

Abstract
Background/Aim:
The compelling evidence reported that selenium is an essential trace mineral for human beings. Selenium plays a pivotal role in the restoration of immune functions. High rates of hepatitis B and C are present in Pakistan. Epidemiologic surveys demonstrated an inverse association between selenium (Se) level and regional cancer incidence, as well as viral infection. The present study was designed to evaluate the concentration of selenium in the serum of patients suffering from hepatitis B and C.
Patients and Methods:
In this cross-sectional descriptive analytical study, serum selenium concentration of 150 patients suffering from hepatitis B and C, along with 26 healthy controls, was determined by atomic absorption spectrophotometer equipped with hydride generation system, model Analytic Jena (Vario III).
Results:
The mean and standard deviation of serum selenium concentration observed in male and female patients with hepatitis C were 101.60±0.55 and 77.43±0.47 μ g/L, respectively, whereas the mean and standard deviation of serum selenium concentration observed in male and female patients with hepatitis B were 107.58±0.44 and 137.8±0.36 μg/L. Analysis of t test showed significant difference between C and B (P<0.001) patients in serum selenium concentration, when compared with the control.
Conclusion:
The obtained results indicate that serum selenium concentration of hepatitis B and C patients is less than serum selenium concentration of healthy individuals. However, serum selenium decline is relative to severity of disease. Based on findings of this study, it is proposed that selenium should be supplemented in such patients in order to optimize nutritional support and to get better treatment response.
Keywords: Hepatitis B and C, Pakistan, selenium level
Trace elements play a pivotal role in normal development, health, and protection of human body, as other essential nutrients do, and their insufficiency may result in a variety of diseases.[1] Among the trace elements, selenium (Se) in trace amounts is indispensable for the maintenance of good health.[2,3] It is an essential component of the enzyme glutathione peroxidase that prevents cellular damage from free radicals.[4] Selenium also plays a crucial role in the detoxification of liver enzymes, enhancing immune function as well as providing antioxidant defiance. Selenium is found in minute amounts in foods[5] with the richest source being found in meat, fish, whole grains, and dairy products. The recommended dietary allowances (RDA) of selenium in the USA are 55 μg/day for women and 70 μg/day for men.
Epidemiologic studies have shown that low grain selenium content is associated with a high regional incidence of hepatitis B viral infections.[6] Selenium deficiency has been involved in the pathogenesis of a number of clinical findings in chronic liver diseases. Hepatitis B and C are viral diseases resulting from DNA, and RNA type virus involves progressive immune dysfunction. The protective role of selenium against hepatitis was reported first in 1997. Different studies have shown lower concentration of selenium in the serum and erythrocytes of hepatitis B and C patients[7,8] and hepatitis B and C patients are at a high risk for poor response to bacterial and viral infections. Selenium deficiency reduces immune functions, increases inflammatory effects, resulting in impairment of the activities of leukocytes, neutrophil and macrophages.[9–11]
Hepatitis C viral infection is linked with low blood levels of antioxidants, including selenium[12–14] and elevated level of oxidative stress.[15–17] Four-year animal studies showed that nutritional supplement of selenium decreased the hepatitis B virus (HBV) infection by 77.2%.[18] The deficiency of selenium is common in patients with hepatitis due to poor appetite during infection, decrease in intake and absorption, decreased bioavailability, and increased losses because of malabsorption. The present study was designed with an objective to find out serum selenium concentrations in patients suffering from HBV and hepatitis C virus (HCV) in our setup and to suggest any recommendation if required, of selenium supplementation by health care planners, gastroenterologists, and hepatologists.
PATIENTS AND METHODS
Selection of hepatitis B and C patients
A total of 150 Pakistani individuals of both sexes aged between 18 and 60 years with hepatitis B and C were selected for the study. The randomly selected study group comprised 107 patients with HCV (71 male and 36 females) and 43 patients with HBV (38 male and 5 females). Samples were collected from Pakistan Institute of Medical Sciences (PIMS), Polyclinic Hospital, CDA Hospital, and Markaz Labs, located in Islamabad, the capital city of Pakistan. All the patients were examined by the consultant gastroenterologists and their entire medical history and physical examination were documented. Exclusion criteria were patients with heart diseases, obese persons, patients with diabetes mellitus, and those who had already been on total parenteral nutrition.
Main outcome measures
All subjects included in the study were screened for HBV and HCV by rapid methodth and confirmed by ELISA technique.
Selection of healthy subjects (controls)
A total of 26 apparently healthy subjects of both sexes, aged between 18 and 60 years residing in the same area were selected for this study. The subjects were all apparently healthy and were selected with no history of smoking, hypertension, and any acute or chronic liver pathology.
Sample collection and preservation
After taking informed consent and ethical approval from ethical committee of the institution, about 5 cc blood was taken from the antecubital vein of patients and healthy subjects. The samples were left undisturbed for 1 h to clot and were then centrifuged at 5000 rpm for 15 min. The collected sera were stored in Eppendorff vials at –20°C until further analysis.
Sample preparation and digestion
Before analysis all the glassware was washed in dilute nitric acid (HNO3 10%) and rinsed carefully with distilled water in order to keep out the risk of contamination. All the solutions and standard were prepared in double distilled water. A standard solution (1000 μg/L) of selenium was obtained from Merck, Germany. Working standards were prepared by appropriate dilution of the stock solution with (0.5% v/v) HNO3. HNO3 (65%), hydrochloric acid (HCl 37%), and sodium hydroxide (NaOH) were purchased from Merck, Germany, and perchloric acid (HClO4 70%) and sodium borohydride (NaBH4) were from BDH, UK origin.
The sodium borbhydride pellets were dissolved in a 1% sodium hydroxide solution to give 3% NaBH4. Three milliliters of 3% super pure HCl was used for hydride generator with continuous flow generation system HS-55. A sample of the serum (1 ml) was transferred to a Teflon beaker for mineralization, then 3 ml of HNO3/HCLO4 (1:1 v/v) was added. The temperature of the sample was then brought gradually to boiling point on a hot plate, until fumes of HClO4 appeared. Samples were then heated according to the following temperature/time scheme: 175°C/60 min, 200°C/60 min and finally 250°C/60 min. The mixture was then heated according to the following (temperature/ time) scheme: 175°C for 60 min, 200°C for 60 min, and finally 250°C for 60 min. The mixture was then left to cool down to room temperature. Then 10 ml of (6N) HCl was added and the sample was heated again on hot plate to 170°C for 30 min to reduce Se (VI) to Se (IV).
Sample analysis
The digested serum samples were analyzed for selenium by using atomic absorption spectrophotometer equipped with hydride generation system, model Analytic Jena (Vario III). Analytical calibration was accomplished with aqueous standards in 0.5% (v/v) HNO3. Fresh calibrations were made each time before analysis.
ADI calculation
ADI is the measure of the amount of a specific substance usually a food additive, or a residue of veterinary drug or pesticide in food or drinking water that can be ingested orally on a daily basis over a life time without an appreciable health risk and is calculated by using the following formula of Navarro et al.[19]

Statistical analysis
All statistical analysis including the calculation of mean±SD, range and variance were calculated. Level of significance was calculated using t test. P values >0.05 were considered nonsignificant.
RESULTS
The results presented in Table 1 show the age and gender wise distribution of mean serum selenium concentration (mg/L) along with ADI among male and female patients suffering from hepatitis C and B in comparison with healthy control. The mean serum selenium concentration in male HCV patients was 101.60±0.55 (mg/L), whereas the mean ADI calculated for HCV patients was 67.77±61.75 mg. The mean serum selenium concentration in female HCV patients was 77.43±0.47 (mg/L), while, the mean ADI was 51.62±36.78 mg, respectively.
Table 1.
Selenium concentration in HBV and HCV patients and control groups in Pakistani population
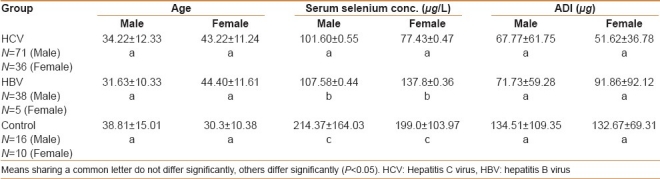
Age and gender wise distribution of selenium concentration and ADI among male and female patients affected due to hepatitis B were 107.58±0.44 μg/L. ADI calculated for HBV male patients was 71.73±59.28 mg. However, the serum selenium concentration and ADI of HBV female patients were 137.8±0.36 μg/L and 91.86±92.12 μg, respectively. The mean serum selenium concentration and ADI of healthy male were 214.37±164.03μg/L and 134.51±62.31 μg. The mean serum selenium concentration and ADI of healthy female were 199±103.97 μg/L and 132.67±69.31 μg, respectively.
Analysis of t test showed a significant difference between two groups regarding serum selenium concentration (P<0.001), however, no significant differences were observed between age and ADI among HBV and HCV patients.
DISCUSSION
Trace elements play an important role in one form or another form as a protective and therapeutic agent in combating disease. Disproportion in this trace element has been linked with a diversity of diseases. Selenium is an essential trace element for various animal species, including human beings.[16] The liver is known for its vital role in the metabolism and homeostasis of selenium in the human system,[17,18] as most of the selenoproteins are synthesized and secreted by the liver.[20,21]
The selenium concentration in healthy individuals reported in the present study were in the range of 30–580 mg/L, which were 90–470 mg/L in females and 30–580 mg/L among males. These results showed a higher concentration of selenium in males. By means of 1.51 (median correlation factor) as introduced by Navarro et al, to calculate the intake of nutrients on a daily basis, the daily intake of selenium in the present study was in the range of 60–313 mg for women in the age group of 18–46 years and 27–387 mg for men having age group in the range of 18-46 years.[19] The ADI was also decreased from 88.82 to 34.07 mg with increase in age. However, among the age group of 18–30 years, the mean ADI was just sufficient to the value recommended by American RDA (70 mg). Patients of the age group 31–60 years showed less ADI value than the recommended one. Aging occurs as a consequence of low antioxidants, rise in free radicals, as well as progressive defects in defense against free radicals damage. Free radicals are responsible for lipid peroxidation in cell membrane, which leak out lysosomal hydrolases causing muscle dystrophy, as a consequence muscles become weak. With growing age, the oxidative stress increases which damages DNA proteins and lipids of the skeletal muscles.[22,23]
Serum selenium concentration decreases as the disease progresses from acute to chronic stage.[24,25] In this context, other authors linked reduced serum selenium concentration with progression of severe cirrhotic conditions. Similarly, we also found low serum selenium concentration in patients with hepatitis B and C, which was 101.60±0.55 and 77.43±0.47 μg/L in male and female patients with hepatitis C, whereas in hepatitis B patients the concentration was 107.58±0.44 and 137.8±0.36 μg/L among male and female patients, respectively, showing significant (P<0.001) differences between HCV and HBV patients.
Al-Bader et al.[26] observed a significant decrease of serum selenium concentration accompanied by liver cirrhosis in rats when they were given thioacetamide, and the changes were reversed when selenium supplementation was introduced. On the other hand, Buljevac et al.[17] did not find significant differences in serum selenium concentrations in patients with liver cirrhosis and in those with liver cirrhosis and coexistent hepatocellular carcinoma, whereas Kalkan et al[27] also identified selenium deficiency in patients with viral hepatitis.
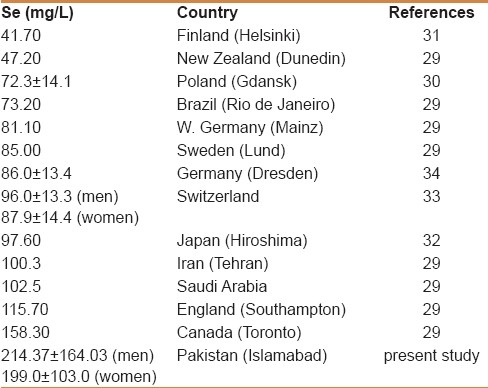
The results of our study are tabulated in Table 2. The concentration of selenium (μg/L) reported in the European countries, such as Finland, New Zealand, Poland, Brazil, W Germany, Sweden, Germany (Dresden), Switzerland, England, and Canada were 41.7l, 47.20, 72.3±14.1, 73.20, 81.10, 85.00, 86.0±13.4, and 96.0±13.3 (men), 87.9±14.4 (women), 115.70, 158.30, respectively, whereas the concentration of selenium (μg/L) reported in the serum of some Asian countries, such as Japan, Iran, and Saudi Arabia were 97.60, 100.3, 102.5, respectively,[28–33] whereas the concentration of selenium (μg/L) reported in the present study in Pakistani males was (214.37±164.03 μg/L) and in females was (199±103 mg/L), which is comparatively higher than the levels calculated for other countries, indicating that the normal Pakistani diet has an adequate content of selenium for both genders.
Table 2.
Review of literature of serum selenium concentration in healthy individuals the world over
Globally, the dietary intake of selenium varies extensively, as selenium concentrations in plant-based foods reflect the concentration of selenium in the soil where the plants were grown. The current dietary requirements for selenium by the Food and Nutrition Board of the Institute of Medicine are based to some extent upon maintenance of optimal levels of selenoproteins in blood, particularly plasma glutathione peroxidase.[34] The selenium requirement for prevention of chronic disease has not yet been definitively determined.[35] but however, for the optimal activity of glutathione peroxidase, the minimum values of serum selenium should be 100 μg/L or greater.[36]
Selenium is a micronutrient and its margin of usefulness and harmfulness is quite narrow. The observations in this study showed the importance of selenium measurement in hepatitis B and C patients and to identify the possible deficiency of selenium in these individuals. It is concluded that the serum selenium concentrations were low in patients suffering from hepatitis B and C as compared with healthy group. Intake of foods, such as sea foods, meat, and whole grains, which are generally good sources of selenium, may decrease the risk of hepatic damage in population predisposed to viral infections. As a consequence, we append, a diet poor in selenium sources, such as fruits and vegetables can increase hepatic damage in those who are predisposed to liver damage. Based on the findings of this study, it is suggested that patients suffering from hepatitis B and C should first undergo selenium deficiency test, then administration of selenium may be proposed if required, for such patients affected due to hepatitis B and C.
CONCLUSION
The findings of this study showed that serum selenium concentration of hepatitis B and C patients is less than serum selenium concentration of healthy individuals. Based on these findings, it is suggested that further interventional studies may be needed to analyze selenium concentration before and after supplementation and then recommendation may be given in such patients in order to optimize nutritional support and to get better treatment response.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Bukhari AQ, Ahmad S, Mirza M. The role of trace elements in health and disease. Elements in health and disease, Second International Conference. Pakistan: Hamdard Foundation; 1987. p. 116. [Google Scholar]
- 2.Thomson CD. Assessment of requirements for selenium and adequacy of selenium status: A review. Eur J Clin Nutr. 2004;58:391–402. doi: 10.1038/sj.ejcn.1601800. [DOI] [PubMed] [Google Scholar]
- 3.Goldhaber SB. Trace elements Risk assessment: Essentiality vs toxicity. Regul Toxicol Pharmacol. 2003;38:232–42. doi: 10.1016/s0273-2300(02)00020-x. [DOI] [PubMed] [Google Scholar]
- 4.Rotruck JT, Pope AL, Ganther HE, Swanson AB, Hafeman DG, Hoekstra WG. Selenium: Biochemical role as a component of glutathione peroxidase. Science. 1973;179:588–90. doi: 10.1126/science.179.4073.588. [DOI] [PubMed] [Google Scholar]
- 5.Glanze WD. Mosby Medical Encyclopedia. Revised ed. St. Louis, MO: CV Mosby; 1996. [Google Scholar]
- 6.Yu YS, Wen-Guang L, Ya-Jun Z, Wei-Ping Y, Chong H. Chemoprevention trial of human hepatitis with selenium supplementation in China. Biol Trace Elem Res. 1989;20:1–2. doi: 10.1007/BF02919094. [DOI] [PubMed] [Google Scholar]
- 7.Platis O, Anagnostopoulos G, Farmaki K, Posantzis M, Gotsis E, Tolis G. Glucose metabolism disorders improvement in patients with thalassaemia major after 24-36 months of intensive chelation therapy. Pediatr Endocrinol Rev. 2004;2(Suppl 2):279–81. [PubMed] [Google Scholar]
- 8.Cavallo-Perin P, Pacini G, Cerutti F, Bessone A, Condo C, Sacchetti L, et al. Insulin resistance and hyperinsulinemia in homozygous beta-thalassemia. Metabolism. 1995;44:281–6. doi: 10.1016/0026-0495(95)90155-8. [DOI] [PubMed] [Google Scholar]
- 9.Dimitrov N, Meyer C, Ullrey D. In: Selenium is a metabolic modulator of phagocytosis. In Selenium in Biology and Medicine. Combs GF, Levander OA, Spallholz J, Oldfield JE, editors. New York: AVI Publishing; 1984. pp. 254–62. [Google Scholar]
- 10.Boyne R, Arthur JR. The response of selenium-deficient mice to Candida albicans infection. J Nutr. 1986;116:816–22. doi: 10.1093/jn/116.5.816. [DOI] [PubMed] [Google Scholar]
- 11.Spallholz JE, Boylan LM, Larsen HS. Advances in understanding selenium's role in the immune system. Ann N Y Acad Sci. 1990;587:123–39. doi: 10.1111/j.1749-6632.1990.tb00140.x. [DOI] [PubMed] [Google Scholar]
- 12.Look MP, Rockstroh JK, Rao GS, Kreuzer KA, Barton S, Lemoch H, et al. Serum selenium, plasma glutathione (GSH) and erythrocyte glutathione peroxidase (GSH-Px)-levels in asymptomatic versus symptomatic human immunodeficiency virus-1 (HIV-1)-infection. Eur J Clin Nutr. 1997;51:266–72. doi: 10.1038/sj.ejcn.1600401. [DOI] [PubMed] [Google Scholar]
- 13.Yu MW, Horng IS, Hsu KH, Chiang YC, Liaw YF, Chen CJ. Plasma selenium levels and risk of hepatocellular carcinoma among men with chronic hepatitis virus infection. Am J Epidemiol. 1999;150:367–74. doi: 10.1093/oxfordjournals.aje.a010016. [DOI] [PubMed] [Google Scholar]
- 14.Jain SK, Pemberton PW, Smith A, McMahon RF, Burrows PC, Aboutwerat A, et al. Oxidative stress in chronic hepatitis C: Not just a feature of late stage disease. J Hepatol. 2002;36:805–11. doi: 10.1016/s0168-8278(02)00060-0. [DOI] [PubMed] [Google Scholar]
- 15.Yu SY, Zhu YJ, Li WG. Protective role of selenium against hepatitis b virus and primary liver cancer in Qidong. Biol Trace Elem Res. 1997;56:117–24. doi: 10.1007/BF02778987. [DOI] [PubMed] [Google Scholar]
- 16.Flohe L, Guzler WS, Loschn G. Trace elements in health and disease. Vol. 7. New York: Raven Press; 1979. The glutathione peroxidase reaction. A key to understanding the selenium requirements of mammals; pp. 263–86. [Google Scholar]
- 17.Buljevac M, Romic Z, Vucelic B, Banic M, Krznaric Z, Plesko S. Serum selenium concentration in patients with liver cirrhosis and hepatocellular carcinoma. Acta Med Croatica. 1996;50:11–4. [PubMed] [Google Scholar]
- 18.Whagner PD. Metabolism of selenium in humans. J Trace Elem Exp Med. 1998;11:227–40. [Google Scholar]
- 19.Navarro M, Lopez H, Ruiz ML, Gonzalez S, Perez V, Lopez MC. Determination of selenium in serum by hydride generation atomic absorption spectrometry for calculation of daily dietary intake. Sci Total Environ. 1995;175:245–52. doi: 10.1016/0048-9697(95)04859-6. [DOI] [PubMed] [Google Scholar]
- 20.Deagan JT, Butler JA, Zachara BA, Whanger PD. Determination of the distribution of selenium between glutathione peroxidase, selenoprotein P, and albumin in plasma. Anal Biochem. 1993;208:176–81. doi: 10.1006/abio.1993.1025. [DOI] [PubMed] [Google Scholar]
- 21.Behne D, Kyriakopoulos A. Mammalian selenium-containing proteins. Annu Rev Nutr. 2001;21:453–73. doi: 10.1146/annurev.nutr.21.1.453. [DOI] [PubMed] [Google Scholar]
- 22.Gianni P, Jan KJ, Douglas MJ, Stuart PM, Tarnopolsky MA. Oxidative stress and the mitochondrial theory of aging in human skeletal muscle. Exp Gerontol. 2004;39:1391–400. doi: 10.1016/j.exger.2004.06.002. [DOI] [PubMed] [Google Scholar]
- 23.Pansarasa O, Bertorelli L, Vecchiet J, Felzani G, Marzatico F. Age-dependent changes of antioxidant activities and markers of free radical damage in human skeletal muscle. Free Radic Biol Med. 1999;27:617–22. doi: 10.1016/s0891-5849(99)00108-2. [DOI] [PubMed] [Google Scholar]
- 24.Dworkin B, Rosenthal WS, Jankowski RH, Gordon GG, Haldea D. Low blood selenium levels in alcoholics with and without advanced liver disease: Correlation with clinical and nutritional status. Dig Dis Sci. 1985;30:838–44. doi: 10.1007/BF01309514. [DOI] [PubMed] [Google Scholar]
- 25.Conri C, Fleury B, Simonoff M, Ducloux G, Berdeu B, Moretto P. Blood selenium, zinc and copper in alcoholism. Ann Med Interne (Paris) 1988;139:138–9. [PubMed] [Google Scholar]
- 26.Al-Bader A, Abul H, Hussain T, Al-Moosawi M, Mathew TC, Dashti H. Selenium and liver cirrhosis. Mol Cell Biochem. 1998;185:1–6. doi: 10.1023/a:1006850514295. [DOI] [PubMed] [Google Scholar]
- 27.Kalkan A, Bulut V, Avci S, Celik I, Bingol NK. Trace elements in viral Hepatitis. J Trace Elem Med Biol. 2002;16:227–30. doi: 10.1016/S0946-672X(02)80049-9. [DOI] [PubMed] [Google Scholar]
- 28.Safaralizadeh R, Kardar GA, Pourpak Z, Moin M, Zare A, Teimourian S. Serum concentration of selenium in healthy individuals living in Tehran. Nutr J. 2005;4:32. doi: 10.1186/1475-2891-4-32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Hac E, Krechniak J, Szyszko M. Selenium in plasma of inhabitants of the Gdansk Region. J Environ Stud. 2001;4:275–8. [Google Scholar]
- 30.Westermarck T, Raunu P, Kirjarinta M, Lappalainen L. Selenium content of whole blood and serum in adults and children of different ages from different parts of Finland. Acta Pharmacol Toxicol (Copenh) 1997;40:465–75. [PubMed] [Google Scholar]
- 31.Hatano S, Nishi Y, Usui T. Plasma selenium concentration in healthy Japanese Children and adults determined by flameless atomic absorption spectrophotometry. J Pediatr Gastroenterol Nutr. 1984;3:426–31. doi: 10.1097/00005176-198406000-00021. [DOI] [PubMed] [Google Scholar]
- 32.Haldimann M, Venner TY, Zimmerli B. Determination of selenium in the serum of healthy Swiss adults and correlation to dietary intake. J Trace Elem Med Biol. 1996;10:31–45. doi: 10.1016/S0946-672X(96)80006-X. [DOI] [PubMed] [Google Scholar]
- 33.Meissner D. Reference values for blood and serum selenium in the Dresden area. Med Klin (Munich) 1997;92(Suppl 3):41–2. [PubMed] [Google Scholar]
- 34.Dietary Reference Intakes for Vitamin C, Vitamin E, Selenium, and Carotenoids. Washington, DC: National Academy Press; 2000. Food and Nutrition Board, Institute of Medicine. [PubMed] [Google Scholar]
- 35.Thomson CD. Assessment of requirements for selenium and adequacy of selenium status: A review. Eur J Clin Nutr. 2004;58:391–402. doi: 10.1038/sj.ejcn.1601800. [DOI] [PubMed] [Google Scholar]
- 36.Sauberlich HE. Laboratory Tests for the Assessment of Nutritional Status. 2nd ed. Boca Raton: CRC Press; 1999. [DOI] [PubMed] [Google Scholar]