

Abstract
A case formulation content coding method is described and applied to the formulation section of 56 intake evaluations randomly selected from an outpatient psychiatric clinic. The coding manual showed good reliability (mean kappa = 0.86) across content and quality categories. Although 95% of the formulations included descriptive infor- mation, only 37% addressed hypothesized predisposing life events accounting for the individual's presenting problems, and 16% included a precipitating stressor. Only 43% inferred a psychological mechanism, 2% inferred a biological mechanism, and 2% mentioned sociocultural factors. Formulations were more descriptive than inferential, more simple than complex, and moderately precise in use of language. In sum, clinicians used the formulation primarily to summarize descriptive information rather than to integrate it into a hypothesis about the causes, precipitants, and maintaining influences of an individual's problems.
Psychotherapists appear to agree that case formulation skills are fundamental to providing effective treatment,1–3 particularly for difficult-to-treat patients with comorbid mental disorders.4 Sperry et al.3 reflect this agreement in noting that “the ability to conceptualize and write succinct case formulations is considered basic to daily clinical practice” (p. vii). Some argue that the advent of managed care and time-limited psychotherapy has heightened the importance of case formulation skills because psychotherapists are increasingly called on to work more efficiently and to justify the value and expense of their services.2,3,5
In light of the consensus that case formulation skills are important, it is striking that little research has addressed the formulation skills of clinicians. Research in this area would not only provide feedback to clinicians that could aid in training, but would also serve the goal of consumer protection by ensuring that a well-thought-out understanding of the patient has been attempted and an appropriate treatment plan developed. In our review of the literature, we found only two studies that directly addressed formulation skills and none in which these skills are directly assessed. Both studies suggest that clinicians may not feel that they are well trained in case formulation. Surveying a small sample of psychiatry program directors and senior psychiatry residents, Fleming and Patterson6 found that fewer that half of the programs provided guidelines for case formulation, and most respondents agreed strongly that standardized, biopsychosocially based guidelines for case formulation were needed. In an earlier survey, Ben-Aron and McCormick7 found that 60% of psychiatry chairs and program directors believed that case formulation was important but was inadequately stressed in training.
These respondents' views are echoed by numerous writers about psychotherapy. Sperry et al.3 recently described case formulation as a poorly defined and undertaught clinical skill. Similarly, Perry et al.8 lament that among psychotherapy supervisors, “a comprehensive psychodynamic formulation is seldom offered and almost never incorporated into the written record” (p. 543).
One reason that case formulation skills have not been more studied may be a lack of consensus as to what a case formulation should contain and what its structure and goals should be. For example, in 1966 Seitz9 found that a group of psychoanalysts showed little agreement in the structure and content of formulations they constructed using the same clinical material. This explanation has less currency today, however, because several systematic methods for constructing case formulations have been developed in recent years. These case formulation construction methods have been developed within several psychotherapy orientations, including psychodynamic,10–14 cognitive-behavioral,15 interpersonal,16 behavioral,17,18 and blends of orientations.19,20 Most share three features:
They emphasize levels of inference that can readily be supported by a patient's statements in therapy.
The information they contain is based largely on clinical judgment rather than patient self-report.
The case formulation is compartmentalized into preset components that are addressed individually in the formulation process and then assembled into a comprehensive formulation.
A number of newer psychodynamic case formulation methods have good reliability and validity, according to Barber and Crits-Christoph's21 review of them. Separate components of Luborsky's Core Conflictual Relationship Theme (CCRT) method, for example, had a mean weighted kappa coefficient in the range of 0.61 to 0.70. Similarly, Curtis et al.22 report intraclass correlation coefficients ranging from 0.78 to 0.90 for components of their Plan Diagnosis Method.
Validity studies have focused on how well adherence to a case formulation predicts psychotherapy process and outcome. Crits-Christoph et al.23 showed that the accuracy of therapist interventions, as defined by adherence to reliably constructed CCRTs, correlated positively with residual gain in psychological adjustment in a group of 43 patients undergoing psychodynamic psychotherapy. Similarly, researchers at the Mount Zion Psychotherapy Group demonstrated that formulation-consistent interventions are associated with a deeper level of experiencing in patients, as compared with interventions that do not adhere to a formulation.24,25 A review of the behavioral and cognitive-behavioral literature by Persons and Tompkins15 showed more equivocal findings as to the association between individualized case formulations and treatment outcome.
Although encouraging, these developments in case formulation research should be viewed in the light of certain limitations.
The evidence for interrater reliability in many of the studies was based on relatively small samples.
Most of the studies were done by developers of the methods, which may have introduced subtle biases in favor of higher reliability.
The content of a case formulation appears to be greatly dependent on its guiding theory. Collins and Messer26 showed that two psychotherapy research teams using the same case formulation method, but guided by different theoretical orientations (Joseph Weiss's cognitive-analytic theory27,28 and Fairbairnian object relations theory), independently constructed formulations that were highly reliable as measured within each research team but widely divergent in content when cross-team comparisons were made.
There is evidence that therapist adherence to an initial formulation in brief dynamic therapy may predict a good outcome only for individuals with interpersonal relationships that are of relatively good quality, and may predict a poor outcome for individuals with low-quality interpersonal relationships.29 McWilliams2 and Eells30 discuss other caveats about case formulation.
Although the case formulation construction methods mentioned above have not led to a consensus on what the content, structure, and goals of a case formulation should be, and regardless of their limitations, they do provide guidelines that can facilitate the evaluation of case formulations.
The purpose of this study is to extend our knowledge of how clinicians use their case formulation skills in daily practice. We first pre-sent a multitheoretical system we developed to evaluate the content of written case formulations. The system was guided by the case formulation construction methods just described. Second, we demonstrate the application of the system to a set of case formulations as they appeared in intake evaluations at an outpatient mental health services clinic.
The CFCCM
The primary purpose of the Case Formulation Content Coding Method (CFCCM) is to provide a tool for reliably and comprehensively categorizing the information that a clinician uses in conceptualizing a patient. Provisions are also included for rating the quality of the formulation. The CFCCM was initially designed to provide a means for coding and comparing the “Case Formulation” and “Treatment Goals and Plan” sections that are usually part of intake evaluations, but it can also be applied to audio-recorded case formulations, narrative case formulations specifically constructed for research purposes, or similar materials.
In constructing the CFCCM we assumed that the primary function of a case formulation is to integrate rather than summarize descriptive information about the patient. We broadly defined a case formulation as a hypothesis about the causes, precipitants, and maintaining influences of a person's psychological, interpersonal, and behavioral problems. The approach views a case formulation as a tool that can help organize complex and contradictory information about a person. Further, it can serve as a blueprint guiding treatment, as a marker for change, and as a structure facilitating the therapist's understanding of and empathy for the patient. This definition is consistent with the newer formulation models reviewed earlier, and it contrasts with the view of some that a formulation is primarily a summary of descriptive information.31,32
A major goal in developing the CFCCM was to make it applicable across several approaches to psychotherapy. Toward this end, we reviewed the case formulation construction methods mentioned earlier, as well as other writings on case formulation, and identified four broad categories of information that are contained in most methods:
Symptoms and problems.
Precipitating stressors or events.
Predisposing life events or stressors.
A mechanism that links the preceding categories together and offers an explanation of the precipitants and maintaining influences of the individual's problems.
Although these categories are consistent with a medical model for treating mental disorders, they were chosen to be theoretically neutral and to provide a structure into which information generated within any theoretical perspective on formulation could be organized. We will first describe the content categories of the CFCCM, then discuss the quality ratings.
Content Categories of the CFCCM
Each content category is given one of three codes: absent, somewhat present, and clearly present. Each piece of information in the formulation is coded under only one category.
Symptoms and Problems:
The first common factor is the identification of signs, symptoms, and other phenomena that may be important clinically. This category incorporates the patient's presenting symptoms and chief complaints as well as problems that may be apparent to the clinician, but not to the patient. As noted by Henry,33 a patient's problems, which Henry defines as discrepancies between perceived and desired states of affairs, may not be readily apparent in the patient's initial self-presentation and thus could require skilled interviewing to reveal.
Precipitating Stressors:
These are events that catalyze or exacerbate the person's current symptoms and problems. These events may be construed either as directly leading to the current problems or as increasing the severity of preexisting problems to a level of clinical significance. Examples: recent divorce or relationship breakup, physical injury, illness, loss of social support, and occupational setback.
Predisposing Life Events:
These are traumatic events or stressors that have occurred in the person's past and that are assumed to have produced an increased vulnerability to developing symptoms. We separated these into three categories: early life (childhood and adolescence), past adulthood, and recent adulthood. We arbitrarily set a cutoff for recent adult stressors as within 2 years of the date the patient is currently being seen.
Inferred Mechanism:
This factor, the most important, represents an attempt to link together and explain information in the preceding three categories. The inferred mechanism is the clinician's hypothesis of the cause of the person's current difficulties. There are three major categories under inferred mechanism: psychological, biological, and sociocultural. Psychological mechanisms may include a core conflict; a set of dysfunctional thoughts, beliefs, or schemas; skills or behavioral deficits; problematic aspects or traits of the self; problematic aspects of relatedness to others; defense mechanisms or coping style; and problems with affect regulation. Biological mechanisms refer to both genetic and acquired conditions that cause or contribute to the patient's problems. Examples include a genetic predisposition for depression, a depression associated with hypothyroidism, or a presumed constitutional predisposition toward anxiety. Sociocultural mechanisms are factors such as ethnicity, socioeconomic status, religious beliefs, degree of acculturation, and absence of social support. A separate mechanism was included for substance abuse or dependency, since it spans the other categories.
Other Content Categories:
In addition to the four major categories just reviewed, the CFCCM includes content categories for positive treatment indicators such as strengths and adaptive skills; the clinician's treatment expectations; inferences as to the patient's overall level of adjustment; negative treatment indicators; and several categories of descriptive information such as past history of mental health care, developmental history, social or educational history, medical history, and mental status.
Quality Ratings in the CFCCM
In addition to examining the content categories listed above, the CFCCM includes quality ratings for the formulation as a whole, for each major subcategory (symptoms, predisposing life events, precipitating factors, and mechanism), and for the complexity of the formulation, the degree of inference used, and the precision of language. (The latter three categories were adapted from Strupp.34)
Complexity:
This refers to the degree to which the formulation takes into account several facets of the person's current problems and integrates these facets into a meaningful account. This dimension was rated on a five-point scale (1 = simple, 5 = complex).
Degree of Inference:
This is the extent to which the formulation goes beyond descriptive information offered by the patient. On a five-point scale (1 = descriptive, 5 = highly inferential), the formulation is rated low if it includes almost exclusively descriptive information, and it is given a higher rating as it contains increasingly more hypothetical considerations. In the development of the scale we were guided by Henry and colleagues'35 distinction between observable phenomena about a patient and assumptions about that patient's “deep structure.”
Precision of Language:
This category refers to the extent to which the language used in the formulation appears tailored to a specific individual or is more generic in nature. This was rated on a five-point scale (1 = general, 5 = precise).
Aims of the Study
We conducted an exploratory investigation intended to
Gather initial reliability data on the CFCCM.
Examine whether the categories are sufficiently broad and inclusive.
Assess the comprehensiveness and quality of a set of representative written case formulations.
Methods
Fifty-six intake reports at an inner-city outpatient psychiatry clinic were randomly selected from a pool of approximately 300, and their content was analyzed by using the CFCCM. Two advanced clinical psychology graduate students performed the coding on the 56 selected intake reports after independently coding and achieving consensus on a set of practice intake reports.
The interviewers were 9 psychiatry residents, 4 social workers, and 1 psychiatric nurse. The intake reports were written as part of the interviewers' typical clinical duties. Six of the 14 identified their primary orientation to psychotherapy as psychodynamic, 3 as cognitive-behavioral, 2 as a blend of psychodynamic and existential, and 1 as a blend of psychodynamic, cognitive-behavioral, and humanistic. Two did not respond to a questionnaire addressing orientation.
Patients
The 56 patients were representative of those seen in the clinic. The mean age was 40.0 years (range 20–66), and most were women (n20= 37; 66.1%). Forty-six (82.1%) were Caucasian, and 10 (17.9%) were African American. Eighteen (32.1%) were single, 17 (30.4%) were divorced, 11 (19.6%) were married, and the remainder were separated (n = 6; 10.7%), widowed (n = 2; 3.6%), or living with a significant other (n = 2; 3.6%). Most were high school educated (mean years of education = 11.4, range 4—16 years) but unemployed (n = 31, 55.4%). Fifteen (26.8%) were employed, 8 (14.3%) were on disability, and 2 (3.6%) were retired.
Results
Reliability
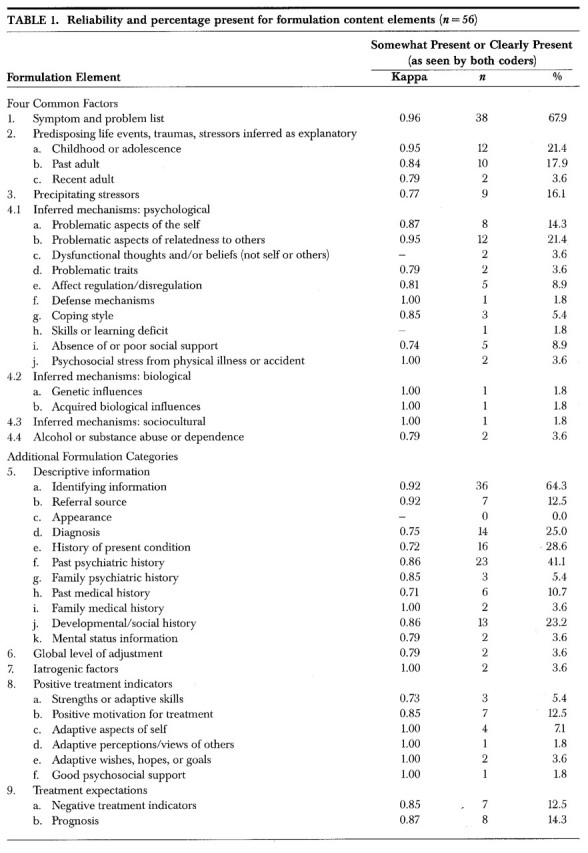
The mean kappa coefficient36 for both content and quality categories of the CFCCM was 0.86, with a range from 0.67 to 1.0. In computing reliability for the content categories, we collapsed “somewhat present” and “clearly present” into one category, leaving “not present” and “present” as the categories evaluated. Table 1 summarizes the reliability coefficients for each content category. The mean kappa for these items was 0.88. Kappa coefficients for the quality ratings of the four common factors were 0.79, 0.88, 0.83, and 0.74, respectively, for symptoms/problems, precipitating stressors, predisposing life events, and inferred mechanisms. The kappa for the ratings of the overall quality of the formulation was 0.70. Complexity, degree of inference, and precision of language had kappas of 0.82, 0.67, and 0.77, respectively. Overall, these data indicate good reliability across the CFCCM categories.
TABLE 1.
Content Categories
Table 1 summarizes the numbers and percentages of case formulations in which each formulation element was judged as somewhat present or clearly present by both coders. Descriptive information was presented in 94.6% (n = 53) of the formulations. The descriptive categories most frequently mentioned were symptoms/problem list (67.9%; n = 38), identifying information (64.3%; n = 36), and past psychiatric history (41.1%; n = 23). Only 37.5% (n = 21) included a predisposing life event inferred as contributing to a patient's problems. Only about one-fifth (21.4%; n = 12) of the formulations contained references to childhood or adolescent events, 17.9% (n = 10) dealt with past adult events, and 3.6% (n = 2) referred to recent adult events. A precipitating stressor was considered in only 16.1% (n = 9) of the formulations. A minority inferred a mechanism as contributing to the individual's problems: 42.9% (n = 24) inferred a psychological mechanism, 1.8% (n = 1) inferred a biological mechanism, and 1.8% inferred a social or cultural mechanism. In addition, only 21.4% (n = 12) inferred a positive treatment indicator. In sum, the formulation section of the intake evaluations was dominated by descriptive information with a primary focus on symptoms and past psychiatric history.
Formulation Quality Categories
In addition to assessing whether each of the four “common factors” was present, it seemed important to measure the quality of its presentation. Therefore, we developed a five-point scale, with verbal anchors as follows: 1 = not present, 2 = rudimentary presentation, 3 = adequate presentation, 4 = good presentation, and 5 = excellent presentation. As shown in Table 2, ratings are predominantly in the “not present,” “rudimentary,” or “adequate” categories.
TABLE 2.

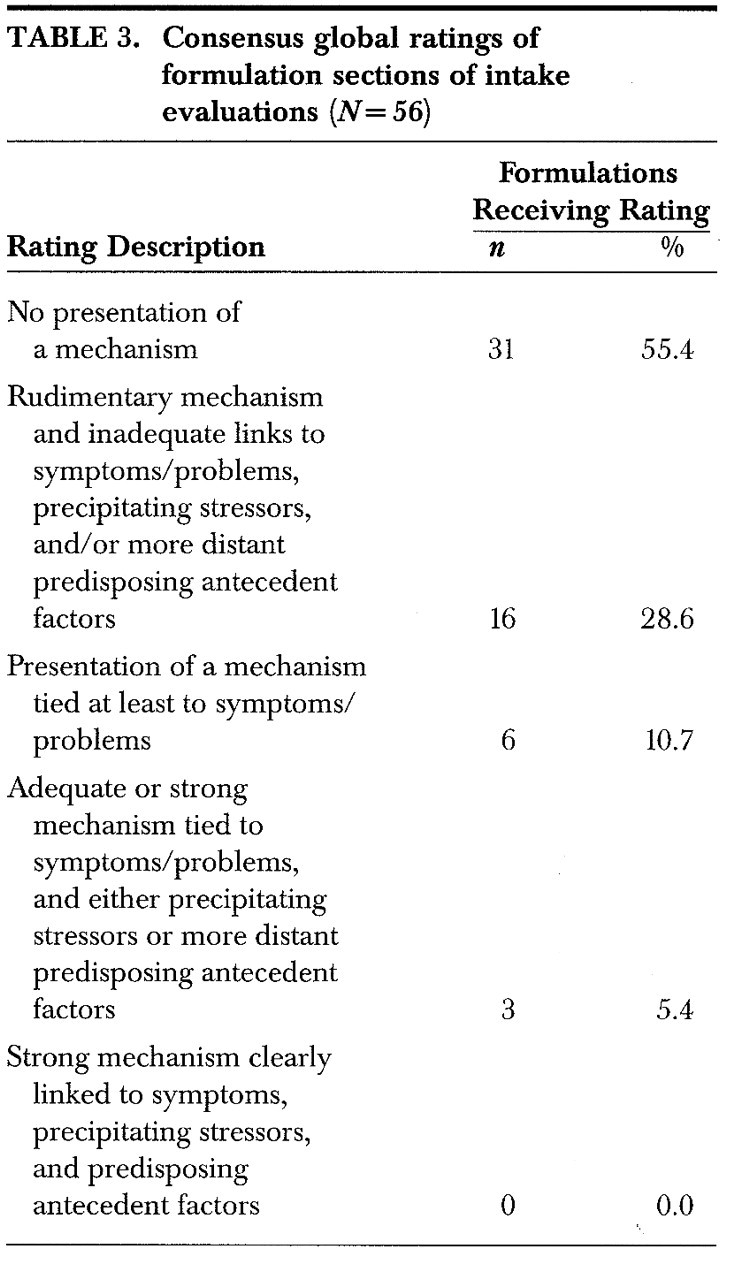
Consensus global ratings of the formulations appear in Table 3. As shown, 31 of the 56 formulations (55.4%) contained no presentation of a mechanism; 16 (28.6%) contained a mechanism that was described as rudimentary, with little attention given to how the mechanism is linked to symptoms, problems, precipitating stressors, or other predisposing life events. Only 3 formulations (5.4%) were rated as having adequate to strong mechanisms.
TABLE 3.
Complexity:
The mean complexity rating on the scale of 1 (simple) to 5 (complex) was 2.05 (SD = 0.94), indicating that the formulations were rated as relatively simple, with little evidence of interweaving and integrating of different types of information.
Degree of Inference:
The inference ratings indicate that the formulations contained primarily descriptive information and little inference. On the scale of 1 (descriptive) to 5 (highly inferential), mean inference ratings were 1.80 (SD = 0.77). Of the 56 formulations rated, 23 (41.1%) were consensually rated at the most descriptive end of the scale; 21 (37.5%) were rated “2”; and the remaining 12 (21.4%) were rated “3.”
Precision of Language:
The formulations were rated as moderately precise in terms of the language used. The mean precision rating was 2.57 (SD = 0.93) on the scale of 1 (general) to 5 (precise).
Discussion
This naturalistic study has a number of limitations. First, a written case formulation may not accurately or completely depict the therapist's understanding of the patient. Second, despite the consensus that case formulation skills are important, little is known about the relationship between case formulation skill and treatment efficacy. A poorly written case formulation may not predict poor psychotherapy outcome. Further, the effectiveness of therapists with good case formulation skills may be due to skills other than those related to case formulation. Third, the case formulations we evaluated were typically dictated after a single intake session with the patient. This may not have provided enough time for an adequate database to be collected. Fourth, the clinicians may not have used the case formulation skills that they have. In that sense, the study is better viewed as an investigation of representative written case formulations rather than as a clinician's best possible work.
Despite these considerations, this first study of case formulation skills in a naturalistic context showed that the CFCCM can be reliably scored and can measure an adequate range of information contained in a case formulation. The findings showed that the clinicians did not consistently use the formulation section to offer hypotheses about a patient's symptoms or to integrate previously presented descriptive information. Instead, they used the formulation primarily to summarize descriptive information. Our findings provide empirical support for surveys suggesting that case formulation is an insufficiently taught skill.6,7
What are the implications of these findings? Three seem central:
There is a need for more training in formulation. The availability of newer, empirically supported case formulation models should facilitate this training.37
The relationship between case formulation and treatment outcome should be studied further. Designs for doing so have been offered by Hayes et al.38 and by Persons.39 Such studies could help document the incremental validity of formulation: whether individualized formulations lead to better therapy processes and outcomes than do generic formulations or the absence of an explicit formulation. They could also advance our understanding of specific therapist skills that lead to positive treatment outcomes.
The relationship between formulation and treatment plans and goals deserves study. One hypothesis would be that a suitably comprehensive, complex, and objective formulation that “fits” the patient well facilitates better articulated and more attainable treatment plans and goals. Another would be that a good formulation helps the therapist anticipate and manage events that could hinder or prevent treatment success.
Acknowledgments
An earlier version of this work was presented at the 27th meeting of the Society of Psychotherapy Research, Amelia Island, FL, June 1996. Interested readers may obtain a copy of the CFCCM from the first author at the address shown in the headnote to this article.
References
- 1.Faulkner LR, Kinzie JD, Angell R, et al: A comprehensive psychiatric formulation model. Journal of Psychiatric Education 1985; 9:189–203 [Google Scholar]
- 2.McWilliams N: Psychoanalytic Diagnosis: Understanding Personality Structure in the Clinical Process. New York, Guilford, 1994
- 3.Sperry L, Gudeman JE, Blackwell B, et al: Psychiatric Case Formulations. Washington, DC, American Psychiatric Press, 1992
- 4.Persons JB: Advantages of studying psychological phenomena rather than psychiatric diagnoses. Am Psychol 1986; 41:1252–1260 [DOI] [PubMed] [Google Scholar]
- 5.Levenson H: Time-Limited Dynamic Psychotherapy: A Guide to Clinical Practice. New York, Basic Books, 1995
- 6.Fleming JA, Patterson PG: The teaching of case formulation in Canada. Can J Psychiatry 1993; 38:345–350 [DOI] [PubMed] [Google Scholar]
- 7.Ben-Aron M, McCormick WO: The teaching of formulation: facts and deficiencies. Can J Psychiatry 1980; 25:163–166 [DOI] [PubMed] [Google Scholar]
- 8.Perry S, Cooper AM, Michels R: The psychodynamic formulation: its purpose, structure and clinical application. Am J Psychiatry 1987; 144:543–550 [DOI] [PubMed] [Google Scholar]
- 9.Seitz PF: The consensus problem in psychoanalytic research, in Methods of Research and Psychotherapy, edited by Gottschalk L, Auerbach L. New York, Appleton-Century Crofts, 1966, pp 209–225
- 10.Curtis JL, Silberschatz G: Plan formulation method, in Handbook of Psychotherapy Case Formulation, edited by Eells TD. New York, Guilford, 1997, pp 116–136
- 11. Horowitz MJ: Formulation as a Basis for Planning Psychotherapy Treatment. Washington, DC, American Psychiatric Press, 1997
- 12.Levenson H, Strupp HH: Cyclical maladaptive patterns: case formulation in time-limited dynamic psychotherapy, in Handbook of Psychotherapy Case Formulation, edited by Eells TD. New York, Guilford, 1997, pp 84–115
- 13.Luborsky L: The core conflictual relationship theme: a basic case formulation method, in Handbook of Psychotherapy Case Formulation, edited by Eells TD. New York, Guilford, 1997, pp 58–83
- 14.Perry JC: The idiographic conflict formulation method, in Handbook of Psychotherapy Case Formulation, edited by Eells TD. New York, Guilford, 1997, pp 137–165
- 15.Persons JB, Tompkins M: Cognitive-behavioral case formulation, in Handbook of Psychotherapy Case Formulation, edited by Eells TD. New York, Guilford, 1997, pp 314–339
- 16.Markowitz JC, Swartz HA: Case formulation in interpersonal psychotherapy of depression, in Handbook of Psychotherapy Case Formulation, edited by Eells TD. New York, Guilford, 1997, pp 192–222
- 17.Nezu AM, Nezu CM, Friedman SH, et al: Case formulation in behavior therapy: problem-solving and functional-analytic strategies, in Handbook of Psychotherapy Case Formulation, edited by Eells TD. New York, Guilford, 1997, pp 368–401
- 18.Koerner K, Linehan MM: Case formulation in dialectical behavior therapy for borderline personality disorder, in Handbook of Psychotherapy Case Formulation, edited by Eells TD. New York, Guilford, 1997, pp 340–368
- 19.Caspar F: Plan Analysis: Toward Optimizing Psychotherapy. Seattle, WA, Hogrefe and Huber, 1995
- 20.Ryle A, Bennett D: Case formulation in cognitive analytic therapy, in Handbook of Psychotherapy Case Formulation, edited by Eells TD. New York, Guilford, 1997, pp 289–313
- 21.Barber JP, Crits-Christoph P: Advances in measures of psychodynamic formulations. J Consult Clin Psychol 1993; 61:574–585 [PubMed] [Google Scholar]
- 22.Curtis JT, Silberschatz G, Sampson H, et al: Developing reliable psychodynamic case formulation: an illustration of the Plan Diagnosis method. Psychotherapy 1988; 25:256–265 [Google Scholar]
- 23.Crits-Christoph P, Cooper A, Luborsky L: The accuracy of therapists' interpretations and the outcome of dynamic psychotherapy. J Consult Clin Psychol 1988; 56:490–495 [DOI] [PubMed] [Google Scholar]
- 24.Silberschatz G, Fretter PB, Curtis JT: How do interpretations influence the process of psychotherapy? J Consult Clin Psychol 1986; 54:646–652 [DOI] [PubMed] [Google Scholar]
- 25.Silberschatz G, Curtis JT: Measuring the therapist's impact on the patient's therapeutic progress. J Consult Clin Psychol 1993; 61:403–411 [DOI] [PubMed] [Google Scholar]
- 26.Collins WD, Messer SB: Extending the Plan Formulation Method to an object relations perspective: reliability, stability, and adaptability. Psychological Assessment 1991; 3:75–81 [Google Scholar]
- 27.Weiss J: How Psychotherapy Works: Process and Technique. New York, Guilford, 1993
- 28.Weiss J, Sampson H: The Psychoanalytic Process: Theory, Clinical Observation, and Empirical Research. New York, Guilford, 1986
- 29.H<179>glend P, Piper WE: Focal adherence in brief dynamic psychotherapy: a comparison of findings from two independent studies. Psychotherapy 1995; 32:618–628 [Google Scholar]
- 30.Eells TD: Psychotherapy case formulation: history and current status, in Handbook of Psychotherapy Case Formulation, edited by Eells TD. New York, Guilford, 1997, pp 1–25
- 31.Loganbill C, Stoltenberg C: The case conceptualization format: a training device for practicum. Counselor Education and Supervision 1983; 22:235–241 [Google Scholar]
- 32.Weerasekera P: Formulation: a multiperspective model. Can J Psychiatry 1993; 38:351–358 [DOI] [PubMed] [Google Scholar]
- 33.Henry WP: Interpersonal case formulation: describing and explaining interpersonal patterns using the Structural Analysis of Social Behavior, in Handbook of Psychotherapy Case Formulation, edited by Eells TD. New York, Guilford, 1997, pp 223–259
- 34.Strupp HH: The psychotherapist's contribution to the treatment process. Behav Sci 1958; 3:43–67 [Google Scholar]
- 35.Henry WP, Strupp HH, Schacht TE, et al: Psychodynamic approaches, in Handbook of Psychotherapy and Behavior Change, edited by Bergin AE, Garfield SL. New York, Wiley, 1994, pp 467–508
- 36.Cohen JA: A coefficient of agreement for nominal scales. Educational and Psychological Measurement 1960; 20:37–46 [Google Scholar]
- 37.Eells TD (ed): Handbook of Psychotherapy Case Formulation. New York, Guilford, 1997
- 38.Hayes SC, Nelson RO, Jarrett RB: The treatment utility of assessment: a functional approach to evaluating assessment quality. Am Psychol 1987; 42:963–974 [DOI] [PubMed] [Google Scholar]
- 39.Persons JB: Psychotherapy outcome studies do not accurately represent current models of psychotherapy: a proposed remedy. Am Psychol 1991; 46:99–106 [DOI] [PubMed] [Google Scholar]