

Abstract
Background:
Elective caesarean sections have been considered safer for both mother and the fetus compared to their emergency counterpart. However, emergency caesarean sections have continued to form bulk of caesarean deliveries in our facility.
Objective:
The objective of this study was to determine the caesarean section rate together with the trend, indications, and maternal mortality associated with elective caesarean operation.
Materials and Methods:
A retrospective analysis of clinical records of all the patients that had caesarean section between January 2002 and December 2010 (9 years) at Usmanu Danfodiyo University Teaching Hospital (UDUTH) Sokoto, Nigeria was conducted.
Results:
During the 9 year study period, 2284 caesarean sections were performed out of 22,985 total deliveries at UDUTH Sokoto, thus giving a caesarean section rate of 9.9%. Emergency and elective operations accounted for 1784 (78.2%) and 498 (21.8%) of the cases respectively. The rate of elective caesarean section increased from 1.7% in 2002 to 3.2% in 2007. Thereafter it declined gradually to 1.8% in 2010. Repeat caesarean section (30.7%) and malpresentation (17.1%) were the most common indications for elective caesarean operation. There were 18 maternal deaths from caesarean section and only one from the elective caesarean procedure.
Conclusion:
The rising trend in the elective caesarean section rate in this study underscores the need for better and improved patient selection together with counseling on its benefits and risks. This is because despite the fact that it is safer than emergency caesarean operation, it is not entirely devoid of complications. Routine use of spinal anesthesia in performing the procedure should be encouraged.
Keywords: Elective caesarean section, sokoto, Nigeria
INTRODUCTION
Caesarean section is the delivery of the fetus, placenta, and membranes after the age of viability through an abdominal and uterine incision.1 There is a wide global variation in the incidence of caesarean section. The general range is from 5% to 25% with a continued rise in developed countries while in developing countries the rate is relatively low.1,2 In Nigeria, the rate of caesarean section varies from one center to the other with 10.3% in Enugu,3 10.5% (Makurdi),4 11.4% (Zaria),5 15.8% (Jos),6 and 20.3% in Birnin-Kebbi7 having been reported. The increase in caesarean section rates is largely driven by several factors which include societal demands for improved fetal outcome, protection of pelvic floor, and the aspiration of obstetricians to meet these demand.8
Caesarean section can be performed either as an elective or emergency procedure. The former constitutes bulk of the cases.3–6 The indications for elective caesarean section are many and varying and are often relative rather than absolute. They include contracted pelvis, major degree placenta previa, two or more previous caesarean section, malpresentation, HIV infection in pregnancy, previous vesico-vaginal fistula repair, intrauterine growth restriction, and bad obstetric history.1,4,6,9
Usmanu Danfodiyo University Teaching Hospital (UDUTH) Sokoto, a 500 bed tertiary health center, serves Sokoto, Kebbi, and Zamfara states in Nigeria and also receives patients from the neighboring Niger Republic. The population served is mainly the Hausa/Fulani ethnic group and of Islamic faith. The main occupation of the men is subsistence farming and animal husbandry. Patients are booked for antenatal care based on both hospital and self-referral. It is an area where early marriage of girls is prevalent. Girls are often married before the age of menarche thus making adolescent pregnancies and their associated complications common finding in the area.8 Some of the complications of adolescent childbirth (cephalopelvic disproportion with associated caesarean delivery and vesico vaginal fistula) often necessitate elective caesarean section in subsequent pregnancies.10,11 Paucity of data in the literature on elective caesarean section in Sokoto, North Western Nigeria informed this study.
MATERIALS AND METHODS
This was a retrospective analysis of 2284 consecutive caesarean sections performed at UDUTH Sokoto over 9 years (January 2002 to December 2010). The records from the labor room and operating theater were retrieved and checked for caesarean deliveries. The delivery records of patients that had elective caesarean sections were obtained and relevant variables extracted. The variables include age, type of caesarean section, its indication, type of anesthesia used, and the maternal outcome. The data were analyzed using simple percentages.
RESULTS
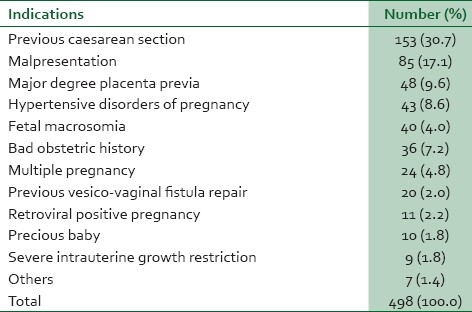
There were 22,985 total deliveries at the facility out of which 2284 were caesarean sections giving a caesarean section rate of 9.9%. A total of 1784 patients (79.3%) had emergency caesarean section while 498 patients (21.8%) had an elective procedure. General and spinal anesthesia were used in 253 (53.6%) and 219 (46.4%) of cases respectively. The age of the patients ranged from 18 years to 44 years with a mean of 31.2±3.6 years. The modal age for elective caesarean section was 30-34 years. Table 1 shows the annual distribution of total, emergency, and elective caesarean section. It demonstrates a gradual rise in the rate of elective caesarean section increasing from 1.7% in 2002 to 3.2% in 2007. However the rate declined to 1.8% in 2010. Table 2 depicts the indications for elective caesarean section. Repeat caesarean section for two or more previous caesarean section (31.1%) and malpresentation (18.4%) were the most common indication for elective caesarean operation. There were 18 maternal deaths from caesarean section and one from the elective caesarean procedure while the rest from emergency caesarean section. The cause of that single death from the former was anaphylactic reaction to general anesthetic agent.
Table 1.
Annual distribution of total, emergency, and elective caesarean section
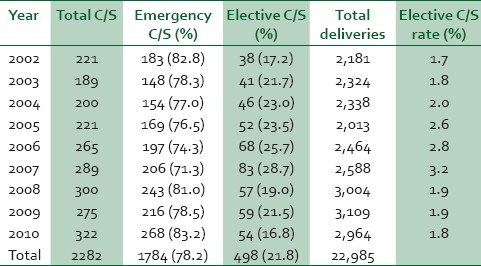
Table 2.
Indications for elective caesarean section
DISCUSSION
The caesarean section rate of 9.9% in this study is within the range of 6.4-32.1% reported in Nigeria by previous authors.3–7,12–14 However, the proportion elective caesarean section (20.7%) relative to its emergency counterpart in the present study is much higher than 5.8-16.4% reported in most centers in the country.4,6,7 This may be attributed to relatively high rate of cephalo-pelvic disproportion arising from early marriage and teenage pregnancy in the study area10 which would have necessitated two previous emergency caesarean deliveries followed by the elective caesarean procedure. In addition, high rate of vesico-vaginal fistula from prolonged obstructed labor in the study zone15 may be contributory. This is because when the fistula is successfully repaired, subsequent deliveries are usually by elective caesarean operation.16
The rising trend of elective caesarean in these data has similarly been observed by previous authors.4–6 The reason for this may be the ever increasing list of the indications of elective caesarean delivery, larger cohort of patients with two or more previous caesarean section, and improved patient selection by clinicians with the use of better diagnostic techniques such as ultrasound machine.5 The most common indication in this study, repeat caesarean section, has also been reported in previous studies.4,6,13 However, the second leading indication for the procedure in these data, malpresentation, is in contrast to bad obstetric history and HIV infection in pregnancy reported in Jos and Makurdi respectivelty.4,6
In conclusion, the rising trend of elective caesarean section observed in this study, underscores the need to better and improved patient selection together with counseling on its benefits and risks as elective caesarean operation though safer than its emergency counterpart is not entirely free of morbidity or mortality to both the mother and the baby. In addition routine use of spinal anesthesia in performing the procedure should be encouraged.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Incerpi MH. Operative delivery. In: Decherney AH, Nathan L, Goodwin TM, Laufer N, editors. Current diagnosis and treatment obstetrics and gynaecology. New York: Mc Graw Hill; 2007. pp. 461–76. [Google Scholar]
- 2.Jaiyesinmi RA, Ojo O. Caesarean section. In: Okonofua F, Odunsi K, editors. Contemporary obstetrics and gynaecology for developing countries. Benin City: Women's Health and Action Research Centre; 2003. pp. 592–621. [Google Scholar]
- 3.Megafu U, Nweke PC. Maternal mortality from caesarean section. Trop J Obstet Gynaecol. 1991;9:1–4. [PubMed] [Google Scholar]
- 4.Swende TZ, Agida ET, Jogo AA. Elective caesarean section at the Federal Medical Centre Makurdi, north-central Nigeria. Niger J Med. 2007;16:372–4. [PubMed] [Google Scholar]
- 5.Sule ST, Matawal BI. Comparisons of indications for caesarean section in Zaria, Nigeria: 1855 and 1995. Ann Afr Med. 2003;2:77–9. [Google Scholar]
- 6.Mutihir JT, Daru PH, Ujah IO. Elective caesarean section at Jos University Teaching Hospital. Trop J Obstet Gynaecol. 2005;22:39–41. [Google Scholar]
- 7.Nwobodo EI, Wara HL. High caesarean section rate at Federal Medical Centre Birnin-Kebbi: Real or apparent? Niger Med Pract. 2004;46:39–40. [Google Scholar]
- 8.Shehu DJ. Socio-cultural factors in the causation of maternal morbidity and mortality in Sokoto. In: Kisekka M, editor. Women's Health Issues in Nigeria. Zaria: Tamaza Publishing Company Limited; 1992. pp. 203–14. [Google Scholar]
- 9.Swende TZ. Emergency caesarean section in a Nigerian tertiary health centre. Niger J Med. 2008;17:396–8. doi: 10.4314/njm.v17i4.37419. [DOI] [PubMed] [Google Scholar]
- 10.Nwobodo EI, Adoke KU. Obstetric outcome of teenage pregnancies at a tertiary hospital in Sokoto, Nigeria. Trop J Obstet Gynaecol. 2005;22:168–70. [Google Scholar]
- 11.Ante M. Adolescent fertility: Panoramic view of problems. Niger Med Pract. 1993;25:3–9. [Google Scholar]
- 12.Oye-Adeniran BA. Recent trends in caesarean section at University Teaching Hospital Lagos, Nigeria. Nig Q J Hosp Med. 1998;8:111–4. [Google Scholar]
- 13.Okonta PI, Otodie VO, Okogbenin SA. Caesarean section at University of Benin Teaching Hospital revisited. Trop J Obstet Gynaecol. 2003;20:63–6. [Google Scholar]
- 14.Adinma JI. Caesarean section: A review from sub-Saharan hospital in Nigeria. Niger Med J. 1993;24:9–12. [Google Scholar]
- 15.Ghatak DP. A study of urinary fistula in Sokoto, Nigeria. Indian Med Assoc. 1992;90:285–7. [PubMed] [Google Scholar]
- 16.Sadauki HM. Operative deliveries. In: Ikpeze OC, editor. Fundamental of Obstetrics and Gynaecolgy. Onitsha: Africana First Publishers PLC; 2009. pp. 140–9. [Google Scholar]