

Abstract
Congenital malformations of the mitral valve are often complex and affect multiple segments of the valve apparatus. They may occur in isolation or in association with other congenital heart defects. The majority of mitral valve malformations are not simply classified, and descriptive terms with historical significance (parachute, mitral, or arcade) often lack the specificity that cardiac surgeons demand as part of preoperative echocardiographic morphological assessment. This paper examines the strengths and limitations of commonly used descriptions and classification systems of congenitally malformed mitral valves. It correlates pathological, surgical, and echocardiographic findings. Finally, it makes recommendations for the systematic evaluation of the congenitally malformed mitral valve using segmental echocardiographic analysis to assist precise communication and optimal surgical management.
Keywords: Congenital, echocardiography, mitral valve
INTRODUCTION
Clinically significant congenital mitral valve lesions are rare and estimated to affect 0.4%[1] of those with congenital heart disease or 5/100 000[2] of the general population. This is a likely underestimate as in the setting of congenital heart disease, mitral valve lesions are often incompletely documented.[3] The original classification and descriptions were based on the severe forms that attracted the attention of pathologists and surgeons. Cardiologists, however, frequently encounter milder, atypical, or incomplete forms of mitral valve defects that are often referred to as the forme fruste.[4,5] Echocardiography reveals that the prevalence of the minor mitral valve defects may be much higher than previously reported, up to 1% (11/1142) in healthy school-aged children.[6] This is similar to the reported prevalence of congenital aortic valve defects.[7,8]
Echocardiography (2-D or 3-D) allows for high resolution real-time evaluation of the mitral valve complex. The cardiac surgeon can now expect detailed preoperative echocardiographic morphological assessment to guide the accurate timing and nature of surgical management. Despite technological advances we still communicate with descriptive terms of historical significance including arcade, parachute, and hammock-like valves. Whilst such terms are not necessarily erroneous, they are simplistic and lack the specificity that surgeons currently demand in the description of congenital cardiac defects.
This paper aims to examine the strengths and weaknesses of commonly used classification systems and descriptions of congenital mitral valve lesions. It will make recommendations on how to systematically evaluate the congenitally malformed mitral valve using 2-D and 3-D echocardiography to assist precise communication and optimal surgical management. It will then identify the most common patterns of congenitally malformed mitral valves based on a systematic review and provide echocardiographic illustrations. Discussion will be limited to settings with concordant atrioventricular and ventricle-atrial connections with the exclusion of atrioventricular canal defects and hypoplastic left heart syndrome.
A literature review was performed using Medline and Embase to identify existing classifications of congenital mitral valve lesions. The search terms “congenital,” “mitral valve,” “surgery,” “pathology,” “stenosis,” and “regurgitation” were optimally combined. Limits applied to the search were “human,” “English,” and “child.” Only those studies that observed a cross-sectional population with minimal bias and a minimum patient cohort of 10 were included.
CLASSIFICATION OF CONGENITAL MITRAL VALVE LESIONS
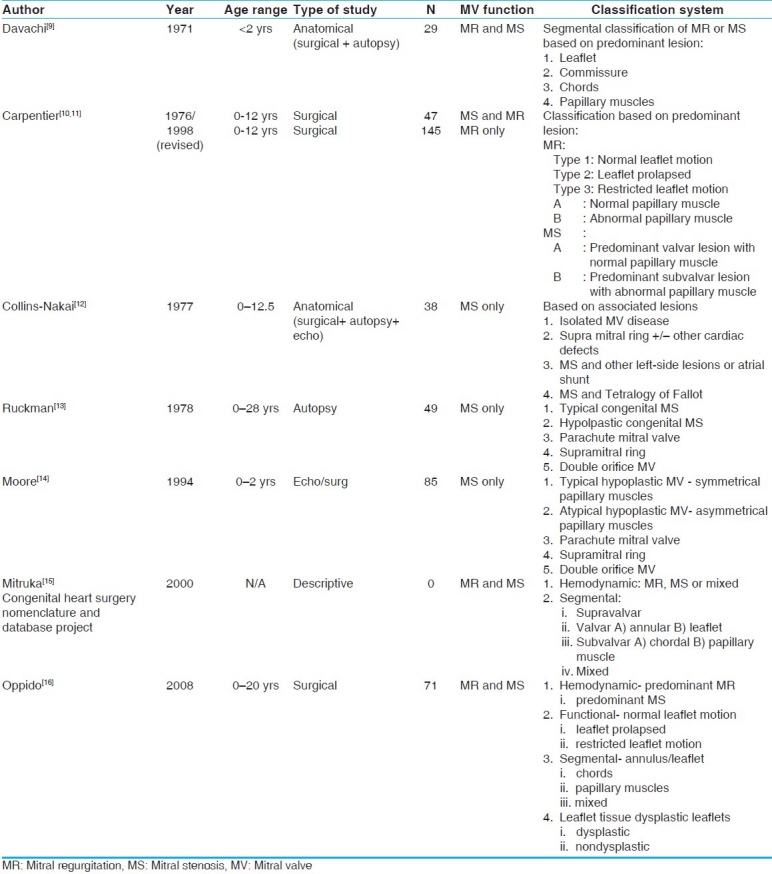
The literature search identified seven classification systems of congenital mitral valve lesions (in the setting of concordant atrioventricular and ventricle-atrial connections with the exclusion atrioventricular canal defects and hypoplastic left-heart syndrome) that are detailed in Table 1.
Table 1.
Classifications of congenital mitral valve disease
Anatomical classification systems: Based on post mortem studies
Davachi and colleagues in 1971, were one of the first to systematically assess and classify congenitally malformed mitral valves based on postmortem assessment.[9] They used a segmental classification according to whether the lesion affected the leaflets, commissures, tendinous chords, or papillary muscle arrangements. In 1977, Collins-Nakai et al. critiqued this segmental classification as they noted 97% (37 out of 38) of their patients with congenital mitral stenosis had more than one segment of the mitral valve apparatus affected.[12] They concluded that it was misleading to classify patients based on one anatomic segment of the mitral valve.[12] They proposed a classification based on associated cardiac defects (e.g., associated left-sided lesion, Tetralogy of Fallot, or no associated defects) [Table 1].
In 1978, Ruckman and van Praagh focused their attention on stenotic mitral valve defects and noted that typically congenital mitral stenosis affected multiple valve segments.[13] Commonly, the leaflet margins were thickened, tendinous chords appeared shortened, interchordal spaces were obliterated, and the two papillary muscles were underdeveloped and closely spaced. They coined the term “typical congenital mitral valve stenosis” to describe this most common defect with two distinct papillary muscle arrangements. The remainder of stenotic mitral valve defects were classified as “parachute mitral valve” (a single papillary muscle variant), “hypoplastic mitral valve” (miniature valve as seen in hypoplastic left heart syndrome), “double orifice mitral valve,” and “supramitral ring.” “Supramitral ring” earned category of its own even though from their work it was clear that it was rarely an isolated defect. As a result, by necessity, some patients were classified into multiple categories based on this system. In 1994, Moore et al.[14] expanded van Praagh's classification by adding “atypical congenital mitral stenosis” to differentiate between groups with symmetrical (typical mitral stenosis) and asymmetrical (atypical mitral stenosis) papillary muscle arrangements. His description of “atypical congenital mitral stenosis” resembled Oosthoek's[17] description of “parachute-like asymmetrical valve” (see complex mitral valve lesions).
Surgical classification
In 1976, Carpentier[10] et al. introduced a surgical classification system to specifically facilitate the development of tailored techniques for congenital mitral valve repair. It was based on the “predominant lesion,” as he also observed that multisegment pathology was the most prevalent. His description and classification was based on observations at surgery made via the left atrium. Prior to this all classifications were based on the pathologists’ view of the defect. The Carpentier classification was based on leaflet motion : Normal, restricted, or prolapsed. In addition it considered the predominant anatomic and hemodynamic effects [Table 1]. This description of congenital mitral valve defects was widely accepted and utilized over the next three decades.[10,11,16,18–25] His team dramatically expanded the repertoire of operative techniques and in doing so popularized mitral valve repair for congenital defects. In 2008, Oppido and colleagues[16] further refined the classification system by adding a further level to Carpentier's classification, the quality of leaflet tissue : Normal or dysplastic. In their surgical series dysplastic leaflets were associated with less favorable and less durable repairs.
Complex congenital MV lesions
Anatomical pathologists and cardiac surgeons introduced descriptive terms for what they perceived as very distinct congenital mitral valve lesions. However, many have argued that the majority of cases do to not fit the classic morphologic pattern but are the incomplete forms or the so called forme fruste.[5,17] As a result these descriptive terms are not stand-alone terms and require further clarification to facilitate effective communication.
“Parachute mitral valve” refers to an anomaly of the mitral valve apparatus where all tendinous cords insert into one papillary muscle as noted by Edwards[26] in 1963. The other papillary muscle is either absent or severely hypoplastic. As a pathologist, he observed the mitral valve through the incised left ventricle and noted that the anomaly had a parachute-like appearance. Others later observed that in the setting of isolated papillary muscle the tendinous chords are often short and fused with interchordal spaces partially or completely obliterated.[9,11,27,28] Commissures are frequently underdeveloped and the leaflets may be dysplastic or deficient. The combination of these lesions can give rise to a funnel rather than parachute-like appearance. It is frequently associated with a “supramitral ring”[9,13] that is often an integral part of the mitral valve leaflets.[29,30] It is a membranous or fibrous shelf that arises from the atrial side of the anterior mitral valve leaflet and posteriorly attaches to the leaflet, annulus, or the left atrial wall below the level of the left atrial appendage.[30] Parachute mitral valve is commonly classified as a malformation of the papillary muscles. However, that is too simplistic. It is often the associated lesions of other valve segments (e.g., commissural underdevelopment, dysplastic leaflets, shortened, and fused tendinous chords) that determine the severity of valvar dysfunction (stenosis and regurgitation) and hence the need for cardiac intervention. In addition to a supramitral ring, parachute mitral valves are frequently associated with subaortic obstruction and coarctation of the aorta. When obstruction at all four levels are present it is than referred to as Shone's complex.[28]
Parachute-like asymmetrical valve was described by Oosthoek[17] in 1997 as an anomaly that is an incomplete form of the true parachute valve with two papillary muscles : One hypoplastic and the other dominant receiving the majority of tendinous chords. He further described that one of the papillary muscles was often elongated, located higher in the left ventricle with its tip reaching to the annulus, and attached at both its base and lateral side to the left ventricular wall. The valve leaflets could be directly attached to hypoplastic papillary muscle. Parachute-like asymmetrical valves formed a spectrum of anomalies, rather than a well-defined entity. Only one out of Oosthoek's 29 cases could be described as a “true” parachute valve. Two decades earlier Rosenquest also demonstrated that most papillary muscle anomalies were often mild or incomplete forms (that were common amongst patients with coarctation) and that the “true” parachute anomaly, with a single papillary muscle, was rare.[5]
Anomalous mitral arcade was first described by Layman and Edwards in 1967 as “an anomaly of the mitral valve that consisted of connection of the left ventricular papillary muscles to the anterior mitral valve leaflet, either directly or through the interposition of unusually short tendinous chords.”[31] When viewed from the left ventricle the two papillary muscles resembled two pillars, and the bridging fibrous tissue in-between the papillary muscles resemble the arch of an arcade.
Hammock mitral valve was first described in 1976 by Carpentier[10] and it referred specifically to the appearance of the mitral valve apparatus from its left atrial aspect as viewed at cardiac surgery. The hammock appearance arose when the valvar orifice was at least partially obstructed by intermixed tendinous chords that attached to abnormal papillary muscles implanted just beneath the posterior leaflet.[32]
Correlation between Surgeons’ and Pathologists’ views of mitral valve morphology
These historical classifications and descriptions of common patterns of congenital mitral valve lesions highlight three important concepts. Firstly, the majority of congenital mitral valve defects are not limited to a single valve segment and it is often difficult to delineate the predominant effect. Secondly, the majority of the mitral valve lesions do not fit the classic descriptions and thus are incomplete or atypical. Thirdly, the classic descriptions of so called distinct congenital mitral valve lesions as described by surgeons and pathologists appear to overlap. For example as Carpentier stated “mitral arcade” is part of the hammock valve spectrum.[10] Hence, the papillary, chordal, and leaflet arrangement present in a hammock valve (when viewed from the left atrium) require these three structures take on an arrangement that appears like an arcade when viewed from a left ventricle. Later, Carpentier included Van Praagh's “typical congenital mitral valve stenosis” in the hammock valve spectrum.[32] Carefully reading Moore's[14] description of “atypical congenital mitral stenosis” and Oosthoek's[17] description of “parachute-like asymmetrical valves” it would be not unreasonable to conclude that they are all part of the spectrum of congenital mitral valve lesions rather than discreet entities.
International classification of congenital MV disease by the “congenital heart surgery nomenclature and database project”
In 2000, an international group reviewed the nomenclature for mitral valve disease for the purpose of establishing a unified reporting system to allow for pooling of data and systematic analysis of outcomes, risks and trends [Table 1].[15] Despite the difficulties noted by their predecessors, they proposed a contemporary anatomic classification (supravalvar, valvar, and subvalvar), but with one major difference. They developed a hierarchical system to allow for coding of multiple or complex anatomical defects in a systematic segmental format. The authors retained commonly used descriptive terms of historical significance (such as parachute and hammock valves).
Correlation of morphology with echocardiography
The obvious limitation of postmortem and surgical assessments is that they both observe the mitral valve in an unnatural cardiac state, during temporary or permanent cardiac arrest. Important technological advances over the last two decades have enabled high resolution 2-D and real-time 3-D echocardiographic assessment of the mitral valve morphology and function. Echocardiography, however has inherited picturesque descriptive terms of congenital mitral valve anomalies. These descriptions were based on surgeons’ and pathologists’ view of the incised heart. However, on echocardiography, the mitral valves do not resemble those classic descriptions of “hammock,” “arcade,” or “parachute.” Nor would those descriptions be sufficient today as the detail of description of malformations must match our technological advancements. Segmental analysis of the annulus, leaflets, commissures, chords, and papillary muscles is required for optimal management.[29] The focus for cardiologists is to describe rather than classify lesions as most forms are incomplete, as illustrated in Figure 1, Video 1a–d].[5,17]
Figure 1.
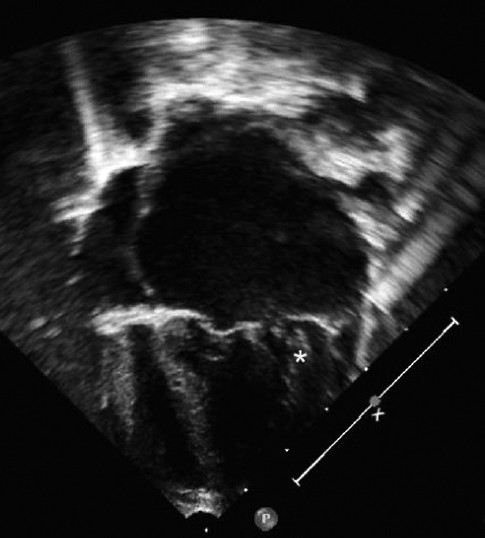
Video 1(a–d): Mixed congenital mitral regurgitation and stenosis. The mitral annuls is markedly dilated. The leaflets are thickened and dysplastic. The chords are abnormally short and fused. The anterolateral papillary muscle (*) inserts high, just below the level of the annulus
Studies have demonstrated that a high level of accuracy can be achieved when analyzing mitral valve pathology using 2-D echocardiography and an incremental benefit can be attained when combined with 3-D imaging when compared to findings at surgery.[33–35] 3-D imaging has the potential of advantage of better disease localization and segmental analysis.[36,37] The majority of comparative studies were derived from adult patients with mitral valve disease[36–39] or children with atrioventricular canal defect.[34,40] It appears that added benefits of 3-D echocardiography are also transferable to other rarer forms of congenital mitral valve lesions.[40,41] Studies suggest that the benefits of 3-D imaging are the greatest when transesophageal imaging is utilized in adult patients,[36,37] children have the advantage of having better transthoracic images. A number of authors have demonstrated the feasibility of performing rapid (5 min) focused real time 3-D echocardiographic imaging in nonsedated children as an add-on to comprehensive 2-D assessment.[42]
Correlation of morphology and mitral valve function
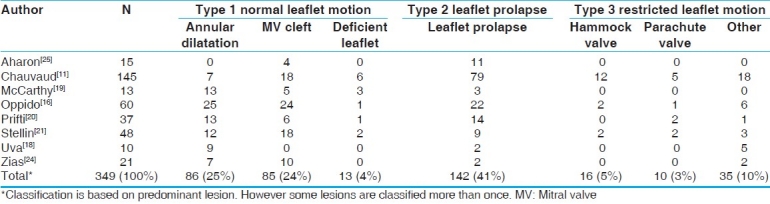
Observational data from cross-sectional populations with congenital mitral valve disease suggest that predominant mitral valve regurgitation is more common than mitral stenosis as a hemodynamic effect [Table 2].[16,18–21,24,25,43] These studies also demonstrate that the patterns of morphological features do not necessarily predict the hemodynamic effect. Complex lesion such as Carpentier's hammock valves (see above) are equally likely to lead to stenosis as regurgitation (pooled data).[10,11,16,18–22,24,25] Whilst, patients with isolated left-sided papillary muscles are more likely to present with stenosis, regurgitation is the predominant lesion in up to a fifth of patients (pooled data).[10,11,16,18–22,24,25] Authors that used Ruckman's and van Praagh's classification demonstrated that “typical congenital mitral valve stenosis” is the most common lesion that results in mitral stenosis [Table 3]. Whilst using Carpentier's classification the most common mechanism of mitral regurgitation is leaflet prolapse followed by annular dilatation and cleft of anterior leaflet [Table 4].
Table 2.
Prevalence of congenital MR relative to congenital MS
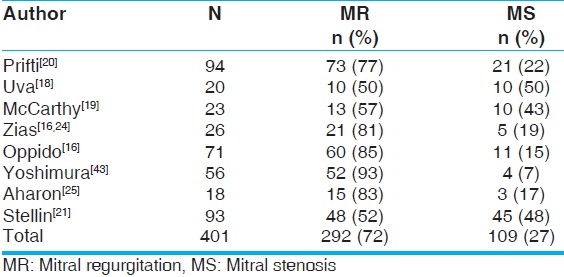
Table 3.
Common MV lesions that result in MS (van Praagh's classification)*

Table 4.
Common MV lesions that result in regurgitation (Carpentiers's classification)*
SYSTEMATIC ECHOCARDIOGRPHIC ASSESSMENT OF THE MITRAL VALVE
Mitral valve anomalies are frequently associated with other cardiac defects and hence a comprehensive congenital cardiac assessment is always essential and is beyond the scope of this article. There are published guidelines on standards for performing pediatric echocardiograms[47] and on how to grade severity of valvar stenosis and regurgitation.[48,49] As per the recommendations by the authors of the “international congenital data base project” all four segments of the mitral valve should be systematically assessed.[15] It is recommended that a comprehensive 2-D imaging should be performed prior to 3-D assessment.
Supravalvar region: The left atrium and the left atrial surface of the mitral valve leaflets should be carefully inspected. A supramitral ring can be missed unless suspected.[50] It is more commonly intra rather than in the supramitral position and is an integral part of the mitral valve leaflets [Figure 2, Video 2a–d].[29,30] A supramitral ring always inserts below the left atrial appendage whilst in cor triatriatum the membrane is between the level of the left atrial appendage and the pulmonary veins.[30]
Figure 2.
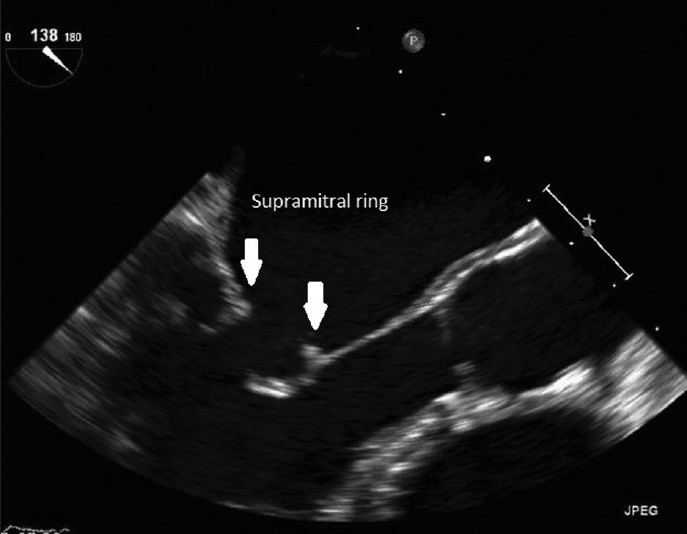
Video 2(a–d) Supramitral ring. The fibrous ring (arrows) is an integral part of the anterior and posterior mitral valve leaflets. The leaflet tips are thickened and chords are abnormally short. (a) 2-D TEE, (b) 2-D color TEE, (c) 3-D live, and (d) 3-D full volume acquisition
Annulus: The annulus of the mitral valve leaflet may be normal, dilated, hypoplastic, or in extreme cases atretic. It should be measured and then indexed to body surface area and expressed as a Z-score (normal deviate). Any deformity should be carefully noted.
Leaflets and commissures: The leaflet tissues may be normal, dysplastic, or thickened. Leaflets may be deficient, underdeveloped, or be associated with accessory tissue [Figure 1, Video 1(a–d]. A leaflet cleft is usually of the anterior mitral valve leaflet with chords often attached to its free edges [Figure 3, Video 3]. Clefts of the posterior mitral valve leaflet are rare and are often confused with normal (but pronounced) indentations of the posterior leaflet. Only clefts that affect the leaflet tissue between these indentations should be regarded as true clefts. Double orifice mitral valve may occur if there is duplication of the orifice with each suborifice supported by its own chordal apparatus [Figures 4a and 4b, Video 4(a–b]. Alternatively a bridging valvar tissue may divide the inlet. The commissures may be underdeveloped or absent. The mobility of the individual segments or scallops of the anterior and posterior mitral valve leaflets should be carefully assessed. Frequently restriction or prolapse is localized to segments rather than affecting the entire leaflet [Figure 5, Video 5].
Figure 3.
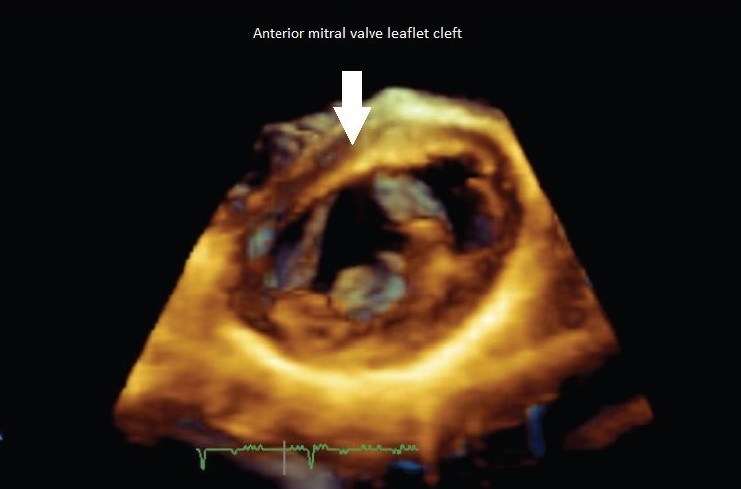
Video 3: Live 3-D transthoracic image of an anterior mitral valve leaflet cleft, left ventricular view
Figure 4.
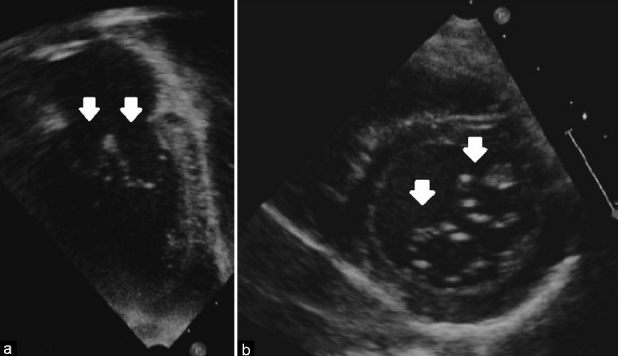
Video 4a–b: Double orifice mitral valve, transthoracic 2-D images. (a) Apical-four-chamber view. (b) Parasternal-short-axis-view. Arrows points to the two separate suborifices each supported by its own chordal apparatus
Figure 5.
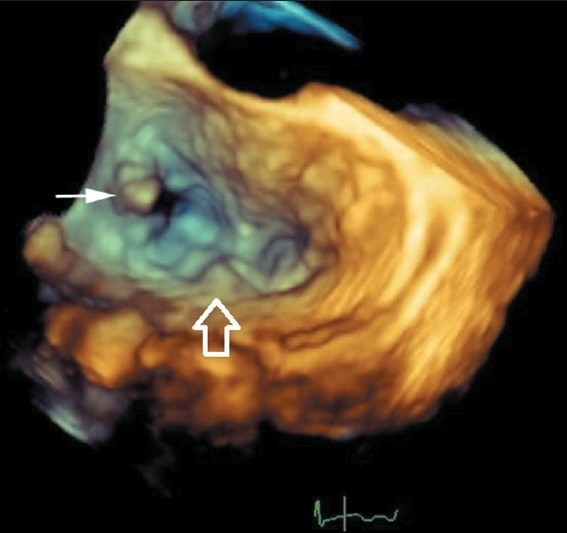
Video 5: Live 3-D transthoracic image of posterior mitral valve leaflet prolapse, left atrial view. The smaller solid points to a flail posterior medial (P1) segment and the larger arrow points to the middle scallop (P2 segment) prolapse
Tendinous chords: Both the primary chords that attach to the leaflet tips and the secondary chords that attach the body of the leaflet may be abnormally formed. Chords may be fuse, matted, thickened, and/or shortened and result in variable degrees of restriction of leaflet motion [Figure 1, Video 1(a–d]. The interchordal spaces may be partially or completely obliterated giving rise to a funnel appearance. When chords elongate, they can allow leaflet prolapse. In the absence of chords, the papillary muscles may directly insert into the leaflets. Insertion of the tendinous chords may be normal with equal distribution between the two papillary muscles or atypical with majority inserting into one dominant papillary muscle. Chords may also have septal attachments.
Papillary muscles: Papillary muscle arrangements may be normal with two symmetrical muscles located two-thirds of the way from the basal to the apical end of the left ventricular wall. Alternatively that arrangement may be asymmetrical (with one dominant papillary muscle), less commonly single (parachute valve), or multiple (as has been described with hammock valves) [Figure 6, Video 6]. Minor variations may also occur such that they be abnormally positioned, closely spaced or hypo- or hyperplastic [Figure 1, Video 1(a–d].
Figure 6.
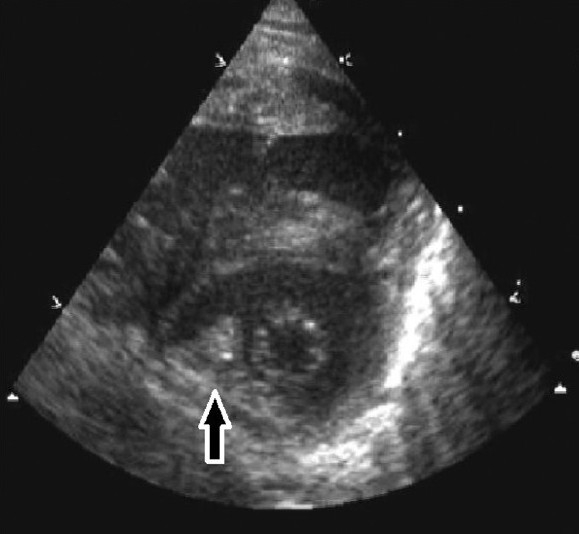
Video 6: Parachute mitral valve, transthoracic 2-D parasternal-short-axis-views. The arrow points to the single hypertrophied posteromedial papillary muscle. Note the eccentric opening of the mitral valve orifice
Once a comprehensive 2-D echocardiogram has been completed additional information can be gained by supplementing the echocardiographic study with transthoracic 3-D imaging. Generally three acquisition modes can be utilized : R0 eal time (narrow angle), zoom (magnified), and full volume or wide angle. The full volume mode requires ECG gating, because the data is compiled from independent narrower pyramidal sectors over four or more consecutive heartbeats. Full-volume acquisitions are prone to reconstruction or stitch artifacts. Older children may be able to hold their breath in expiration to minimize artifacts.[51]
Importance of systematic segmental assessment: Today, the ever expending repertoire of surgical techniques allow for individualized approach to mitral valve repair. There are various techniques to repair the annulus, to resect or enlarg e leaflets, and to adjust chordal and papillary muscle length. Operations are individualized to create an optimal balance, to normalize leaflet motion and coaptation. Many large centers have published ever improving results and experiences with surgical repair of congenitally malformed mitral valves. Nevertheless, mitral valve repair remains a challenge, particularly in infants and young children where alternatives such as mechanical and bioprosthetic valve replacement is associated with high mortality and morbidity.[52–55,14] Hence, in young children the question is not whether to repair or to replace but when to repair. In the first 12 months of life repair is technically difficult and should be avoided whenever possible.[32] The cardiologist's role is to systematically interrogate the mitral valve and assist the surgeon in estimating the likelihood of repair. Simple lesions that produce severe hemodynamic effects can often be successfully dealt with, for example, closure of a mitral valve cleft or resection of the supramitral membrane. However, in the setting of more complex lesions with dysplastic leaflets and grossly abnormal mitral valve apparatus optimizing medical management and delaying surgery is often the best strategy in the very young.
CONCLUSIONS
The majority of congenital mitral valve lesions are complex and affect multiple segments of the valve apparatus. Often it is too difficult to define the predominant lesion and predominant effect. The classical patterns of malformations are relatively rare and most can be characterized as the incomplete form or the forme fruste. On echocardiography, even the classical patterns of congenital mitral valves lesions do not give rise to a visual appearance of a parachute, hammock, or an arcade-like valve. However, a detailed segmental echocardiographic assessment can clearly define the pathology relating to the annulus, leaflet, commissures, chords, and papillary muscle arrangements. Generally there is a good correlation between 2-D echocardiographic findings and surgical morphology, which can be further supplement with 3-D imaging. A comprehensive echocardiographic assessment of a malformed mitral valve can guide the timing and nature of surgical repair.
Videos available on www.apc.com
ACKNOWLEDGEMENTS
We would like to acknowledge Dr. Louise Calder for her critical review of the manuscript. The primary author's research position was funded by Research Scholarships from the National Heart Foundation of New Zealand and the Lowitja Institute of Australia.
Footnotes
Source of Support: Research Scholarships from the National Heart Foundation of New Zealand and the Lowitja Institute of Australia,
Conflict of Interest: None declared.
REFERENCES
- 1.Nadas AS. Pediatric Cardiology. 3rd ed. Philadelphia: Saunders; 1972. [Google Scholar]
- 2.Mitchell SC, Korones SB, Berendes HW. Congenital heart disease in 56,109 Births incidence and natural history. Circulation. 1971;43:323–32. doi: 10.1161/01.cir.43.3.323. [DOI] [PubMed] [Google Scholar]
- 3.Hoffman JI, Kaplan S. The incidence of congenital heart disease. J Am Coll Cardiol. 2002;39:1890–900. doi: 10.1016/s0735-1097(02)01886-7. [DOI] [PubMed] [Google Scholar]
- 4.Celano V, Pieroni DR, Morera JA, Roland JM, Gingell RL. Two-dimensional echocardiographic examination of mitral valve abnormalities associated with coarctation of the aorta. Circulation. 1984;69:924–32. doi: 10.1161/01.cir.69.5.924. [DOI] [PubMed] [Google Scholar]
- 5.Rosenquist GC. Congenital mitral valve disease associated with coarctation of the aorta : A0 spectrum that includes parachute deformity of the mitral valve. Circulation. 1974;49:985–93. doi: 10.1161/01.cir.49.5.985. [DOI] [PubMed] [Google Scholar]
- 6.Webb RH, Wilson NJ, Lennon DR, Wilson EM, Nicholson RW, Gentles TL, et al. Optimising echocardiographic screening for rheumatic heart disease in New Zealand : N0 ot all valve disease is rheumatic. Cardiol Young. 2011;21:436–43. doi: 10.1017/S1047951111000266. [DOI] [PubMed] [Google Scholar]
- 7.Roberts WC. The congenitally bicuspid aortic valve : A0 study of 85 autopsy cases. Am J Cardiol. 1970;26:72–83. doi: 10.1016/0002-9149(70)90761-7. [DOI] [PubMed] [Google Scholar]
- 8.Basso C, Boschello M, Perrone C, Mecenero A, Cera A, Bicego D, et al. An echocardiographic survey of primary school children for bicuspid aortic valve. Am J Cardiol. 2004;93:661–3. doi: 10.1016/j.amjcard.2003.11.031. [DOI] [PubMed] [Google Scholar]
- 9.Davachi F, Moller JH, Edwards JE. Diseases of the mitral valve in infancy.An anatomic analysis of 55 cases. Circulation. 1971;43:565–79. doi: 10.1161/01.cir.43.4.565. [DOI] [PubMed] [Google Scholar]
- 10.Carpentier A, Branchini B, Cour JC, Asfaou E, Villani M, Deloche A, et al. Congenital malformations of the mitral valve in children.Pathology and surgical treatment. J Thorac Cardiovasc Surg. 1976;72:854–66. [PubMed] [Google Scholar]
- 11.Chauvaud S, Fuzellier JF, Houel R, Berrebi A, Mihaileanu S, Carpentier A. Reconstructive surgery in congenital mitral valve insufficiency (Carpentier's techniques) : Long-term results. J Thorac Cardiovasc Surg. 1998;115:84–93. doi: 10.1016/s0022-5223(98)99001-8. discussion 92-3. [DOI] [PubMed] [Google Scholar]
- 12.Collins-Nakai RL, Rosenthal A, Castaneda AR, Bernhard WF, Nadas AS. Congenital mitral stenosis. A review of 20 years’ experience. Circulation. 1977;56:1039–47. doi: 10.1161/01.cir.56.6.1039. [DOI] [PubMed] [Google Scholar]
- 13.Ruckman RN, van Praagh R. Anatomic types of congenital mitral stenosis : Report of 49 autopsy cases with consideration of diagnosis and surgical implications. Am J Cardiol. 1978;42:592–601. doi: 10.1016/0002-9149(78)90629-x. [DOI] [PubMed] [Google Scholar]
- 14.Moore P, Adatia I, Spevak PJ, Keane JF, Perry SB, Castaneda AR, et al. Severe congenital mitral stenosis in infants. Circulation. 1994;89:2099–106. doi: 10.1161/01.cir.89.5.2099. [DOI] [PubMed] [Google Scholar]
- 15.Mitruka SN, Lamberti JJ. Congenital heart surgery nomenclature and database project : M0 itral valve disease. Ann Thorac Surg. 2000;69(4 Suppl):S132–46. doi: 10.1016/s0003-4975(99)01360-0. [DOI] [PubMed] [Google Scholar]
- 16.Oppido G, Davies B, McMullan DM, Cochrane AD, Cheung MM, d’Udekem Y, et al. Surgical treatment of congenital mitral valve disease : Midterm results of a repair-oriented policy. J Thorac Cardiovasc Surg. 2008;135:1313–20. doi: 10.1016/j.jtcvs.2007.09.071. discussion 1320-1. [DOI] [PubMed] [Google Scholar]
- 17.Oosthoek PW, Wenink AC, Macedo AJ, Gittenberger-de Groot AC. The parachute-like asymmetric mitral valve and its two papillary muscles. J Thorac Cardiovasc Surg. 1997;114:9–15. doi: 10.1016/S0022-5223(97)70111-9. [DOI] [PubMed] [Google Scholar]
- 18.Uva MS, Galletti L, Gayet FL, Piot D, Serraf A, Bruniaux J, et al. Surgery for congenital mitral valve disease in the first year of life. J Thorac Cardiovasc Surg. 1995;109:164–74. doi: 10.1016/S0022-5223(95)70432-9. discussion 174-6. [DOI] [PubMed] [Google Scholar]
- 19.McCarthy JF, Neligan MC, Wood AE. Ten years’ experience of an aggressive reparative approach to congenital mitral valve anomalies. Eur J Cardiothorac Surg. 1996;10:534–9. doi: 10.1016/s1010-7940(96)80420-9. [DOI] [PubMed] [Google Scholar]
- 20.Prifti E, Vanini V, Bonacchi M, Frati G, Bernabei M, Giunti G, et al. Repair of congenital malformations of the mitral valve: Early and midterm results. Ann Thorac Surg. 2002;73:614–21. doi: 10.1016/s0003-4975(01)03419-1. [DOI] [PubMed] [Google Scholar]
- 21.Stellin G, Padalino MA, Vida VL, Boccuzzo G, Orrù E, Biffanti R, et al. Surgical repair of congenital mitral valve malformations in infancy and childhood : A single-center 36-year experience. J Thorac Cardiovasc Surg. 2010;140:1238–44. doi: 10.1016/j.jtcvs.2010.05.016. [DOI] [PubMed] [Google Scholar]
- 22.Serraf A, Zoghbi J, Belli E, Lacour-Gayet F, Aznag H, Houyel L, et al. Congenital mitral stenosis with or without associated defects : A evolving surgical strategy. Circulation. 2000;102(19 Suppl 3):III66–71. doi: 10.1161/01.cir.102.suppl_3.iii-166. [DOI] [PubMed] [Google Scholar]
- 23.Wood AE, Healy DG, Nolke L, Duff D, Oslizlok P, Walsh K. Mitral valve reconstruction in a pediatric population : Late clinical results and predictors of long-term outcome. J Thorac Cardiovasc Surg. 2005;130:66–73. doi: 10.1016/j.jtcvs.2005.03.025. [DOI] [PubMed] [Google Scholar]
- 24.Zias EA, Mavroudis C, Backer CL, Kohr LM, Gotteiner NL, Rocchini AP. Surgical repair of the congenitally malformed mitral valve in infants and children. Ann Thorac Surg. 1998;66:1551–9. doi: 10.1016/s0003-4975(98)00933-3. [DOI] [PubMed] [Google Scholar]
- 25.Aharon AS, Laks H, Drinkwater DC, Chugh R, Gates RN, Grant PW, et al. Early and late results of mitral valve repair in children. J Thorac Cardiovasc Surg. 1994;107:1262–70. discussion 1270-1. [PubMed] [Google Scholar]
- 26.Schiebler GL, Edwards JE, Burchell HB, DuShane JW, Ongley PA, Wood EH. Congenital corrected transposition of the great vessels : A study of 33 cases. Pediatrics. 1961;27(Suppl):849–88. [PubMed] [Google Scholar]
- 27.Hoashi T, Bove EL, Devaney EJ, Hirsch JC, Ohye RG. Mitral valve repair for congenital mitral valve stenosis in the pediatric population. Ann Thorac Surg. 2010;90:36–41. doi: 10.1016/j.athoracsur.2010.03.099. [DOI] [PubMed] [Google Scholar]
- 28.Shone JD, Sellers RD, Anderson RC, Adams P, Jr, Lillehei CW, Edwards JE. The developmental complex of “parachute mitral valve,” supravalvular ring of left atrium, subaortic stenosis, and coarctation of aorta. Am J Cardiol. 1963;11:714–25. doi: 10.1016/0002-9149(63)90098-5. [DOI] [PubMed] [Google Scholar]
- 29.Asante-Korang A, O’Leary PW, Anderson RH. Anatomy and echocardiography of the normal and abnormal mitral valve. Cardiol Young. 2006;16(Suppl 3):27–34. doi: 10.1017/s1047951106000734. [DOI] [PubMed] [Google Scholar]
- 30.Banerjee A, Kohl T, Silverman NH. Echocardiographic evaluation of congenital mitral valve anomalies in children. Am J Cardiol. 1995;76:1284–91. doi: 10.1016/s0002-9149(99)80357-9. [DOI] [PubMed] [Google Scholar]
- 31.Layman TE, Edwards JE. Anomalous mitral arcade. A type of congenital mitral insufficiency. Circulation. 1967;35:389–95. doi: 10.1161/01.cir.35.2.389. [DOI] [PubMed] [Google Scholar]
- 32.Carpentier A, Brizard CP. Congenital malformations of the mitral valve. In: Stark J, Leval M, Tsang V, editors. Surgery for congenital heart defects. London: Wiley; 2006. pp. 573–90. [Google Scholar]
- 33.García-Orta R, Moreno E, Vidal M, Ruiz-López F, Oyonarte JM, Lara J, et al. Three-dimensional versus two-dimensional transesophageal echocardiography in mitral valve repair. J Am Soc Echocardiogr. 2007;20:4–12. doi: 10.1016/j.echo.2006.07.005. [DOI] [PubMed] [Google Scholar]
- 34.Takahashi K, Guerra V, Roman KS, Nii M, Redington A, Smallhorn JF. Three-dimensional echocardiography improves the understanding of the mechanisms and site of left atrioventricular valve regurgitation in atrioventricular septal defect. J Am Soc Echocardiogr. 2006;19:1502–10. doi: 10.1016/j.echo.2006.07.011. [DOI] [PubMed] [Google Scholar]
- 35.Barrea C, Levasseur S, Roman K, Nii M, Coles JG, Williams WG, et al. Three-dimensional echocardiography improves the understanding of left atrioventricular valve morphology and function in atrioventricular septal defects undergoing patch augmentation. J Thorac Cardiovasc Surg. 2005;129:746–53. doi: 10.1016/j.jtcvs.2004.07.023. [DOI] [PubMed] [Google Scholar]
- 36.Ben Zekry S, Nagueh SF, Little SH, Quinones MA, McCulloch ML, Karanbir S, et al. Comparative accuracy of two- and three-dimensional transthoracic and transesophageal echocardiography in identifying mitral valve pathology in patients undergoing mitral valve repair : I0 nitial observations. J Am Soc Echocardiogr. 2011;24:1079–85. doi: 10.1016/j.echo.2011.06.011. [DOI] [PubMed] [Google Scholar]
- 37.Pepi M, Tamborini G, Maltagliati A, Galli CA, Sisillo E, Salvi L, et al. Head-to-head comparison of two- and three-dimensional transthoracic and transesophageal echocardiography in the localization of mitral valve prolapse. J Am Coll Cardiol. 2006;48:2524–30. doi: 10.1016/j.jacc.2006.02.079. [DOI] [PubMed] [Google Scholar]
- 38.Sugeng L, Shernan SK, Salgo IS, Weinert L, Shook D, Raman J, et al. Live 3-dimensional transesophageal echocardiography initial experience using the fully-sampled matrix array probe. J Am Coll Cardiol. 2008;52:446–9. doi: 10.1016/j.jacc.2008.04.038. [DOI] [PubMed] [Google Scholar]
- 39.Sharma R, Mann J, Drummond L, Livesey SA, Simpson IA. The evaluation of real-time 3-dimensional transthoracic echocardiography for the preoperative functional assessment of patients with mitral valve prolapse : A comparison with 2-dimensional transesophageal echocardiography. J Am Soc Echocardiogr. 2007;20:934–40. doi: 10.1016/j.echo.2007.01.028. [DOI] [PubMed] [Google Scholar]
- 40.Seliem MA, Fedec A, Szwast A, Farrell PE, Jr, Ewing S, Gruber PJ, et al. Atrioventricular valve morphology and dynamics in congenital heart disease as imaged with real-time 3-dimensional matrix-array echocardiography : Comparison with 2-dimensional imaging and surgical findings. J Am Soc Echocardiogr. 2007;20:869–76. doi: 10.1016/j.echo.2006.11.025. [DOI] [PubMed] [Google Scholar]
- 41.Espinola-Zavaleta N, Vargas-Barrón J, Keirns C, Rivera G, Romero-Cárdenas A, Roldán J, et al. Three-dimensional echocardiography in congenital malformations of the mitral valve. J Am Soc Echocardiogr. 2002;15:468–72. doi: 10.1067/mje.2002.115772. [DOI] [PubMed] [Google Scholar]
- 42.Balestrini L, Fleishman C, Lanzoni L, Kisslo J, Resai Bengur A, Sanders SP, et al. Real-time 3-dimensional echocardiography evaluation of congenital heart disease. J Am Soc Echocardiogr. 2000;13:171–6. doi: 10.1067/mje.2000.102988. [DOI] [PubMed] [Google Scholar]
- 43.Yoshimura N, Yamaguchi M, Oshima Y, Oka S, Ootaki Y, Murakami H, et al. Surgery for mitral valve disease in the pediatric age group. J Thorac Cardiovasc Surg. 1999;118:99–106. doi: 10.1016/S0022-5223(99)70148-0. [DOI] [PubMed] [Google Scholar]
- 44.Selamet Tierney ES, Graham DA, McElhinney DB, Trevey S, Freed MD, Colan SD, et al. Echocardiographic predictors of mitral stenosis-related death or intervention in infants. Am Heart J. 2008;156:384–90. doi: 10.1016/j.ahj.2008.03.019. [DOI] [PubMed] [Google Scholar]
- 45.McElhinney DB, Sherwood MC, Keane JF, del Nido PJ, Almond CS, Lock JE. Current Management of Severe Congenital Mitral Stenosis : O0 utcomes of Transcatheter and Surgical Therapy in 108 Infants and Children. Circulation. 2005;112:707–14. doi: 10.1161/CIRCULATIONAHA.104.500207. [DOI] [PubMed] [Google Scholar]
- 46.Coles JG, Williams WG, Watanabe T, Duncan KF, Sherret H, Dasmahapatra HK, et al. Surgical experience with reparative techniques in patients with congenital mitral valvular anomalies. Circulation. 1987;76:III117–22. [PubMed] [Google Scholar]
- 47.Lai WW, Geva T, Shirali GS, Frommelt PC, Humes RA, Brook MM, et al. Guidelines and standards for performance of a pediatric echocardiogram : A0 report from the Task Force of the Pediatric Council of the American Society of Echocardiography. J Am Soc Echocardiogr. 2006;19:1413–30. doi: 10.1016/j.echo.2006.09.001. [DOI] [PubMed] [Google Scholar]
- 48.Baumgartner H, Hung J, Bermejo J, Chambers JB, Evangelista A, Griffin BP, et al. Echocardiographic assessment of valve stenosis : EAE/ASE recommendations for clinical practice. Eur J Echocardiogr. 2009;10:1–25. doi: 10.1093/ejechocard/jen303. [DOI] [PubMed] [Google Scholar]
- 49.Zoghbi WA, Enriquez-Sarano M, Foster E, Grayburn PA, Kraft CD, Levine RA, et al. Recommendations for evaluation of the severity of native valvular regurgitation with two-dimensional and Doppler echocardiography. J Am Soc Echocardiogr. 2003;16:777–802. doi: 10.1016/S0894-7317(03)00335-3. [DOI] [PubMed] [Google Scholar]
- 50.Magee AG, Boutin C, McCrindle BW, Smallhorn JF. Echocardiography and cardiac catheterization in the preoperative assessment of ventricular septal defect in infancy. Am Heart J. 1998;135:907–13. doi: 10.1016/s0002-8703(98)70053-5. [DOI] [PubMed] [Google Scholar]
- 51.Sugeng L, Coon P, Weinert L, Jolly N, Lammertin G, Bednarz JE, et al. Use of real-time 3-dimensional transthoracic echocardiography in the evaluation of mitral valve disease. J Am Soc Echocardiogr. 2006;19:413–21. doi: 10.1016/j.echo.2005.11.016. [DOI] [PubMed] [Google Scholar]
- 52.Antunes MJ, Vanderdonck KM, Sussman MJ. Mechanical valve replacement in children and teenagers. Eur J Cardiothorac Surg. 1989;3:222–8. doi: 10.1016/1010-7940(89)90070-5. [DOI] [PubMed] [Google Scholar]
- 53.Beierlein W, Becker V, Yates R, Tsang V, Elliott M, de Leval M, et al. Long-term follow-up after mitral valve replacement in childhood : Poor event-free survival in the young child. Eur J Cardiothorac Surg. 2007;31:860–5. doi: 10.1016/j.ejcts.2007.02.006. [DOI] [PubMed] [Google Scholar]
- 54.Zweng TN, Bluett MK, Mosca R, Callow LB, Bove EL. Mitral valve replacement in the first 5 years of life. Ann Thorac Surg. 1989;47:720–4. doi: 10.1016/0003-4975(89)90126-4. [DOI] [PubMed] [Google Scholar]
- 55.Günther T, Mazzitelli D, Schreiber C, Wottke M, Paek SU, Meisner H, et al. Mitral-valve replacement in children under 6 years of age. Eur J Cardiothorac Surg. 2000;17:426–30. doi: 10.1016/s1010-7940(00)00353-5. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.