, Howard BV, Umans JG, Roman MJ, Ratner RE, et al. Effect of statins alone versus statins plus ezetimibe on carotid atherosclerosis in type 2 diabetes: The SANDS (Stop Atherosclerosis in Native Diabetics Study) trial. J Am Coll Cardiol. 2008;52:2198–205. doi: 10.1016/j.jacc.2008.10.031. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Josan K, Majundar SR, Mcalister FA. The efficacy and safety of intensive statin therapy: A meta analysis randomized trials. CMAJ. 2008;176:576–83. doi: 10.1503/cmaj.070675. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Anderson KM, Odell PM, Wilson PW, Kannel WB. Cardiovascular risk profiles. Am Heart J. 1991;121:293–8. doi: 10.1016/0002-8703(91)90861-b. [DOI] [PubMed] [Google Scholar]
- 7.Kinlay S, Schwartz GG, Olsson AG, Rifai N, Leslie SJ, Sasiela WJ, et al. High dose atorvastatin enhances the decline in inflammatory markers in patients with acute coronary syndromes. Circulation. 2003;26:571–81. doi: 10.1161/01.CIR.0000091404.09558.AF. [DOI] [PubMed] [Google Scholar]
- 8.Golomb B. Statins lower blood pressure. Arch Intern Med. 2008;184:243–9. [Google Scholar]
- 9.Jones P, Kafonek S, Laurora I, Hunninqhake D. Comparative dose efficacy study of atorvastatin versus simvastatin, pravastatin, lovastatin and fluvastatin in patients with hypercholesterolemia (the CURVES study) Am J Cardiol. 1998;81:582–7. doi: 10.1016/s0002-9149(97)00965-x. [DOI] [PubMed] [Google Scholar]
- 10.Walker R. Dyslipidemia. In: Roger W, Clivw E, editors. Clinical Pharmacy and Therapeutics. 3rd ed. Edinburgh: Churchil Livingstone; 2003. pp. 353–69. [Google Scholar]
- 11.Pasceri V, Patti G, Nusca A. Randomized trial of Atorvastatin for reduction of myocardial damage during coronary intervention. Circulation. 2004;110:674–8. doi: 10.1161/01.CIR.0000137828.06205.87. [DOI] [PubMed] [Google Scholar]
- 12.Kearnsa AK, Bilbiea CL, Clarkson PM, Whitec M, Sewright KA, Gadarl M, et al. The creatine kinase respose to eccentric exercise with atorvastatin 10 mg or 80 mg. Atherosclerosis. 2008;200:121–5. doi: 10.1016/j.atherosclerosis.2007.12.029. [DOI] [PubMed] [Google Scholar]