

Abstract
Introduction:
HIV/AIDS can lead to poverty affecting particularly women and young people and can halt or reverse socioeconomic development of a country.
Objective:
The objective of this study was to assess the socioeconomic consequences of HIV/AIDS within the family.
Materials and Methods:
A cross-sectional descriptive study was carried out among patients admitted in in-patient department and those attending integrated counseling and testing centre (ICTC) of School of Tropical Medicine, Kolkata. Data were gathered by interviewing the patients by using a predesigned questionnaire.
Results:
For prolonged duration and severity of disease, higher proportion of indoor patients reported loss of job, decreased family income, increased expenditure for care seeking, and faced greater economic consequences, reflected by selling assets. Loss of job was mainly due to illness (86.8%), disclosure of sero-status (13.2%), and predominantly among skilled workers. Assets were sold mainly to meet the cost of own illness for indoor patients, but more to meet the expenditure for husband's illness, in the case of ICTC patients. High school dropout seen in both groups was mainly due to economic reasons. HIV/AIDS status was known to other members of family for 84.8% of indoor patients out of which 15.4% experienced rejection by family members. Out of 72 ever married women indoor patients whose in-laws were aware of their HIV/AIDS status, 41.7%, 40.9%, and 33.33% reportedly were blamed for spouse's illness, and had strained relation with in-laws and spouse, respectively.
Conclusion:
Intensive behavior change communication and provision of care and support are required to curb AIDS-related stigma, discrimination, and to maintain physical, mental, and social wellbeing of people living with HIV/AIDS.
Keywords: HIV/AIDS, people living with HIV/AIDS, sero-status, socioeconomic consequences
INTRODUCTION
HIV/AIDS is a threat to social and economic development. Treatment of HIV/AIDS patients must be accompanied with other social measures to enhance their physical, mental, and social wellbeing. HIV/AIDS can lead to poverty, affecting particularly women and young people. Weakened family and societal support systems, decreased participation in formal education of young people as a result of AIDS in the family, along with depleted family income due to loss of work, and poor disease management present additional vulnerabilities.1 The growing number of HIV-infected women – many married or in single-partner relationship - highlights the importance of specific programs to empower the women.
Effective prevention and care in enabling environments can only help the HIV/AIDS patients to overcome the devastating outcomes of the disease. By an appropriate response to support those affected by HIV/AIDS, everyone gains and no one loses. Families’ gain as the income from work will continue, children gain as they continue to receive support from their family. In this way people living with HIV/AIDS (PLWHAs) remain productive for longer. The state gains because production is not disrupted in key sectors.2 Against this background, the present study was undertaken to assess the socioeconomic consequences of HIV/AIDS in the family.
MATERIALS AND METHODS
An institution-based cross-sectional, observational study was carried out for a period of 3 months from July to October 2008 among the HIV/AIDS patients attending the Calcutta School of Tropical Medicine, Kolkata. All patients attending the integrated counseling and testing centre (ICTC) and newly diagnosed to be infected with HIV, as well as all indoor patients with HIV/AIDS admitted during the study period, were considered for the study. Only patients willing to participate in the study were included and were interviewed in the presence of a trained counselor, after taking their informed consent and ensuring complete anonymity and confidentiality. A total of 292 PLWHAs (200 attending ICTC and 92 admitted in the hospital) were thus selected. Information pertaining to age, sex, marital status, occupation, family income, and expenditure including cost incurred to treatment, schooling of children, perception of family members toward the PLWHAs, etc. was obtained by the help of a predesigned, pretested, semistructured questionnaire in English, translated in Bengali/Hindi. The data were analyzed by using proportions, chi-square and z-tests for proportions.
RESULTS
The analysis revealed that majority of the patients were male, constituting 80.4% indoor and 66.5% newly diagnosed ICTC patients with M:F=2.44:1. Overall mean age of the participants was 33.07 years and 77.7% were less than 40 years of age. Hindus constituted the majority (80.0%) of the population followed by 15.1% Muslims and 2.4% Christians. The spectrum of educational status of PLWHAs ranged from illiteracy in 17.4% of indoor and 24% of ICTC patients to graduation in 8% of indoor and 5% of ICTC patients. About three-fourth of the PLWHAs belonged to rural and semiurban areas. History of migration was almost equally present in both indoor (50%) and outdoor (51%) patients. Majority, 72.6% of the patients were currently married. 21.7% of indoor and 15% of newly diagnosed patients was unmarried.
A total of 63% of indoor and 49% of newly diagnosed patients came from joint families. Skilled workers and housewives constituted the majority of patients. Approximately, one-third of indoor (36.1%) and newly diagnosed ICTC patients (34.1%) had only one child, and 41.3% inpatients and 54.5% of newly diagnosed patients had three or more dependants in their families.
The proportion of patients who revealed loss of job, selling of family assets, decreased family income, increased expenditure, and absence from work was significantly higher in the indoor than in the newly diagnosed patient with HIV/AIDS. However, school dropouts of children of PLWHAs were high in both the groups [Table 1]. The mean of previous and present per capita monthly income was Rs. 1147.09 and Rs. 529.57 respectively, and mean decrease in monthly income was 53.8 %. Mean working days lost in 1 year was 171.32 days.
Table 1.
Socioeconomic consequences of HIV/AIDS among PLWHAs
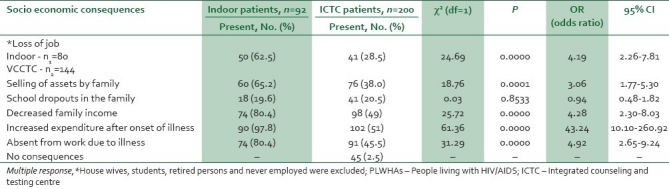
When reasons for the above-mentioned socioeconomic consequences were explored Table 2, it was found that illness was the most common reason (86.8%) for loss of job/work, followed by disclosure of sero-status to employer (13.2%). One-fifth of indoor and 4.3% of ICTC patients reported loss of work/job following disclosure of sero-status to employer. Skilled workers like drivers (22%), goldsmith (34%), jari workers (19.8%) constituted 75.8% of the total of 91 patients reporting loss of job.
Table 2.
Reasons for the Socioeconomic consequences (multiple responses)
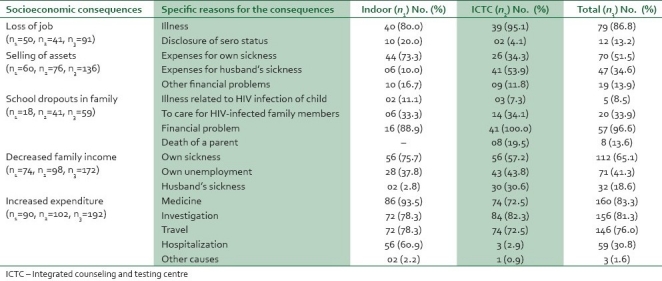
A higher proportion (73.3%) of indoor patients cited their own sickness as the main reason for selling of assets compared to ICTC patients (34.3%) and the difference was significant (z=4.94, P=0). On the other hand selling of assets to meet the expenses incurred to husband's sickness was reported by 53.9% of ICTC patients as against 10% of indoor patients yielding a significant gap in between (z=6.36, P=0).
Financial problems were accounted for in 88.9% of the school dropout children of the inpatients and 100% of outpatient participants, followed by the need to care for HIV-infected family members, almost one-third in both groups. However, 19.5% of outpatients had school dropouts due to death of a parent.
Sickness of the participants was the most common reason for decrease in family income in both groups of patients, followed by unemployment of patient and death of husband. Medicines, investigations, and travel were the major causes for increased expenditure in both the groups. Hospitalization costs were also an important factor in 60.9% indoor patients.
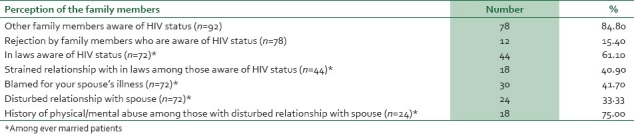
Behavior of the family members as perceived by the indoor patients was also explored [Table 3]. Among 92 indoor patients, 78 (84.8%) reported that their family members were aware of their HIV-positive status. Among them 15.4% experienced rejection by the members of their families. Overall, spouses were the major caregivers of the indoor patients (47.8%) , followed by their relatives (34.8%), and parents (15.2%). Only 2.2% of patients reported having no caregivers. Of the 72 ever married indoor patients, the in-laws were aware of HIV-positive status in 61.1% cases, and among them 40.9% patients had strained relations with their in laws. Among ever-married PLWHAs, 41.7% were blamed for their spouse's illness. Disturbed relationship with spouse was reported by 33.3% of these patients, all female, and among them, history of physical or mental abuse was present in 75% patients.
Table 3.
Effect of the disease on family relationships as perceived by indoor patients with HIV/AIDS
DISCUSSION
HIV/AIDS infects people at the peak of their productive and income generating years. Families feel its economic impact as soon as one of their members falls ill with an AIDS-related condition. A study3 undertaken by networks of PLWHAs with support from International Labour Organization (ILO) across four states of India showed that PLWHAs and their families suffered drastic income cuts by one third, compared to half, in our study. Amid rising household expenditures, families compromised on education and faced mounting debts, also corroborated in this study. A total of 38% respondents were forced to withdraw children from school in the study conducted by ILO3 and send them to work to make their ends meet compared to about one fifths of patients in the present study, supporting the observation that AIDS epidemic is changing the demand for education, as more children die of the disease, leave school to care for family members or become AIDS orphans without the means or opportunity to attend school.3
A study among PLWHAs in India3 showed that many did not disclose their sero-status to their employers fearing stigma and discrimination at the workplace. In our study, loss of job following disclosure was an important observation among in-patients, majority of whom were migrant skilled workers.
A significantly higher proportion of indoor patients cited their sickness as the main reason for selling of assets compared to newly diagnosed, as the duration and severity of their illness was more. A study in Rwanda4 among HIV-positive individuals revealed that less than 30% of households were able to meet the costs of health services exclusively from their own resources and some families paid for health care by borrowing money and selling assets. In the present study, half of the female ICTC patients were already financially affected and had to sell assets mainly due to their husband's HIV infection and subsequent illness. A study5 in Mumbai also found that economic wellbeing of the households was severely affected by AIDS. Wives experienced the maximum burden, as their spouses lost jobs and they themselves were either poorly paid or ill equipped to start earning. Women came to the hospitals mainly to take medicines for their husbands or for counseling and generally started treatment only after they become widows.5
As revealed by ILO3 , increased family expenditure in both groups of participants due to care seeking and hospitalization was also observed in this study. A study in Cote d Ivoire found that households with an HIV/AIDS patient spent twice on medical expenses as other households. Time and transportation expenses also added to the economic burden because health facilities were often located far from house.6
Spouses were the major caregivers of the indoor patients followed by their relatives. This reflects the traditional values of an Indian society where at the time of crisis, the extended family gives economic and social support - also reflected in several case studies7,8, where it was found that the responsibility of the joint family often remains even when the economic activity of the household is not joint. Even families that were predominantly nuclear seemed to turn first to and often automatically receive support from the larger family unit. Case studies8 conducted on PLWHAs of New Delhi, India, and Stockholm, Sweden, showed that Sweden had an advanced welfare system to help HIV/AIDS patients, but they lacked the primary support of their families. Although the HIV-infected people in India were not getting the similar medical benefits as in Sweden, they received a strong family support.
It was found that in overall terms, household responses to PLWHAs were supportive and positive. Even when some household members displayed a rejecting attitude, the households did not abandon a member with HIV. However, the household response differed by gender and by relationship status, and was similar to the findings in other studies.5 Household responses could be better understood by paying close attention to the history of past relationships between the HIV-positive person and the caregivers. A previous history of disturbed relationships – physical violence, emotional and economic neglect, mistrust and suspicion between partners – influenced attitudes and feelings with which care was provided.
CONCLUSION
The socio-economic impact of HIV/AIDS was considerably grave, and certainly more among the sicker patients with increased severity and duration of the disease. Intensive education for PLWHAs, their family members, and other stakeholders is urgently required for the reduction of AIDS-related stigma and discrimination, as also the need for care and support. More research to get a better insight into the problem of socio-economic impact at household and community levels, and for mainstreaming of PLWHAs is the need of the hour. Services to support those affected as well as a legal framework to protect their rights is also important.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Population, reproductive rights and reproductive health with special reference to HIV/AIDS – A concise report, United Nations. New York: Department of Economic and Social affairs, Population Division. 2004. [Accessed on 24.01.2008]. Available from: http://www.amazon.com/Population-Reproductive-Rights-Special-Reference/dp/sitb-next/9211513731 .
- 2.Sexual health exchange. [Last accessed on 2006, Jan24]. Available from: http:// www.kit.nl/exchange2003/1: 15-6 .
- 3.ILO project – Assigning the socio economic impact of HIV/AIDS on PLWHAS and their families in India – undertaken. [Last accessed on 2006 Jan 24]. Available from: http://www.ilo.org .
- 4.Nandakumar AK, Schreider P, Butera D, Pitayanom S, Kongslin S, Wattana S. Use and expenditures on out patient health care by a sample of HIV positive individuals in Rwanda. Paper presented at the International AIDS Economic Network (IAEN) Symposium on the economics of AIDS. Durban, South Africa; 2000. Population Bulletin. 2002;57:22. [Google Scholar]
- 5.Bharat S. Facing the challenge household and community response to HIV/AIDS in Mumbai, India (Executive Summary) In: Agarwal OP, Sharma AK, Indrayan A, editors. HIV/AIDS Research in India. New Delhi: National AIDS Control Organization, Ministry of Health and Family Welfar; 1997. pp. 372–5. [Google Scholar]
- 6.Lamptey P, Wigley M, Carr D, Colly MY. Facing the HIV/AIDS pandemic. Popul Bull. 2002;57:20–1. [Google Scholar]
- 7.Basu A, Gupta D, Krishna G. “The household impact of adult morbidity and mortality: Some implications of the potential epidemic of AIDS in India,” in the economics of HIV and AIDS. In: Bloom DE, Godwin P, editors. New Delhi: Oxford University Press; 1997. [Google Scholar]
- 8.Kaur H, Kar HK. Psycho-social cultural aspects of HIV/AIDS in India and Sweden: A comparative study. In: Agarwal OP, Sharma AK, Indrayan A, editors. HIV/AIDS research in India. New Delhi: National AIDS Control Organization, Ministry of Health and Family Welfare; 1997. pp. 473–9. [Google Scholar]