

Abstract
Endoscopic submucosal dissection (ESD) is now the most common endoscopic treatment in Japan for intramucosal gastrointestinal neoplasms (non-metastatic). ESD is an invasive endoscopic surgical procedure, requiring extensive knowledge, skill, and specialized equipment. ESD starts with evaluation of the lesion, as accurate assessment of the depth and margin of the lesion is essential. The devices and strategies used in ESD vary, depending on the nature of the lesion. Prior to the procedure, the operator must be knowledgeable about the treatment strategy(ies), the device(s) to use, the electrocautery machine settings, the substances to inject, and other aspects. In addition, the operator must be able to manage complications, should they arise, including immediate recognition of the complication(s) and its treatment. Finally, in case the ESD treatment is not successful, the operator should be prepared to apply alternative treatments. Thus, adequate knowledge and training are essential to successfully perform ESD.
Keywords: Attachments, Complication, Endoscope, Electrosurgical unit, Endoscopic submucosal dissection, Endoscopic submucosal dissection device, Injection agent, Sedation, Training
INTRODUCTION
Endoscopic submucosal dissection (ESD) is now a well-known procedure for the treatment of superficial neoplasms in the gastrointestinal tract. Use of gastric ESD with an insulation-tipped diathermic knife (IT knife) was first reported in the literature by Hosokawa and Yoshida[1] in 1998, with the first English language report of rectal ESD published by Gotoda et al[2] in 1999. Earlier, in 1988, Hirao et al[3] reported a novel endoscopic therapeutic procedure to remove a superficial gastric tumor with a needle knife and local injection of hypertonic saline-epinephrine solution (ERHSE), which is considered the first usage of ESD. These methods were developed to provide patients with a minimally-invasive procedure and to prevent overtreatment.
Initially, for small intramucosal gastric cancer, the possibility of lymph node metastases was estimated to be less than 3% (but not zero)[1]. In 2000, Gotoda et al[4] analyzed 5265 patients who had undergone gastrectomy with lymph node dissection for early gastric cancer, and found that none of the 1230 well-differentiated intramucosal cancers less than 30 mm diameter were associated with nodal metastases regardless of ulceration findings. Moreover, of 929 well-differentiated intramucosal cancers without ulceration, none were associated with nodal metastases. These findings provided the basis for the indication of ESD to treat intraepithelial gastric cancer. Detailed indications in each organ for the application of ESD will be discussed in other articles in this issue.
Endoscopic mucosal resection (EMR) is still a mainstay for the treatment of gastrointestinal intramucosal tumors. The alternate ESD requires an extensive knowledge base and a high skill level, obtained only through adequate training and experience. Moreover, ESD is a more time-intensive procedure with a higher incidence of complications, as compared to EMR. So, why should ESD be chosen instead of EMR? A direct comparison of EMR and ESD (Table 1) clearly reveals the answer: ESD provides a higher rate of complete en-bloc resection which results in higher curative resection and a lower recurrence rate[5-9]. In addition, a meta-analysis revealed that ESD shows better en bloc and curative resection rates and decreased local recurrence compared with EMR[10].
Table 1.
Comparison between endoscopic mucosal resection and endoscopic submucosal dissection
| Method | Total cases | En-bloc resection (%) | Complete resection (%) | Complication (%) | Year1 | Reference | |||
| Bleeding | Perforation | Stenosis | |||||||
| Esophagus | ESD | 31 | 100 | 97 | - | 3 | - | 2008 | Ishihara et al[5] |
| EMRC | 68 | 87 | 71 | 1.4 | - | 4.4 | 2008 | Ishihara et al[5] | |
| EMR-2channel | 72 | 71 | 46 | - | - | - | 2008 | Ishihara et al[5] | |
| Stomach | ESD | 195 | 83 | 83 | 3.9 | 9.7 | - | 2006 | Oka et al[6] |
| EMR | 825 | 42 | 23.6 | 6.2 | 0.5 | - | 2006 | Oka et al[6] | |
| ESD | 243 | 95.9 | 93 | 5.3 | 4.5 | - | 2009 | Min et al[7] | |
| EMR-precut | 103 | 77.7 | 89.3 | 3.9 | 1.9 | - | 2009 | Min et al[7] | |
| ESD | 303 | 92.7 | 73.6 | - | 3.6 | - | 2006 | Oka et al[8] | |
| EMR | 411 | 56 | 61.1 | - | 2.2 | - | 2006 | Oka et al[6] | |
| Colon (over 2 cm) | ESD | 145 | 84 | 98 | 1.4 | 6.2 | - | 2010 | Saito et al[9] |
| EMR | 228 | 33 | 86 | 3.1 | 1.3 | - | 2010 | Saito et al[9] | |
Year of paper publication. -: Not mentioned in the article; ESD: Endoscopic submucosal dissection; EMRC: Endoscopic mucosal resection using a transparent cap; EMR-2channel: 2-channel endoscopic mucosal resection; EMR-precut: Endoscopic mucosal resection after circumferential precutting.
In this article, the basic knowledge required before starting ESD is described, such as the endoscope, electrosurgical unit, ESD devices, injection agents, sedation, complications, and training.
ENDOSCOPE
The ESD procedure can be performed with regular endoscopes, but therapeutic endoscopes offer additional utility and functionality, as described below.
Waterjet function
Bleeding is a common complication in ESD that often occurs during the procedure. When this happens, it is helpful to apply water onto the bleeding site: the water can clean away blood and blood clots easily and identify the precise bleeding point, facilitating immediate intervention for hemostasis. All endoscope manufacturers offer endoscopes with a waterjet feature (GIF-Q260J and GIF-1TQ160 from Olympus, EG-450RD5 from Fujifilm and EG29-i10N and EG-2990K from Pentax).
Large diameter channel
Most ESD knives can fit in the regular channel, which is 2.8 mm in diameter. However, during the procedure, air, water or blood must be suctioned; thus, an endoscope with a larger channel is more suited for ESD procedures. Most therapeutic endoscopes, such as those mentioned above, are equipped with a larger 3.2 mm diameter channel. Another endoscope choice is one with a dual channel (GIF-2T240 or GIF-2T160 from Olympus and EG-450D5 from Fujifilm). This type of scope offers two advantages. First, a second device, such as grasping forceps or an injection needle, can be used concurrently, which saves the time required to change devices. Second, it may facilitate an easier approach to the lesion. For instance, if the operator needs to cut or dissect on the right side, it may be more difficult with a regular endoscope, which has its working channel on the left side. Thus, if the device can be applied from the right side, the procedure will be easier and faster.
Flexibility
The flexibility of most current endoscopes is sufficient to perform ESD. For colorectal ESD, an esophagogastroduodenoscopy (EGD) endoscope may be useful because it is easy to switch to a retroflex view in the narrow space. In the stomach, it is sometimes difficult to approach the lesions, especially in the “angle” or lower body of the stomach. One option is to use a multi-bending endoscope (GIF-2TQ260). This scope also has two channels, a useful feature for ESD.
Useful attachments
The use of specialized attachments can broaden the functionality of existing endoscopes and enable a wider range of ESD procedures. This is especially advantageous if budget constraints preclude the purchase of new endoscopes.
During ESD procedures, particularly for those involving a dissecting step, a transparent distal attachment (hood/cap) can be mounted at the tip of the endoscope to maintain a clearer view of the dissecting area. The hood pushes the resected mucosa against the submucosa (counter traction) allowing a better view. An endoscopic hood/cap is useful in preventing extraneous folds from being in the surgical field, and is indispensable for ESD. Various other types of attachments can be chosen depending on the needs or situation (e.g., an attachment with holes to drain water or blood). Needless to say, it is necessary to keep a clear view and determine the correct margin of the lesion to perform the precise ESD procedure. Failure to attain adequate margins with ESD may mandate surgery.
The type KUME hood (Create Medic, Yokohama, Japan) is a soft transparent distal attachment with a thin tube (Figure 1A). When mounted on the tip of the endoscope, this hood can provide a waterjet via the tube attached to a water-filled syringe. A related device (Kume cap-knife attachment, Create Medic, Yokohama, Japan) uses a fixed snare to facilitate ESD[11].
Figure 1.
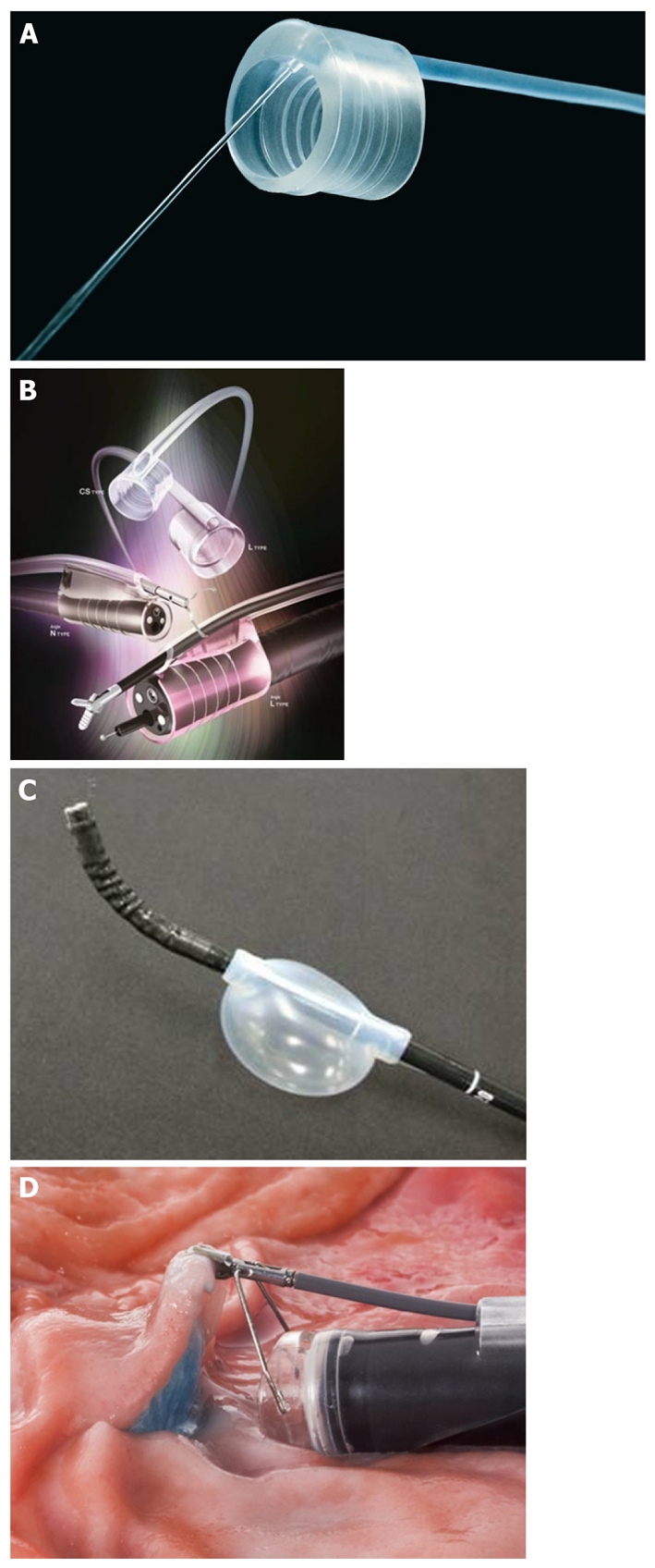
Attachments for endoscopes that broaden their functionality. A: Type Kume hood; B: Impact shooter; C: Air assist; D: Endo lifter.
Impact Shooter (Top Co., Tokyo, Japan) is another transparent distal attachment with a tube (Figure 1B). Having a tube of diameter 2.8 mm, it is designed for devices such as ESD knives, and also enables the endoscope to work like a dual channel scope. The disadvantage is its small diameter; it requires an overtube with a larger diameter.
Air Assist (Top Co., Tokyo, Japan) is a soft balloon that fits outside the endoscope, proximal to the bending area of the endoscope (Figure 1C). This device enables the endoscope to mimic a multi-bending scope. When the balloon is inflated with air (up to 200 cc) in the gastric lumen, the scope will be pushed by the balloon against the gastric wall, enabling the scope to approach close to the lesion.
The Endo Lifter (Olympus, Tokyo, Japan) is a distal attachment with grasping forceps, which can be used to grasp the mucosa (Figure 1D). Once the proximal area is cut and the mucosa grasped with the Endo Lifter, the submucosal layer is revealed, enabling easy and safe dissection of the submucosa.
Carbon dioxide insufflation
Insufflation with carbon dioxide (instead of air) is popular in endoscopy/colonoscopy to reduce patient postprocedural pain[12,13]. Recently, carbon dioxide insufflation has also been reported to be useful for ESD[14], allowing the use of fewer sedative medications and possibly reducing complications, such as compartment syndrome following perforation during ESD. Nonaka et al[15] reported the safety of carbon dioxide insufflation for upper gastrointestinal ESD cases.
ELECTROSURGICAL UNIT
A high performance ESU is indispensable for a successful ESD procedure. An ESU instrument passes high-frequency electric currents through tissue to accomplish a particular surgical effect. The ESU is required for every step of an ESD procedure: marking, pre-cutting, circumferential cutting, submucosal dissection and hemostasis. Older ESUs only had one power setting, but the ICC series ESU (ICC 200, ICC 300, ICC 350, ERBE, Tuebingen, Germany) is unique in that it has a sensor that can control the power automatically and adjust to the circumstance[16]. Each instrument can detect the current, the power voltage and the spark, and can then generate a certain amount of voltage. Therefore, the procedure can be performed in a smooth and steady manner. There are various kinds of electric modes, each of which is used for a different purpose (Figure 2). A steady cut is made with the “Auto cut” mode, where power dosing is automated (software controlled) with constant voltage. The “Endo cut” mode provides both cut and coagulation effects, which is effective for hemostasis during the cut procedure. The “Forced coag” mode generates a high voltage and is suitable for submucosal dissection. Due to the high voltage, a cutting effect is also obtained with the coagulation effect. For hemostasis, the “Soft coag” mode is effective. Since the maximum voltage is limited to 200 volts in this mode, the coagulation effect does not penetrate to deeper areas.
Figure 2.

The various electric modes that are offered by ICC and VIO electrosurgical unit instruments and their function.
The VIO series (VIO 300D, VIO 200D, VIO 200S, ERBE, Tuebingen, Germany) are advanced models of the ICC series. Since the maximum current of a VIO series machine is twice that of the ICC series, it can generate more power. Also, some new modes are provided: Dry cut™, Swift coag™ and Spray coag™. The “Dry cut” mode provides both higher power for coagulation and cutting, so the lesion can be cut faster and more coagulation (hemostasis) is also obtained. The “Dry cut” mode is often said to be difficult to handle for beginners. The “Swift coag” mode is similar to the “Dry cut” mode: it provides a higher voltage and less current, providing a smaller cutting effect and a larger hemostatic effect. The “Spray coag” mode gives non-contact surface coagulation, with low penetration depth. It is useful for post-procedural hemostasis of a broad area. The various electric modes that can be used with the ICC and VIO are shown in Figure 2.
ESD DEVICES
A large variety of ESD devices have now been developed and launched by several companies. In the past, these devices were divided into two groups: uncovered type devices and covered devices. However, recently, a third group of ESD devices were launched: forceps devices (Table 2).
Table 2.
Characteristics of each endoscopic submucosal dissection device
| Device | Marking | Pre-cut | Cut | Dissection | Hemostasis | Fibrosis | Beginner use | Figure |
| Needle Knife | O | O | O | O | O | × | Figure 3A | |
| Flex Knife | O | O | O | O | Figure 3B | |||
| Hook Knife | O | O | O | O | O | × | Figure 3C | |
| Triangle Tip Knife | O | O | O | O | Figure 3D | |||
| Dual Knife | O | O | O | O | Figure 3E | |||
| Flush Knife BT | O | O | O | O | Figure 3F | |||
| IT Knife 2 | × | × | O | O | Figure 3G | |||
| Mucosectome 2 | × | × | O | O | Figure 3H | |||
| Swanblade | O | O | Figure 3I | |||||
| SB Knife | O | O | O | O | Figure 3J | |||
| Clutch Cutter | O | O | O | O | O | O | O | Figure 3K |
O: Suitable; ×: Not recommended; Blank: Not ideal but can be used.
Uncovered devices
Uncovered devices have nibs on the edges of the tips. The shape of the nib varies from device to device and characterizes each device. The advantage of an uncovered device is that it can perform nearly all of the steps of an ESD procedure, except for hemostasis. The disadvantage is that it requires a high skill level to handle. If not used carefully, the nibs can produce complications, such as bleeding and perforation. Also, moving the knife too rapidly can result in inadequate coagulation during cutting or dissecting, and result in bleeding. Moreover, perforation can occur if the knife cuts too deeply, which can occur when visualization is poor.
Needle Knife (KD-1L-1, Olympus, Tokyo)
Although not originally developed for ESD, the needle knife is very useful for this procedure. It is applicable in every step of ESD, and is useful in cases with accompanying fibrosis. The most significant advantage of this device, compared to other devices, is reusability: this is the only reusable ESD device (owing to its durability during sterilization). As the tip of this needle knife is sharp and non-covered, it is easy to inadvertently perforate the tissue. Thus, this device requires care in maneuvering and is most suitable for expert ESD operators[17] (Figure 3A).
Figure 3.

Endoscopic submucosal dissection devices. A: Needle Knife; B: Flex Knife; C: Hook Knife; D: Triangle Tip Knife; E: Dual Knife; F: Flush Knife BT; G: IT Knife 2; H: Mucosectome 2; I: Swan blade; J: SB Knife; K: Clutch cutter; L: Coagrasper.
Flex Knife (KD-630L, Olympus, Tokyo)
This knife has a thin snare-like tip and is useful for all ESD steps: marking, cutting, and dissection. It has a barb on the tip of the sheath, to prevent unnecessary deep insertion of the knife into the submucosa. The lower price (almost half that of other devices) is another signature feature of this device[18,19] (Figure 3B).
Hook Knife (KD-620LR/KD-620QR, Olympus, Tokyo)
This knife is similar to the needle knife, but with a tip that is bent at a right angle and rotatable, and is also usable for all ESD steps. The angle enables not only cutting of the lesion but also hooking the lesion, even fibrotic lesions. When the lesion is expected to be fibrotic, this device should be used, in combination with other devices. Like the needle knife, it is a thin knife, requiring skillful maneuvering[20] (Figure 3C).
Triangle Tip Knife (KD-640L, Olympus, Tokyo)
This knife has a small triangular plate at the tip, and is like the IT knife 2 (without the insulation; see below). The small triangular-shaped tip enables it to make markings and also to hook the mucosa and the submucosa, making it is usable during all ESD steps[21] (Figure 3D).
Dual Knife (KD-650L/KD-650Q, colon, Olympus, Tokyo)
This knife has a small ball-like process on the top, which prevents it from slipping (unlike the Needle Knife). When the tip is retracted, only 0.3 mm of the ball-like process protrudes, so it is easy to make markings on the lesion. The thicker end of the sheath prevents inadvertent tissue perforation (Figure 3E).
Flush Knife BT/ Flush Knife (DK2618JB/DK2618JN, Fujifilm, Saitama)
The difference between Flush Knife BT and Flush Knife is the ball-like process (ball tip) on the edge. This ball-like process enables hooking of the lesion and makes the ESD procedure easier. Flush Knife BT is like the Dual Knife, but unique due to a waterjet channel. Since the waterjet channel is mounted inside the knife sheath in the same direction as the knife, the waterjet is emitted in the same direction toward the lesion. It is useful for washing the lesion or hemostasis, and sometimes, for submucosal injection during the dissection. This knife is useful in facilities lacking scopes with waterjets. Flush Knife BT has a product line from 1.5 mm to 30 mm in length (while the Flush Knife goes from 1.0 mm to 30 mm). For esophageal or colorectal ESD, a 1.5 mm or 2.0 mm length may be safer and useful, whereas for gastric ESD, a 25 mm knife is more suitable[22-24]. The Splash Needle (DN-2718A, Pentax, Tokyo) is like the Flush Knife, but only comes in a length of 2.5 mm (Figure 3F).
Covered devices
Covered devices have a blade which is covered with insulated material, such as a ceramic tip, or sheath to prevent perforation. The original covered device was the IT knife, with a variety of covered devices now available.
IT knife/ IT knife 2 (KD-610L/KD-611L, Olympus, Tokyo)
The IT knife was the first device developed for ESD, and this device was instrumental in promoting the usage of ESD among endoscopists, due to its ease of handling (compared to the Needle Knife). An insulated ceramic tip is mounted on the tip of this device to prevent unnecessary perforation. IT knife 2 is an improved version of IT knife, with a small metallic plate mounted inside the ceramic tip, facilitating procedures in the traverse direction. During the cutting process, it is sometimes difficult to see the cutting point, because the lesion is on the side, not on the tip, but trying to adjust the position constantly and maintaining a good view during the procedure is important to avoid errors. A critical procedural aspect is to not push the knife toward the lesion while cutting (which can result in perforation), but instead, cut the lesion in a “pulling” manner, which is safer[1,2,25,26] (Figure 3G).
Mucosectome 2 (DP-D2518/DP-D2622, Pentax, Tokyo)
Mucosectome 2, a unique device, was developed with the concept of safety in mind, i.e., to prevent perforations. This knife has a 5 mm rotatable blade on one side of the sheath and can only cut in one direction, creating a safer ESD device. Consequently, it can be used only for dissection and not for marking or cutting. Because of its design (where the blade is on one side of the round sheath rather than on the sheath tip), the dissection depth can be rather shallow, and procedures can take longer[27] (Figure 3H).
Swanblade (DC-D2618, Pentax, Tokyo)
This knife has a round, snare-like rotatable tip on one side of the sheath. The concept behind this knife design is the same as that of the Mucosactome 2: namely, safety. Although it was designed for dissection, it can still be used for marking. With the smaller blade embedded in one side of the sheath, it is a safe device but may require a longer procedure time (Figure 3I).
Forceps devices
Forceps devices are brand-new tools in the field of ESD. They were developed with a point-of-view different from the other types of devices: to grasp and cut, instead of just cut, as with the knives. The first advantage of these devices is safety: the operator can more readily see the lesion before cutting or dissecting. Also, as the lesion can be better viewed, cutting can be stopped should the cutting point be incorrect or complications arise. The second advantage is that other devices, such as hemostasis forceps, are not needed. Thus, this kind of device is suitable for beginners. Of course, the procedure time is longer because it always requires two steps: grasp then cut.
SB knife and SB knife Jr. (MD-47706/MD-47704 and MD-47703, Sumitomo Bakelite, Akita)
These forceps have a claw and curved scissors to prevent unnecessary injury of the normal muscle layer. The SB knife line includes the following: standard type (7 mm knife), short type (6 mm knife) and thin type (SB knife Jr.; 3.5 mm knife). The use of specially designed transparent hoods (SB hoods) is recommended[28] (Figure 3J).
Clutch Cutter (DP2618DT, Fujifilm, Saitama)
The characteristic feature of this forceps device is the rotatable, serrated cutting edge, which enables the endoscopist to grasp the lesion securely and properly. The serrated edge furnishes a firm grip that does not easily slip off the lesion. An all-in-one device, the Clutch Cutter, can be applied for every step of the ESD procedure: marking, cutting, dissection, and also hemostasis. With this device, the ESD strategy is simple: grasp and cut what is directly in view. It is easy to handle and safe and, hence, appropriate for beginners[29-31] (Figure 3K).
Other devices
Other devices for ESD are being used, but these are not yet available in Japan; thus, we have no practical experience with them. Some are described below: (1) The Fork knife (Kachu Technology, Seoul) is a unique device, which has two interchangeable knives: a fixed flexible snare and a forked knife. It also has a waterjet feature[32]; (2) The Hybrid knife (ERBE, Tuebingen) has an ultrafine, high-pressure fluid jet with an electrocautery needle (like the Flush knife or Splash needle)[33]; and (3) The Flexible Maryland dissector (Ethicon Endo-Surgery, Cincinnati, USA) was developed from the laparoscopic Maryland dissector[34]. It is a forceps device (like the Clutch Cutter).
INJECTION AGENTS
For EMR, the injection agent is used to lift the lesion up to prevent complications such as perforation or bleeding. Similarly, for the safe and accurate performance of ESD, the submucosal injection plays an even more important role: to expose and hold steady the cutting point. Hence, the correct choice of injection agent is a key to successful ESD. More specifically, injection of the correct agent provides clearer visualization of the lesion, and makes the cutting and dissection process easier and safer. Because the ESD procedure generally takes longer than the EMR procedure, a long-lasting agent is needed for ESD. At the same time, the agent must be safe, easy to handle, and easy to inject.
Normal saline (NS) is the most popular injection agent for EMR. It is inexpensive and easy to inject into the submucosa. Although NS has also been used for ESD in some situations, it has a major disadvantage: it is not a long-lasting cushion when injected into the submucosa. To overcome this issue, a large variety of injection agents have been evaluated[35-37]. Hypertonic saline solution and dextrose are inexpensive and readily available, but both can cause tissue damage[38]. Likewise, hydroxypropyl methylcellulose can damage tissue. On the other hand, fibrinogen is a good submucosal cushion[39]; but, since this agent is derived from human serum, it has been criticized as a potential vehicle for viral transmission. Further investigations to address this issue are expected. Sodium carboxymethylcellulose[40], endoscopic lubricant jelly (Null Jelly)[41] and photocrosslinkable chitosan hydrogel[42] may be other choices, but further study is necessary to verify the safety and efficacy of these alternatives.
As a submucosal injection agent, glycerol (also called glycerin; Chugai Pharmaceutical, Tokyo) has been widely used for EMR[43]. This inexpensive agent (commercially available as 10% glycerin and 5% fructose in NS) was originally used for the treatment of brain edema, and is also useful for ESD, but a more viscous agent is desirable for ESD to maintain a good visual field. Sodium hyaluronate was firstly described as a submucosal injection agent by Yamamoto et al[44] in 1999. Although expensive, this substance produces a good, long-lasting cushion in the submucosa, even in the colon[45]. A ready-to-use commercial product is available in Japan (Mucoup, Johnson and Johnson, Tokyo), which can be used undiluted or diluted with glycerol or NS; and, sodium hyaluronate is now a standard injection substance for ESD in Japan.
Other agents to mix
Epinephrine (when added to a submucosal injection agent, such as sodium hyaluronate or glycerol) has been reported to reduce immediate bleeding during the endoscopic procedure[46-48]. However, due to the limited clinical evidence, its use may not be warranted. [When used, 0.05 cc to 0.1 cc of diluted epinephrine (0.001%) is mixed into 20 cc of the submucosal injection agent].
Indigo carmine may also be added to the injection solution to help visualize the area to cut or dissect. This blue dye visualizes the submucosa where the solution is injected, which helps prevent inadvertent cutting of the normal muscle layer that can lead to perforation. As the dye can excessively darken the area, some endoscopists avoid using it. For ESD submucosal injection, a 0.004% dye concentration in the injection solution is suitable.
Another chemical added to submucosal injection solutions is lidocaine (1%), which has been used as a local anesthesia, especially for rectal ESD close to the dental line[49].
Future injection agent
Sumiyama et al[50,51] reported a novel ESD procedure using mesna (sodium 2-mercaptoethanesulfonate). Mesna is a mucolytic agent which cleaves disulfide bonds in connective tissue between anatomical planes. Once the lesion has been circumferentially isolated, mesna is injected into the submucosal layer, and the region to be dissected is held with the tip of a cap-fitted endoscope. There is rarely a need to dissect the submucosa with electrocautery and minimal concern about perforation with knifes. If this innovative procedure proves to be safe, it may change ESD itself: ESD will not be limited to highly-skilled surgical craftsmen anymore, and thus, may be practiced universally.
SEDATION
Most of the diagnostic endoscopies are performed without any sedation in Japan. In contrast, almost all endoscopic procedures are performed with sedation in the United States, even for diagnostic examination. In the United States, patients usually receive conscious sedation during the procedure, with benzodiazepines combined with opioids the most frequently used (e.g., midazolam with fentanyl or pethidine).
Because of the longer procedure time for ESD (vs EMR), it is very important to sedate the patient throughout the procedure (to minimize patient discomfort and anxiety). Patients need to be well sedated for ESD, and thus changes in their behavior should not be relied upon to consider the possibility of complications. For most interventional cases, conscious sedation is also provided. If sedation cannot be used for whatever reason, the patient may require general anesthesia. In the United States, providing general anesthesia is relatively easy, requiring the presence of an anesthesiologist or nurse anesthetist, but is difficult in other countries, including Japan, due to more limits in budget and trained personnel, such as nurse anesthetists.
Recently, propofol-based sedation has become popular for endoscopic procedures. This type of sedation is not conscious sedation, but general anesthesia; thus, propofol-based sedation should ideally be provided by an anesthesiologist or a nurse anesthetist under the supervision of an anesthesiologist. However, due to limited anesthesiology resources, propofol is being administered by endoscopists or nurses.
The American Gastroenterological Association (AGA) position is that, if undertaken appropriately, gastroenterologist-directed propofol sedation (GD-P) is medicolegally reasonable. The AGA suggests that GD-P can be safely accomplished by adhering to 5 basic principles[52]: (1) the gastroenterologist should ensure compliance with prevailing guidelines promulgated by professional societies as well as laws and regulations imposed by medical boards and/or credentialing bodies; (2) GD-P should be limited to appropriate, relatively low-risk, patients; (3) gastroenterologists and staff should be trained in the recognition and management of respiratory depression, the pharmacologic properties of propofol, and advanced cardiac life support; (4) endoscopy units should be equipped with resuscitation equipment and drugs, and appropriate monitoring equipment; and (5) the informed consent discussion should inform patient of risks, benefits and alternatives to GD-P, and of the qualification and experience of the endoscopists to administer GD-P. The FDA-approved product label, however, states that “propofol should be administered only by persons trained in the administration of general anesthesia.”
In addition, the European Society of Gastrointestinal Endoscopy (ESGE) states the following[53]: Propofol-based sedation presents similar rates of adverse effects, provides higher postprocedure patient satisfaction for most endoscopic procedures, decreases time to sedation and decreases recovery time. Specific knowledge and skills are necessary for endoscopists and nursing staff using non-anesthesiologist-administered propofol (NAAP) to ensure patient comfort and safety. NAAP performed by endoscopists and nurses should not take place without appropriate training, and self-training in NAAP is strongly discouraged.
With conscious sedation or general anesthesia (including propofol-based sedation), the patient must be appropriately monitored during the procedure.
COMPLICATIONS
Since ESD is an endoscopic surgical procedure, the risk of complications is unavoidable. Bleeding and perforation are common complications in the upper and lower gastrointestinal tract. Stricture is also common in esophageal, pylorus or gastric cardia ESD, especially when a large lesion is removed. The incidence of complications in each organ is listed in Table 3.
Table 3.
Complications and outcomes of endoscopic submucosal dissection
| Total cases | Complication (%) | En-bloc resection(%) | Year1 | Reference | ||||
| Bleeding | Perforation | Stenosis | Operation | |||||
| Esophagus | 107 | 0 | 4 | 18 | 0 | 100 | 2009 | Ono et al[67] |
| 102 | 0 | 6 | - | 0 | 95 | 2005 | Oyama et al[20] | |
| Stomach | 468 | 5.4 | 4.7 | - | 0.4 | 97 | 2010 | Kato et al[59] |
| 478 | 8.2 | 3.6 | - | 0 | - | 2010 | Mannen et al[60] | |
| 589 | 1.8 | 4.5 | - | 0 | 94.9 | 2009 | Isomoto et al[61] | |
| 1000 | 15.6 | 1.2 | - | 0.2 | 95.3 | 2009 | Chung et al[62] | |
| 1033 | 6 | 4 | - | 0.1 | 98 | 2005 | Oda et al[63] | |
| Colon | 1111 | 1.5 | 5.5 | - | 0.5 | 88 | 2010 | Saito et al[64] |
| 200 | 1 | 5.5 | - | 0.5 | 91.5 | 2007 | Fujishiro et al[65] | |
| 268 | 0.3 | 2.2 | - | 0 | 99.2 | 2010 | Toyonaga et al[66] | |
-: not mentioned in the article;
Year of paper publication.
Bleeding
Bleeding is a common complication of ESD (except for esophageal ESD), and can be treated endoscopically on the spot. Soft coagulation with hemostatic forceps (e.g., Coagrasper; FD-410LR or FD-410QR, Olympus, Tokyo) (Figure 3L) has been reported to be effective both in gastric and colorectal ESD[54,55]. Hemoclips are also used to eliminate bleeding, but they must be deployed with care to avoid their getting in the way and interfering with subsequent steps. When visibility and detection of the bleeding vessel is obscured as a result of continuous or massive bleeding, injection of hypertonic saline-epinephrine solution (HSE) may be effective[56-58]. In an easy procedure, the injection of HSE will not impede later steps.
Another type of bleeding is delayed bleeding, which occurs after the procedure. The incidence of delayed bleeding is estimated to be 1.8% to 15.6% in gastric[59-63] and 0.3% to 1.5% in colorectal[64-66], although 0% (in two studies) in esophageal ESD[5,67]. In most reports, it is less than 10%, and only one report showed a relatively high percentage of 15.6%[62]. The authors concluded that the reason for their findings was unclear, but that it may be due to a different definition of delayed bleeding. One risk factor associated with delayed bleeding is the size of the resected area[60,68]. The treatment of delayed bleeding is similar to that used in gastroduodenal ulcer bleeding: endoscopic hemostasis, but some authors reported gastric cases that needed surgery to stop massive bleeding[59,69].
It is best to prevent bleeding, and acid depressant drugs are commonly used before and after the ESD procedure. Different studies have shown that proton pump inhibitors (PPIs) are more effective than histamine H2-receptor antagonists for the prevention of delayed bleeding after ESD[70,71]. For the timing of administration, one report concluded that preoperative and postoperative administration of PPIs yield similar results, and preoperative administration does not offer any benefit over postoperative administration after ESD[69].
Perforation
Perforation is another common complication in ESD. The rate of perforation is 4% in esophageal[5,67], 1.2% to 4.7% in gastric[59-63] and 2.2% to 5.5% in colorectal ESD[40,64,65]. Since mediastinitis and peritonitis consequent to esophageal perforation and colon perforation, respectively, have high mortality rates, surgery was previously the method-of-choice for gastrointestinal perforation. But recently, conservative or endoscopic treatment tends to be selected for smaller perforations when the lesion is clean[72,73]. Most of the perforations due to ESD are smaller and tend to be treated in a non-surgical manner[74,75]. Raju et al[76] evaluated the feasibility and safety of endoscopic closure of colonic perforations with endoclips in a porcine model. Mucosal and submucosal healing was obtained, and the closure prevented fecal soiling of the peritoneal cavity. Occasionally, a small amount of free air is observed (only by CT), but without a visible perforation (by endoscope) after ESD: the so-called transmural air leak. It is reported to be observed in 13% of the patients, but none of them had signs of severe infection. They were successfully treated using conservative treatment[65].
It is very important to immediately recognize when a perforation has occurred. In most perforation cases, the patient becomes agitated, and then calms down after successful closure of the perforation. Upon noticing a perforation, insufflation (air or carbon dioxide) should be stopped immediately. Endoscopic closure should be considered if the lesion is clean (i.e., without feces and so on). If the abdominal cavity is distended because of gas insufflation, decompression treatment should be considered. After injecting local anesthesia with a 23-gauge needle, a 16- to 18-gauge indwelling needle is used to puncture the right lower abdomen to decompress[77]. Taku et al[78] advise that colonoscopists should focus on (1) adequate washing of the area around the lesion, and adequate aspiration of fecal fluid at the time of resection; and (2) changing the patient’s position so that the resected lesion is placed as high as possible, to minimize leakage due to gravity. In addition, the authors suggest that indications for endoscopic clipping of perforations are (1) small defect size (less than 10 mm); (2) the bowel can be prepared adequately; and (3) the patient’s condition remains stable after immediate perforation. After successful endoscopic closure, the patient should be fasted and treated with antibiotics. Formal guidelines for the fasting period have not been established, but one report on colonic perforation reported a mean fasting period of 4.2 d and a mean duration of intravenous antibiotic agents of 5.5 d[79]. Minami et al[74] reported that the average period of fasting after perforation due to gastric ESD was 6.3 d and the median admission period was 10.1 d before 1998, but was 2.1 d and 6.7 d, respectively, from 1999 to 2006. Surgical treatment should be considered when the perforated lesion cannot be closed with endoclips, abdominal pain has exacerbated, or severe peritonitis is suspected. If there is any concern about the patient’s condition, the patient should be sent to surgery without hesitation.
Another concern may be peritoneal dissemination of infection following perforation. However, Ikeda et al[80] reported that among thirty-three patients who had gastrectomy due to perforation as a complication of gastric EMR or ESD, no dissemination was observed. They concluded that dissemination is unlikely to occur after gastric perforation during endoscopic resection.
Stricture
Stricture may occur after ESD when a large lesion is removed. In the esophagus, the estimated rate is 16.7% to 18%[67,81,82]. A risk factor for esophageal stricture is the circumferential resection. Also, in the stomach, circumferential dissection is a risk factor of stricture in the gastric cardia or pylorus[83,84]. In most cases, endoscopic balloon dilation is effective, although there are some refractory cases and some complications (e.g., perforation). Surgical treatment is necessary when the stricture is refractory, or if a perforation occurred after balloon dilation. There are some reports on the prevention of stricture. Local steroid injection is known to prevent stricture[85,86]. Triamcinolone acetonide (in saline at a final concentration of 10 mg/mL) can be injected into each of four quadrants at the narrowest region of the stricture. Recently, oral administration of prednisolone was shown to be effective in preventing esophageal stricture[87,88]. For adults, 30 mg of prednisolone is the starting oral dose and tapered weekly[89].
To reduce the complication of stricture, some materials are reported to help ulcer healing following ESD, including autologous oral mucosal epithelial cell sheets[90,91], biodegradable poly-L-lactic acid stents[92] and extracellular matrix (ECM) scaffold material[93].
Other complications
One case each of phlegmonous gastritis and gastric ischemia has been reported[94,95]. Citrobacter freundii, Enterobacter cloacae and á-streptococcus were cultured from the former case, however, the etiology was unclear in the other case. There are several reports regarding bacteremia following ESD, which concluded that the frequency is low[96,97]. One case series, although possibly not a complication, showed intra-abdominal adhesions after ESD[98]. Intra-abdominal adhesions were observed in all cases with an artificial scarring more than 25 mm in diameter. This finding reveals that, even without an observed perforation during ESD, inflammation of the serosa of the gastrointestinal tract and abdominal cavity may result.
TRAINING
As ESD is a highly technical and demanding invasive procedure, endoscopists require training before performing the procedure. The operator must possess a good understanding of all aspects of ESD: the endoscopes, ESU, ESD knives, injection agents, sedation, complications, and other aspects.
In Asian countries like Japan, Korea and China, gastric intraepithelial neoplasm is more prevalent than in Western countries. Accordingly, most medical institutions in Japan provide training (in a stepwise manner): initially, endoscopists participate as an assistant, starting with ESD in the gastric antrum or the rectum for 20 to 30 cases with a supervisor, then in the proximal stomach, the colon or the esophagus.
In contrast, in Western countries, cases of gastric lesions are less common, resulting in a slow introduction of the ESD technique[99-102]. Efforts are currently underway to change this situation. Possible solutions to improve training and experience are the use of animal models and the establishment of training centers[103-105]. Further, deficiencies in training and experience can now be more rapidly overcome as a result of new technologies. As described above, new advances have led to devices that are easy to handle, making it simpler for beginners to perform ESD. Devices with scissors and forceps, like the Clutch Cutter or other covered devices, are easier to use, leading to fewer complications (e.g., perforation), although the procedure time is longer than those with non-covered devices. The other new approach in ESD, the use of mesna (sodium 2-mercaptoethanesulfonate)[50,51], may also make submucosal dissection safer and faster.
CONCLUSION
In this article, we have described some of the basic knowledge required before starting ESD: this includes the endoscopes used, electrosurgical unit, ESD devices, injection agents, sedation, complications and training. Moreover, we have emphasized that, at least currently, the performance of ESD, which involves invasive endoscopic procedures, requires a high level of technical skill and sufficient knowledge. Therefore, for the safe and effective execution of ESD, we recommend that those wishing to perform ESD must have adequate training, under the guidance of a skilled endoscopist.
Footnotes
Peer reviewer: David Friedel, MD, Winthrop University Hospital, 222 Station Plaza North, Suite 428, Mineola, NY 11501, United States
S- Editor Yang XC L- Editor Webster JR E- Editor Yang XC
References
- 1.Hosokawa K, Yoshida S. [Recent advances in endoscopic mucosal resection for early gastric cancer] Gan To Kagaku Ryoho. 1998;25:476–483. [PubMed] [Google Scholar]
- 2.Gotoda T, Kondo H, Ono H, Saito Y, Yamaguchi H, Saito D, Yokota T. A new endoscopic mucosal resection procedure using an insulation-tipped electrosurgical knife for rectal flat lesions: report of two cases. Gastrointest Endosc. 1999;50:560–563. doi: 10.1016/s0016-5107(99)70084-2. [DOI] [PubMed] [Google Scholar]
- 3.Hirao M, Masuda K, Asanuma T, Naka H, Noda K, Matsuura K, Yamaguchi O, Ueda N. Endoscopic resection of early gastric cancer and other tumors with local injection of hypertonic saline-epinephrine. Gastrointest Endosc. 1988;34:264–269. doi: 10.1016/s0016-5107(88)71327-9. [DOI] [PubMed] [Google Scholar]
- 4.Gotoda T, Yanagisawa A, Sasako M, Ono H, Nakanishi Y, Shimoda T, Kato Y. Incidence of lymph node metastasis from early gastric cancer: estimation with a large number of cases at two large centers. Gastric Cancer. 2000;3:219–225. doi: 10.1007/pl00011720. [DOI] [PubMed] [Google Scholar]
- 5.Ishihara R, Iishi H, Uedo N, Takeuchi Y, Yamamoto S, Yamada T, Masuda E, Higashino K, Kato M, Narahara H, et al. Comparison of EMR and endoscopic submucosal dissection for en bloc resection of early esophageal cancers in Japan. Gastrointest Endosc. 2008;68:1066–1072. doi: 10.1016/j.gie.2008.03.1114. [DOI] [PubMed] [Google Scholar]
- 6.Oka S, Tanaka S, Kaneko I, Mouri R, Hirata M, Kawamura T, Yoshihara M, Chayama K. Advantage of endoscopic submucosal dissection compared with EMR for early gastric cancer. Gastrointest Endosc. 2006;64:877–883. doi: 10.1016/j.gie.2006.03.932. [DOI] [PubMed] [Google Scholar]
- 7.Min BH, Lee JH, Kim JJ, Shim SG, Chang DK, Kim YH, Rhee PL, Kim KM, Park CK, Rhee JC. Clinical outcomes of endoscopic submucosal dissection (ESD) for treating early gastric cancer: comparison with endoscopic mucosal resection after circumferential precutting (EMR-P) Dig Liver Dis. 2009;41:201–209. doi: 10.1016/j.dld.2008.05.006. [DOI] [PubMed] [Google Scholar]
- 8.Oda I, Saito D, Tada M, Iishi H, Tanabe S, Oyama T, Doi T, Otani Y, Fujisaki J, Ajioka Y, et al. A multicenter retrospective study of endoscopic resection for early gastric cancer. Gastric Cancer. 2006;9:262–270. doi: 10.1007/s10120-006-0389-0. [DOI] [PubMed] [Google Scholar]
- 9.Saito Y, Fukuzawa M, Matsuda T, Fukunaga S, Sakamoto T, Uraoka T, Nakajima T, Ikehara H, Fu KI, Itoi T, et al. Clinical outcome of endoscopic submucosal dissection versus endoscopic mucosal resection of large colorectal tumors as determined by curative resection. Surg Endosc. 2010;24:343–352. doi: 10.1007/s00464-009-0562-8. [DOI] [PubMed] [Google Scholar]
- 10.Cao Y, Liao C, Tan A, Gao Y, Mo Z, Gao F. Meta-analysis of endoscopic submucosal dissection versus endoscopic mucosal resection for tumors of the gastrointestinal tract. Endoscopy. 2009;41:751–757. doi: 10.1055/s-0029-1215053. [DOI] [PubMed] [Google Scholar]
- 11.Kume K, Yamasaki M, Yoshikawa I, Otsuki M. Grasping-forceps-assisted endoscopic submucosal dissection using a novel irrigation cap-knife for large superficial early gastric cancer. Endoscopy. 2007;39:566–569. doi: 10.1055/s-2007-966394. [DOI] [PubMed] [Google Scholar]
- 12.Nakajima K, Lee SW, Sonoda T, Milsom JW. Intraoperative carbon dioxide colonoscopy: a safe insufflation alternative for locating colonic lesions during laparoscopic surgery. Surg Endosc. 2005;19:321–325. doi: 10.1007/s00464-004-8915-9. [DOI] [PubMed] [Google Scholar]
- 13.Bretthauer M, Lynge AB, Thiis-Evensen E, Hoff G, Fausa O, Aabakken L. Carbon dioxide insufflation in colonoscopy: safe and effective in sedated patients. Endoscopy. 2005;37:706–709. doi: 10.1055/s-2005-870154. [DOI] [PubMed] [Google Scholar]
- 14.Saito Y, Uraoka T, Matsuda T, Emura F, Ikehara H, Mashimo Y, Kikuchi T, Kozu T, Saito D. A pilot study to assess the safety and efficacy of carbon dioxide insufflation during colorectal endoscopic submucosal dissection with the patient under conscious sedation. Gastrointest Endosc. 2007;65:537–542. doi: 10.1016/j.gie.2006.11.002. [DOI] [PubMed] [Google Scholar]
- 15.Nonaka S, Saito Y, Takisawa H, Kim Y, Kikuchi T, Oda I. Safety of carbon dioxide insufflation for upper gastrointestinal tract endoscopic treatment of patients under deep sedation. Surg Endosc. 2010;24:1638–1645. doi: 10.1007/s00464-009-0824-5. [DOI] [PubMed] [Google Scholar]
- 16.Kohler A, Maier M, Benz C, Martin WR, Farin G, Riemann JF. A new HF current generator with automatically controlled system (Endocut mode) for endoscopic sphincterotomy--preliminary experience. Endoscopy. 1998;30:351–355. doi: 10.1055/s-2007-1001281. [DOI] [PubMed] [Google Scholar]
- 17.Yamamoto H, Kawata H, Sunada K, Satoh K, Kaneko Y, Ido K, Sugano K. Success rate of curative endoscopic mucosal resection with circumferential mucosal incision assisted by submucosal injection of sodium hyaluronate. Gastrointest Endosc. 2002;56:507–512. doi: 10.1067/mge.2002.128108. [DOI] [PubMed] [Google Scholar]
- 18.Yahagi N, Fujishiro M, Kakushima N, Kobayashi K, Hashimoto T, Oka M, Iguchi M, Enomoto S, Ichinose M, Niwa H and Omata M. Endoscopic submucosal dissection for early gastric cancer using the tip of an electrosurgical snare (thin type) Dig Endosc. 2004;16:34–38. [Google Scholar]
- 19.Kodashima S, Fujishiro M, Yahagi N, Kakushima N, Ichinose M, Omata M. Endoscopic submucosal dissection for gastric neoplasia: experience with the flex-knife. Acta Gastroenterol Belg. 2006;69:224–229. [PubMed] [Google Scholar]
- 20.Oyama T, Tomori A, Hotta K, Morita S, Kominato K, Tanaka M, Miyata Y. Endoscopic submucosal dissection of early esophageal cancer. Clin Gastroenterol Hepatol. 2005;3:S67–S70. doi: 10.1016/s1542-3565(05)00291-0. [DOI] [PubMed] [Google Scholar]
- 21.Inoue H, Kudo S. A novel procedure of en bloc EMR using triangle-tipped knife. Gastrointestinal Endosc. 2003;57:AB 86. [Google Scholar]
- 22.Toyonaga T, Nishino E, Hirooka T, Dozaiku T, Sugiyama T, Iwata Y, Ono W, Ueda C, Tomita M, Hirooka T, et al. Use of short needle knife for esophageal endoscopic submucosal dissection. Dig Endosc. 2005;17:246–252. [Google Scholar]
- 23.Takeuchi Y, Uedo N, Ishihara R, Iishi H, Kizu T, Inoue T, Chatani R, Hanaoka N, Taniguchi T, Kawada N, et al. Efficacy of an endo-knife with a water-jet function (Flushknife) for endoscopic submucosal dissection of superficial colorectal neoplasms. Am J Gastroenterol. 2010;105:314–322. doi: 10.1038/ajg.2009.547. [DOI] [PubMed] [Google Scholar]
- 24.Toyonaga T, Man-I M, Fujita T, Nishino E, Ono W, Morita Y, Sanuki T, Masuda A, Yoshida M, Kutsumi H, et al. The performance of a novel ball-tipped Flush knife for endoscopic submucosal dissection: a case-control study. Aliment Pharmacol Ther. 2010;32:908–915. doi: 10.1111/j.1365-2036.2010.04425.x. [DOI] [PubMed] [Google Scholar]
- 25.Ono H, Kondo H, Gotoda T, Shirao K, Yamaguchi H, Saito D, Hosokawa K, Shimoda T, Yoshida S. Endoscopic mucosal resection for treatment of early gastric cancer. Gut. 2001;48:225–229. doi: 10.1136/gut.48.2.225. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Ono H, Hasuike N, Inui T, Takizawa K, Ikehara H, Yamaguchi Y, Otake Y, Matsubayashi H. Usefulness of a novel electrosurgical knife, the insulation-tipped diathermic knife-2, for endoscopic submucosal dissection of early gastric cancer. Gastric Cancer. 2008;11:47–52. doi: 10.1007/s10120-008-0452-0. [DOI] [PubMed] [Google Scholar]
- 27.Kawahara Y, Takenaka R, OkadaH Risk management to prevent perforation during endoscopic submucosal dissection. Dig Endosc. 2007;19 Supplement s1:S9–S13. [Google Scholar]
- 28.Honma K, Kobayashi M, Watanabe H, Suga T, Tominaga K, Yamagata M, Hiraishi H. Endoscopic submucosal dissection for colorectal neoplasia. Dig Endosc. 2010;22:307–311. doi: 10.1111/j.1443-1661.2010.01018.x. [DOI] [PubMed] [Google Scholar]
- 29.Akahoshi K, Akahane H, Murata A, Akiba H, Oya M. Endoscopic submucosal dissection using a novel grasping type scissors forceps. Endoscopy. 2007;39:1103–1105. doi: 10.1055/s-2007-966842. [DOI] [PubMed] [Google Scholar]
- 30.Akahoshi K, Honda K, Akahane H, Akiba H, Matsui N, Motomura Y, Kubokawa M, Endo S, Higuchi N, Oya M. Endoscopic submucosal dissection by using a grasping-type scissors forceps: a preliminary clinical study (with video) Gastrointest Endosc. 2008;67:1128–1133. doi: 10.1016/j.gie.2007.12.007. [DOI] [PubMed] [Google Scholar]
- 31.Akahoshi K, Akahane H. A new breakthrough: ESD using a newly developed grasping type scissor forceps for early gastrointestinal tract neoplasms. World J Gastrointest Endosc. 2010;2:90–96. doi: 10.4253/wjge.v2.i3.90. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Kim HG, Cho JY, Bok GH, Cho WY, Kim WJ, Hong SJ, Ko BM, Kim JO, Lee JS, Lee MS, et al. A novel device for endoscopic submucosal dissection, the Fork knife. World J Gastroenterol. 2008;14:6726–6732. doi: 10.3748/wjg.14.6726. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Yahagi N, Neuhaus H, Schumacher B, Neugebauer A, Kaehler GF, Schenk M, Fischer K, Fujishiro M, Enderle MD. Comparison of standard endoscopic submucosal dissection (ESD) versus an optimized ESD technique for the colon: an animal study. Endoscopy. 2009;41:340–345. doi: 10.1055/s-0029-1214473. [DOI] [PubMed] [Google Scholar]
- 34.von Renteln D, Pohl H, Vassiliou MC, Walton MM, Rothstein RI. Endoscopic submucosal dissection by using a flexible Maryland dissector: a randomized, controlled, porcine study (with videos) Gastrointest Endosc. 2010;71:1056–1062. doi: 10.1016/j.gie.2010.01.049. [DOI] [PubMed] [Google Scholar]
- 35.Uraoka T, Saito Y, Yamamoto K, Fujii T. Submucosal injection solution for gastrointestinal tract endoscopic mucosal resection and endoscopic submucosal dissection. Drug Des Devel Ther. 2009;2:131–138. doi: 10.2147/dddt.s3219. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Polymeros D, Kotsalidis G, Triantafyllou K, Karamanolis G, Panagiotides JG, Ladas SD. Comparative performance of novel solutions for submucosal injection in porcine stomachs: An ex vivo study. Dig Liver Dis. 2010;42:226–229. doi: 10.1016/j.dld.2009.05.018. [DOI] [PubMed] [Google Scholar]
- 37.Kantsevoy SV, Adler DG, Conway JD, Diehl DL, Farraye FA, Kwon R, Mamula P, Rodriguez S, Shah RJ, Wong Kee Song LM, et al. Endoscopic mucosal resection and endoscopic submucosal dissection. Gastrointest Endosc. 2008;68:11–18. doi: 10.1016/j.gie.2008.01.037. [DOI] [PubMed] [Google Scholar]
- 38.Fujishiro M, Yahagi N, Kashimura K, Mizushima Y, Oka M, Enomoto S, Kakushima N, Kobayashi K, Hashimoto T, Iguchi M, et al. Comparison of various submucosal injection solutions for maintaining mucosal elevation during endoscopic mucosal resection. Endoscopy. 2004;36:579–583. doi: 10.1055/s-2004-814517. [DOI] [PubMed] [Google Scholar]
- 39.Lee SH, Park JH, Park do H, Chung IK, Kim HS, Park SH, Kim SJ, Cho HD. Clinical efficacy of EMR with submucosal injection of a fibrinogen mixture: a prospective randomized trial. Gastrointest Endosc. 2006;64:691–696. doi: 10.1016/j.gie.2006.07.032. [DOI] [PubMed] [Google Scholar]
- 40.Yamasaki M, Kume K, Kanda K, Yoshikawa I, Otsuki M. A new method of endoscopic submucosal dissection using submucosal injection of jelly. Endoscopy. 2005;37:1156–1157. doi: 10.1055/s-2005-870372. [DOI] [PubMed] [Google Scholar]
- 41.Yamasaki M, Kume K, Yoshikawa I, Otsuki M. A novel method of endoscopic submucosal dissection with blunt abrasion by submucosal injection of sodium carboxymethylcellulose: an animal preliminary study. Gastrointest Endosc. 2006;64:958–965. doi: 10.1016/j.gie.2006.07.035. [DOI] [PubMed] [Google Scholar]
- 42.Ishizuka T, Ishihara M, Aiko S, Nogami Y, Nakamura S, Kanatani Y, Kishimoto S, Hattori H, Horio T, Tanaka Y, et al. Experimental evaluation of photocrosslinkable chitosan hydrogel as injection solution for endoscopic resection. Endoscopy. 2009;41:25–28. doi: 10.1055/s-0028-1103483. [DOI] [PubMed] [Google Scholar]
- 43.Sumiyoshi T, Fujii T, Sumiyoshi Y, Matsuda T, Kozu T, Saito D, Akasu T, Fu KI. Injected substances to the submucosa in endoscopic mucosal resection: glycerin solution versus normal saline solution. Gastrointest Endosc. 2002;55:AB 110. [Google Scholar]
- 44.Yamamoto H, Yube T, Isoda N, Sato Y, Sekine Y, Higashizawa T, Ido K, Kimura K, Kanai N. A novel method of endoscopic mucosal resection using sodium hyaluronate. Gastrointest Endosc. 1999;50:251–256. doi: 10.1016/s0016-5107(99)70234-8. [DOI] [PubMed] [Google Scholar]
- 45.Kita H, Yamamoto H, Miyata T, Sunada K, Iwamoto M, Yano T, Yoshizawa M, Hanatsuka K, Arashiro M, Omata T, et al. Endoscopic submucosal dissection using sodium hyaluronate, a new technique for en bloc resection of a large superficial tumor in the colon. Inflammopharmacology. 2007;15:129–131. doi: 10.1007/s10787-007-1572-6. [DOI] [PubMed] [Google Scholar]
- 46.Folwaczny C, Heldwein W, Obermaier G, Schindlbeck N. Influence of prophylactic local administration of epinephrine on bleeding complications after polypectomy. Endoscopy. 1997;29:31–33. doi: 10.1055/s-2007-1004058. [DOI] [PubMed] [Google Scholar]
- 47.Hsieh YH, Lin HJ, Tseng GY, Perng CL, Li AF, Chang FY, Lee SD. Is submucosal epinephrine injection necessary before polypectomy? A prospective, comparative study. Hepatogastroenterology. 2001;48:1379–1382. [PubMed] [Google Scholar]
- 48.Lee SH, Chung IK, Kim SJ, Kim JO, Ko BM, Kim WH, Kim HS, Park DI, Kim HJ, Byeon JS, et al. Comparison of postpolypectomy bleeding between epinephrine and saline submucosal injection for large colon polyps by conventional polypectomy: a prospective randomized, multicenter study. World J Gastroenterol. 2007;13:2973–2977. doi: 10.3748/wjg.v13.i21.2973. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Sanchez-Yague A, Yamaguchi Y, Takao T, Tanaka M, Kakushima N, Takizawa K, Ikehara H, Matsubayashi H, Ono H. Endoscopic submucosal dissection of a lower rectal polyp proximal to the dentate line by using local lidocaine injection. Gastrointest Endosc. 2011;73:405–407. doi: 10.1016/j.gie.2010.06.044. [DOI] [PubMed] [Google Scholar]
- 50.Sumiyama K, Gostout CJ, Rajan E, Bakken TA, Knipschield MA. Chemically assisted endoscopic mechanical submucosal dissection by using mesna. Gastrointest Endosc. 2008;67:534–538. doi: 10.1016/j.gie.2007.10.041. [DOI] [PubMed] [Google Scholar]
- 51.Sumiyama K, Tajiri H, Gostout CJ, Kawamura M, Imazu H, Ohya TR, Ikeda K, Goda K, Saito S, Kato T. Chemically assisted submucosal injection facilitates endoscopic submucosal dissection of gastric neoplasms. Endoscopy. 2010;42:627–632. doi: 10.1055/s-0029-1244223. [DOI] [PubMed] [Google Scholar]
- 52.Cohen LB, Delegge MH, Aisenberg J, Brill JV, Inadomi JM, Kochman ML, Piorkowski JD. AGA Institute review of endoscopic sedation. Gastroenterology. 2007;133:675–701. doi: 10.1053/j.gastro.2007.06.002. [DOI] [PubMed] [Google Scholar]
- 53.Dumonceau JM, Riphaus A, Aparicio JR, Beilenhoff U, Knape JT, Ortmann M, Paspatis G, Ponsioen CY, Racz I, Schreiber F, et al. European Society of Gastrointestinal Endoscopy, European Society of Gastroenterology and Endoscopy Nurses and Associates, and the European Society of Anaesthesiology Guideline: Non-anesthesiologist administration of propofol for GI endoscopy. Endoscopy. 2010;42:960–974. doi: 10.1055/s-0030-1255728. [DOI] [PubMed] [Google Scholar]
- 54.Arima S, Sakata Y, Ogata S, Tominaga N, Tsuruoka N, Mannen K, Shiraishi R, Shimoda R, Tsunada S, Sakata H, et al. Evaluation of hemostasis with soft coagulation using endoscopic hemostatic forceps in comparison with metallic hemoclips for bleeding gastric ulcers: a prospective, randomized trial. J Gastroenterol. 2010;45:501–505. doi: 10.1007/s00535-009-0186-8. [DOI] [PubMed] [Google Scholar]
- 55.Yoshida N, Naito Y, Kugai M, Inoue K, Wakabayashi N, Yagi N, Yanagisawa A, Yoshikawa T. Efficient hemostatic method for endoscopic submucosal dissection of colorectal tumors. World J Gastroenterol. 2010;16:4180–4186. doi: 10.3748/wjg.v16.i33.4180. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Hirao M, Kobayashi T, Masuda K, Yamaguchi S, Noda K, Matsuura K, Naka H, Kawauchi H, Namiki M. Endoscopic local injection of hypertonic saline-epinephrine solution to arrest hemorrhage from the upper gastrointestinal tract. Gastrointest Endosc. 1985;31:313–317. doi: 10.1016/s0016-5107(85)72213-4. [DOI] [PubMed] [Google Scholar]
- 57.Hirao M, Yamazaki H, Masuda K, Kobayashi T, Seto F. Hemostatic procedure by endoscope for gastrointestinal bleeding; clinical practice of endoscopic local injection of hypertonic sodium epinephrine (HS-E) slolution. Stomach Intestine. 1980;7:751–755. [Google Scholar]
- 58.Hirao M, Kobayashi T, Masuda K, Yamaguchi S, Noda K, Yamazaki H, Naka K, Kawauchi H, Sato F. Endoscopic local injection of hypertonic saline epinephrine solution to arrest hemorrhage from the upper digestive tract. I. Fundamental research. Gastroenterol Endosc. 1981;23:1097–1107. [Google Scholar]
- 59.Kato M, Nishida T, Tsutsui S, Komori M, Michida T, Yamamoto K, Kawai N, Kitamura S, Zushi S, Nishihara A, et al. Endoscopic submucosal dissection as a treatment for gastric noninvasive neoplasia: a multicenter study by Osaka University ESD Study Group. J Gastroenterol. 2011;46:325–331. doi: 10.1007/s00535-010-0350-1. [DOI] [PubMed] [Google Scholar]
- 60.Mannen K, Tsunada S, Hara M, Yamaguchi K, Sakata Y, Fujise T, Noda T, Shimoda R, Sakata H, Ogata S, et al. Risk factors for complications of endoscopic submucosal dissection in gastric tumors: analysis of 478 lesions. J Gastroenterol. 2010;45:30–36. doi: 10.1007/s00535-009-0137-4. [DOI] [PubMed] [Google Scholar]
- 61.Isomoto H, Shikuwa S, Yamaguchi N, Fukuda E, Ikeda K, Nishiyama H, Ohnita K, Mizuta Y, Shiozawa J, Kohno S. Endoscopic submucosal dissection for early gastric cancer: a large-scale feasibility study. Gut. 2009;58:331–336. doi: 10.1136/gut.2008.165381. [DOI] [PubMed] [Google Scholar]
- 62.Chung IK, Lee JH, Lee SH, Kim SJ, Cho JY, Cho WY, Hwangbo Y, Keum BR, Park JJ, Chun HJ, et al. Therapeutic outcomes in 1000 cases of endoscopic submucosal dissection for early gastric neoplasms: Korean ESD Study Group multicenter study. Gastrointest Endosc. 2009;69:1228–1235. doi: 10.1016/j.gie.2008.09.027. [DOI] [PubMed] [Google Scholar]
- 63.Oda I, Gotoda T, Hamanaka H, Eguchi T, Saito Y, Matsuda T, Bhandari P, Emura F, Saito D and Ono H. Endoscopic submucosal dissection for early gastric cancer: Technical feasibility, operation time and complications from a large consecutive series. Digestive Endoscopy. 2005;1:54–58. [Google Scholar]
- 64.Saito Y, Uraoka T, Yamaguchi Y, Hotta K, Sakamoto N, Ikematsu H, Fukuzawa M, Kobayashi N, Nasu J, Michida T, et al. A prospective, multicenter study of 1111 colorectal endoscopic submucosal dissections (with video) Gastrointest Endosc. 2010;72:1217–1225. doi: 10.1016/j.gie.2010.08.004. [DOI] [PubMed] [Google Scholar]
- 65.Fujishiro M, Yahagi N, Kakushima N, Kodashima S, Muraki Y, Ono S, Yamamichi N, Tateishi A, Oka M, Ogura K, et al. Outcomes of endoscopic submucosal dissection for colorectal epithelial neoplasms in 200 consecutive cases. Clin Gastroenterol Hepatol. 2007;5:678–83; quiz 645. doi: 10.1016/j.cgh.2007.01.006. [DOI] [PubMed] [Google Scholar]
- 66.Toyonaga T, Man-i M, Fujita T, East JE, Nishino E, Ono W, Morita Y, Sanuki T, Yoshida M, Kutsumi H, et al. Retrospective study of technical aspects and complications of endoscopic submucosal dissection for laterally spreading tumors of the colorectum. Endoscopy. 2010;42:714–722. doi: 10.1055/s-0030-1255654. [DOI] [PubMed] [Google Scholar]
- 67.Ono S, Fujishiro M, Niimi K, Goto O, Kodashima S, Yamamichi N, Omata M. Long-term outcomes of endoscopic submucosal dissection for superficial esophageal squamous cell neoplasms. Gastrointest Endosc. 2009;70:860–866. doi: 10.1016/j.gie.2009.04.044. [DOI] [PubMed] [Google Scholar]
- 68.Okada K, Yamamoto Y, Kasuga A, Omae M, Kubota M, Hirasawa T, Ishiyama A, Chino A, Tsuchida T, Fujisaki J, et al. Risk factors for delayed bleeding after endoscopic submucosal dissection for gastric neoplasm. Surg Endosc. 2011;25:98–107. doi: 10.1007/s00464-010-1137-4. [DOI] [PubMed] [Google Scholar]
- 69.Ono S, Kato M, Ono Y, Nakagawa M, Nakagawa S, Shimizu Y, Asaka M. Effects of preoperative administration of omeprazole on bleeding after endoscopic submucosal dissection: a prospective randomized controlled trial. Endoscopy. 2009;41:299–303. doi: 10.1055/s-0029-1214530. [DOI] [PubMed] [Google Scholar]
- 70.Uedo N, Takeuchi Y, Yamada T, Ishihara R, Ogiyama H, Yamamoto S, Kato M, Tatsumi K, Masuda E, Tamai C, et al. Effect of a proton pump inhibitor or an H2-receptor antagonist on prevention of bleeding from ulcer after endoscopic submucosal dissection of early gastric cancer: a prospective randomized controlled trial. Am J Gastroenterol. 2007;102:1610–1616. doi: 10.1111/j.1572-0241.2007.01197.x. [DOI] [PubMed] [Google Scholar]
- 71.Jeong HK, Park CH, Jun CH, Lee GH, Kim HI, Kim HS, Choi SK, Rew JS. A prospective randomized trial of either famotidine or pantoprazole for the prevention of bleeding after endoscopic submucosal dissection. J Korean Med Sci. 2007;22:1055–1059. doi: 10.3346/jkms.2007.22.6.1055. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Wesdorp IC, Bartelsman JF, Huibregtse K, den Hartog Jager FC, Tytgat GN. Treatment of instrumental oesophageal perforation. Gut. 1984;25:398–404. doi: 10.1136/gut.25.4.398. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Yoshikane H, Hidano H, Sakakibara A, Ayakawa T, Mori S, Kawashima H, Goto H, Niwa Y. Endoscopic repair by clipping of iatrogenic colonic perforation. Gastrointest Endosc. 1997;46:464–466. doi: 10.1016/s0016-5107(97)70045-2. [DOI] [PubMed] [Google Scholar]
- 74.Minami S, Gotoda T, Ono H, Oda I, Hamanaka H. Complete endoscopic closure of gastric perforation induced by endoscopic resection of early gastric cancer using endoclips can prevent surgery (with video) Gastrointest Endosc. 2006;63:596–601. doi: 10.1016/j.gie.2005.07.029. [DOI] [PubMed] [Google Scholar]
- 75.Neuhaus H, Costamagna G, Devière J, Fockens P, Ponchon T, Rösch T. Endoscopic submucosal dissection (ESD) of early neoplastic gastric lesions using a new double-channel endoscope (the "R-scope") Endoscopy. 2006;38:1016–1023. doi: 10.1055/s-2006-944830. [DOI] [PubMed] [Google Scholar]
- 76.Raju GS, Pham B, Xiao SY, Brining D, Ahmed I. A pilot study of endoscopic closure of colonic perforations with endoclips in a swine model. Gastrointest Endosc. 2005;62:791–795. doi: 10.1016/j.gie.2005.07.047. [DOI] [PubMed] [Google Scholar]
- 77.Saito Y, Matsuda T, Kikuchi T, Ikehara H and Uraoka T. Successful endoscopic closures of colonic perforation requring abdominal decompression after endscopic mucosal resection and endoscopic submucosal dissedction for early colon cancer. Dig Endosc. 2007;19 Supplement s1:S34–S39. [Google Scholar]
- 78.Taku K, Sano Y, Fu KI, Saito Y. Iatrogenic perforation at therapeutic colonoscopy: should the endoscopist attempt closure using endoclips or transfer immediately to surgery? Endoscopy. 2006;38:428. doi: 10.1055/s-2006-925248. [DOI] [PubMed] [Google Scholar]
- 79.Taku K, Sano Y, Fu KI, Saito Y, Matsuda T, Uraoka T, Yoshino T, Yamaguchi Y, Fujita M, Hattori S, et al. Iatrogenic perforation associated with therapeutic colonoscopy: a multicenter study in Japan. J Gastroenterol Hepatol. 2007;22:1409–1414. doi: 10.1111/j.1440-1746.2007.05022.x. [DOI] [PubMed] [Google Scholar]
- 80.Ikehara H, Gotoda T, Ono H, Oda I, Saito D. Gastric perforation during endoscopic resection for gastric carcinoma and the risk of peritoneal dissemination. Br J Surg. 2007;94:992–995. doi: 10.1002/bjs.5636. [DOI] [PubMed] [Google Scholar]
- 81.Mizuta H, Nishimori I, Kuratani Y, Higashidani Y, Kohsaki T, Onishi S. Predictive factors for esophageal stenosis after endoscopic submucosal dissection for superficial esophageal cancer. Dis Esophagus. 2009;22:626–631. doi: 10.1111/j.1442-2050.2009.00954.x. [DOI] [PubMed] [Google Scholar]
- 82.Ono S, Fujishiro M, Niimi K, Goto O, Kodashima S, Yamamichi N, Omata M. Predictors of postoperative stricture after esophageal endoscopic submucosal dissection for superficial squamous cell neoplasms. Endoscopy. 2009;41:661–665. doi: 10.1055/s-0029-1214867. [DOI] [PubMed] [Google Scholar]
- 83.Tsunada S, Ogata S, Mannen K, Arima S, Sakata Y, Shiraishi R, Shimoda R, Ootani H, Yamaguchi K, Fujise T, et al. Case series of endoscopic balloon dilation to treat a stricture caused by circumferential resection of the gastric antrum by endoscopic submucosal dissection. Gastrointest Endosc. 2008;67:979–983. doi: 10.1016/j.gie.2007.12.023. [DOI] [PubMed] [Google Scholar]
- 84.Coda S, Oda I, Gotoda T, Yokoi C, Kikuchi T, Ono H. Risk factors for cardiac and pyloric stenosis after endoscopic submucosal dissection, and efficacy of endoscopic balloon dilation treatment. Endoscopy. 2009;41:421–426. doi: 10.1055/s-0029-1214642. [DOI] [PubMed] [Google Scholar]
- 85.Holder TM, Ashcraft KW, Leape L. The treatment of patients with esophageal strictures by local steroid injections. J Pediatr Surg. 1969;4:646–653. doi: 10.1016/0022-3468(69)90492-8. [DOI] [PubMed] [Google Scholar]
- 86.Lee M, Kubik CM, Polhamus CD, Brady CE, Kadakia SC. Preliminary experience with endoscopic intralesional steroid injection therapy for refractory upper gastrointestinal strictures. Gastrointest Endosc. 1995;41:598–601. doi: 10.1016/s0016-5107(95)70199-0. [DOI] [PubMed] [Google Scholar]
- 87.Morikawa N, Honna T, Kuroda T, Watanabe K, Tanaka H, Takayasu H, Fujino A, Tanemura H, Matsukubo M. High dose intravenous methylprednisolone resolves esophageal stricture resistant to balloon dilatation with intralesional injection of dexamethasone. Pediatr Surg Int. 2008;24:1161–1164. doi: 10.1007/s00383-008-2224-7. [DOI] [PubMed] [Google Scholar]
- 88.Hishiki T, Kouchi K, Saito T, Terui K, Sato Y, Mitsunaga T, Nakata M, Yoshida H. Successful treatment of severe refractory anastomotic stricture in an infant after esophageal atresia repair by endoscopic balloon dilation combined with systemic administration of dexamethasone. Pediatr Surg Int. 2009;25:531–533. doi: 10.1007/s00383-009-2367-1. [DOI] [PubMed] [Google Scholar]
- 89.Isomoto H, Yamaguchi N, Nakayama T, Hayashi T, Nishiyama H, Ohnita K, Takeshima F, Shikuwa S, Kohno S, Nakao K. Management of esophageal stricture after complete circular endoscopic submucosal dissection for superficial esophageal squamous cell carcinoma. BMC Gastroenterol. 2011;11:46. doi: 10.1186/1471-230X-11-46. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90.Ohki T, Yamato M, Murakami D, Takagi R, Yang J, Namiki H, Okano T, Takasaki K. Treatment of oesophageal ulcerations using endoscopic transplantation of tissue-engineered autologous oral mucosal epithelial cell sheets in a canine model. Gut. 2006;55:1704–1710. doi: 10.1136/gut.2005.088518. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 91.Takagi R, Murakami D, Kondo M, Ohki T, Sasaki R, Mizutani M, Yamato M, Nishida K, Namiki H, Yamamoto M, et al. Fabrication of human oral mucosal epithelial cell sheets for treatment of esophageal ulceration by endoscopic submucosal dissection. Gastrointest Endosc. 2010;72:1253–1259. doi: 10.1016/j.gie.2010.08.007. [DOI] [PubMed] [Google Scholar]
- 92.Saito Y, Tanaka T, Andoh A, Minematsu H, Hata K, Tsujikawa T, Nitta N, Murata K, Fujiyama Y. Novel biodegradable stents for benign esophageal strictures following endoscopic submucosal dissection. Dig Dis Sci. 2008;53:330–333. doi: 10.1007/s10620-007-9873-6. [DOI] [PubMed] [Google Scholar]
- 93.Nieponice A, McGrath K, Qureshi I, Beckman EJ, Luketich JD, Gilbert TW, Badylak SF. An extracellular matrix scaffold for esophageal stricture prevention after circumferential EMR. Gastrointest Endosc. 2009;69:289–296. doi: 10.1016/j.gie.2008.04.022. [DOI] [PubMed] [Google Scholar]
- 94.Ajibe H, Osawa H, Yoshizawa M, Yamamoto H, Satoh K, Koinuma K, Morishima K, Hosoya Y, Yasuda Y, Sugano K. Phlegmonous gastritis after endoscopic submucosal dissection for early gastric cancer. Therap Adv Gastroenterol. 2008;1:91–95. doi: 10.1177/1756283X08095746. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 95.Probst A, Maerkl B, Bittinger M, Messmann H. Gastric ischemia following endoscopic submucosal dissection of early gastric cancer. Gastric Cancer. 2010;13:58–61. doi: 10.1007/s10120-009-0539-2. [DOI] [PubMed] [Google Scholar]
- 96.Min BH, Chang DK, Kim DU, Kim YH, Rhee PL, Kim JJ, Rhee JC. Low frequency of bacteremia after an endoscopic resection for large colorectal tumors in spite of extensive submucosal exposure. Gastrointest Endosc. 2008;68:105–110. doi: 10.1016/j.gie.2007.11.051. [DOI] [PubMed] [Google Scholar]
- 97.Itaba S, Iboshi Y, Nakamura K, Ogino H, Sumida Y, Aso A, Yoshinaga S, Akiho H, Igarashi H, Kato M, et al. Low-frequency of bacteremia after endoscopic submucosal dissection of the stomach. Dig Endosc. 2011;23:69–72. doi: 10.1111/j.1443-1661.2010.01066.x. [DOI] [PubMed] [Google Scholar]
- 98.Akagi T, Shiraishi N, Hiroishi K, Etoh T, Yasuda K, Kitano S. Case series of intra-abdominal adhesions induced by artificial ulceration after endoscopic submucosal dissection before additional laparoscopic gastrectomy. Gastrointest Endosc. 2010;72:438–443. doi: 10.1016/j.gie.2010.03.1066. [DOI] [PubMed] [Google Scholar]
- 99.Bergman JJ. How to justify endoscopic submucosal dissection in the Western world. Endoscopy. 2009;41:988–990. doi: 10.1055/s-0029-1215247. [DOI] [PubMed] [Google Scholar]
- 100.Neuhaus H. Endoscopic mucosal resection and endoscopic submucosal dissection in the West--too many concerns and caveats? Endoscopy. 2010;42:859–861. doi: 10.1055/s-0030-1255724. [DOI] [PubMed] [Google Scholar]
- 101.Ribeiro-Mourão F, Pimentel-Nunes P, Dinis-Ribeiro M. Endoscopic submucosal dissection for gastric lesions: results of an European inquiry. Endoscopy. 2010;42:814–819. doi: 10.1055/s-0030-1255778. [DOI] [PubMed] [Google Scholar]
- 102.Teoh AY, Chiu PW, Wong SK, Sung JJ, Lau JY, Ng EK. Difficulties and outcomes in starting endoscopic submucosal dissection. Surg Endosc. 2010;24:1049–1054. doi: 10.1007/s00464-009-0724-8. [DOI] [PubMed] [Google Scholar]
- 103.Vázquez-Sequeiros E, de Miquel DB, Olcina JR, Martín JA, García M, Lucas DJ, Garrido E, González C, Blanco AP, Arnau MR, et al. Training model for teaching endoscopic submucosal dissection of gastric tumors. Rev Esp Enferm Dig. 2009;101:546–552. doi: 10.4321/s1130-01082009000800005. [DOI] [PubMed] [Google Scholar]
- 104.Tanimoto MA, Torres-Villalobos G, Fujita R, Santillan-Doherty P, Albores-Saavedra J, Gutierrez G, Martin-del-Campo LA, Bravo-Reyna C, Villanueva O, Villalobos JJ, et al. Endoscopic submucosal dissection in dogs in a World Gastroenterology Organisation training center. World J Gastroenterol. 2010;16:1759–1764. doi: 10.3748/wjg.v16.i14.1759. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 105.Deprez PH, Bergman JJ, Meisner S, Ponchon T, Repici A, Dinis-Ribeiro M, Haringsma J. Current practice with endoscopic submucosal dissection in Europe: position statement from a panel of experts. Endoscopy. 2010;42:853–858. doi: 10.1055/s-0030-1255563. [DOI] [PubMed] [Google Scholar]