

Abstract
Background:
Students are pivotal to manpower development and technological advancement of any nation. Nigerian nation was recently ranked third human immunodeficiency virus (HIV) most endemic nation in the world
Aim:
The study was designed to determine the frequency of HIV infection among Nigerian tertiary and secondary institution students.
Materials and Methods:
A HIV screening test was conducted on 1,978 apparently healthy students composed of 981 males and 997 females aged 11–35 years, randomly selected from some Nigerian tertiary and secondary institutions
Results:
Overall, the sero-prevalence rate of 13.7% was recorded consisting 9.9% in the tertiary and 3.8% in secondary institutions. The distribution of the infection showed no significant difference by age (χ2=1.07, P>0.05) and by gender (χ2=0.85, P>0.05). Also, the prevalence had no significant association with the settlement of students (χ2=0.96, P>0.05) and the status of educational institutions (χ2=1.42, P>0.05).
Conclusion:
The findings indicate a high HIV prevalence rate among students in this part of the globe. General behavioral changes about sex among the students are suggested.
Keywords: Educational-institutions endemic-state, Frequency, Human immunodeficiency virus, Students
Introduction
Human immunodeficiency virus (HIV) infection and acquired immune deficiency syndrome (AIDS) affect all aspects of human endeavors as they cut across age, gender, race, socio-political status, education, relation, ethnic, culture, and barriers of any kind. As in 2005, about 43 million have been infected with the dreaded virus while over 25 million have died of the infection world-wide.[1] It has also been reported that over 60% of the global HIV/AIDS cases are concentrated in Africa.[2] In Nigeria, it has been reported that at least 10,000 youths are infected monthly,[1] while the HIV prevalence rate as in 2008 was 5.0%. Similarly, in the same year, the prevalence rate in Adamawa State was 4.6%.[3] The infection has now assumed an astronomical dimension world-wide, hence described as pandemic rather than being an epidemic.[4,5]
Ordinarily, students are expected to be among the low-risk groups.[6] However, because of the considerable complacency among them about HIV and its mode of infection as earlier documented,[7–9] the group is now tending toward high risk. The risky behaviors of some students in some parts of the world have been reported in many studies.[10–18] This, therefore, calls for a serious attention to ascertain the extent of the infection among them. In view of devastating impact of HIV infection on African economy, it was recommended[19] that for proper resource allocation, the epidemiological study of the infection is very essential, especially with particular reference to youths and demographic influence.
Youth, a group ranging from 15 to 24 years, occupies a prominent position in the economy of any nation as they are often regarded as future leaders. Many of the members in this group are either in the institutions of learning or undergoing vocational training. Some reports[12,13] have shown that immoral and risky sexual behaviors are common among sexually mature and active students. This study reports the prevalence of HIV infection among students in some tertiary and secondary institutions in Nigeria.
Materials and Methods
Selection of subjects
A total of 1978 apparently healthy students aged 11–35 years composed of 981 males and 997 females were randomly sampled in three geographical zones (North, South, and Central) of Adamawa State in North-Eastern Nigeria between September 2008 and August 2009.
The subjects were those attending Federal Medical Center, Specialist Hospital, General Hospitals in Ganye, Mubi, Garkida, and Numan. Others were subjects attending Kowa Hospital, Peace Hospital, Adamawa Hospital, Yola Biomedics Laboratories, and Health Centers in Tola, Pella and Fufore. They were apparently healthy seeking medical check-up for job recruitment, admissions, and blood donation. They also included some healthy students attending HIV voluntary counseling and testing clinics. Prior to the commencement of the study approval from Research and Ethics Committee of the State Ministry of Health was obtained in accordance with the Helsinki Declaration guidelines. Also, informed consent of the participants was sought and obtained in writing before volunteers were enrolled in the study.
Specimen collection and laboratory analysis
After proper sterilization of the antecubital fossa of the arm with swab of methylated spirit, 5 ml of blood was collected from each of the students by vein puncture and put in a plain tube, held at room temperature for about 20 minutes and spun to remove the serum needed for HIV antibodies tying. A Capillus HIV kit (Trinity Biotech, UK) was used for the HIV antibodies detection while a Determine (Abbot, Japan) HIV kit was used to confirm initial-positive cases. Only concordant positive results were recorded and considered for the study. Manufactures’ procedures for HIV testing were strictly followed. Both positive and negative control specimens were included and run concurrently with the test samples to ascertain the reliability of the screening kits used. In-depth interview was also conducted with each student for information on educational institutions, settlement, and age.
Statistical analysis
Data obtained from the tests were entered and analyzed using SPSS Version 16 software of computer (SPSS Inc., USA). The test of significance was performed using chi-square for HIV sero-prevalence with respect to educational institution category, settlement of the institutions, age, and gender of the subjects. The statistical difference was interpreted based on 95% confidence level (P=0.05).
Results
Overall, the sero-prevalence rate of 13.7% was recorded consisting 9.9% in the tertiary and 3.8% in secondary institutions. The distribution of the infection showed no significant difference by age (χ2=1.07, P>0.05) and by gender (χ2=0.85, P>0.05). Also, the prevalence had no significant association with the settlement of students (χ2=0.96, P>0.05) and the status of educational institutions (χ2=1.42, P>0.05).
The findings from the study were expressed in percentages and presented in Tables 1–3 as shown below.
Table 1.
Geographical distribution of HIV infection among students in tertiary and secondary institutions

Table 3.
Prevalence of HIV infection among students in relation to age and gender
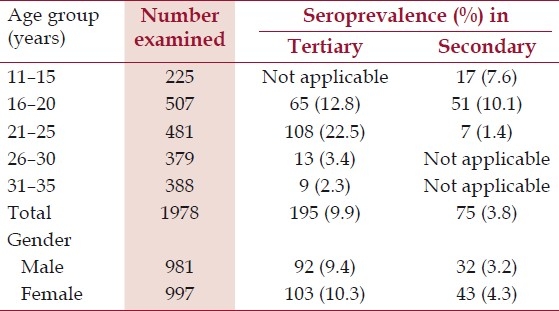
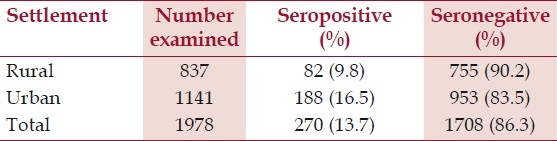
Table 2.
Prevalence of HIV infection among students by educational settlement
Discussion
Students are often regarded as future leaders of any nation considering their pivotal position in manpower development, socioeconomic, political, and technological advancement of a nation. However, many students and indeed some citizens of African countries are still reluctant to acknowledge the spread of HIV pandemic owing to their social and cultural norms. HIV infection is no more a news all over the world, what seems new now judging from this present study is that students are tending toward being among the “high risk groups.”
The findings in this study revealed an amazing prevalence rate of 13.7% consisting of 9.9% among the students of tertiary institutions and 3.8% from those in secondary schools. Meanwhile, there is a possibility that the HIV prevalence could still be higher than these findings because some subjects may be in the window period.[20,21]
In addition to some risky sexual behaviors, unhealthy and unhygienic living in the hostels which include sharing of shaving blade, clippers, and toothbrushes could also contribute to the high prevalence of the virus among students. Similarly keeping multiple sex partners, youthful exuberance, complacency, economic hardship, and some immoral social activities on the campus such as gala night, beauty contests, disco parties, and watching pornographic films, all could enhance risky sexual behaviors and consequently resulting to high rate of infection. Students that are involved in taking hard drugs have higher risk of being infected than nonusers.[22] These social vices are found among many students of higher learning especially in tertiary institutions and they could explain why the infection rate in this study is higher in tertiary institutions (9.9%) than in secondary schools (3.8%). However, statistical analysis by chi-square showed no significant difference in the prevalence of the infection in secondary and tertiary institutions (χ2=1.42, P>0.05).
Judging the prevalence of the infection by the settlement of students, a higher rate (16.5%) was recorded in the urban centers than those in rural settlement with 9.8%. Statistically, there was no significant difference in the distribution of the infected students with respect to institutions’ settlement (χ2=0.96, P>0.05). However, the slight variation in findings among students from rural and urban institutions could be attributed to nonuniformity in the number examined.
Age-related prevalence of HIV infections among students examined showed a highest rate (22.5%) within the 21–25 years age bracket while the least (2.3%) was recorded within 31–35 years’ age group. Progression from adolescent to early adulthood is usually accompanied by hormonal, emotional, and physical changes which usually result to high sexual activities in early years of puberty. This could explain the high rate of infection within the age group 21–25 years. Also, younger and matured females of this age bracket are often preferred to older ones by male sex partners. Consequently, the group is more exposed and more vulnerable to sexually transmitted infection than the older group. This finding is in consonance with result of previous studies[22,23] that reported similar observation. Statistical analysis by the chi-square test however showed no significant difference in the prevalence of the infection by age (χ2=1.07, P>0.05). Similarly, by gender consideration, the females recorded a higher rate (10.3%) than the male counterpart (9.4%). This variation in findings could be attributed to difference in the anatomical structure of the female genital tract that makes them more vulnerable to genital infection. Poverty and violence, against young females, are also some factors that could probably predispose them to infection.[23] This result agrees with the findings from similar studies[24,25] that also reported a higher HIV rates among females than males but disagrees with report of Center for Disease Control which documented higher rate in males than females.[26]
From the present findings, it is obvious that the HIV prevalence rate among students in this part of the globe is still high, and if allowed to spread further, it could be a serious threat to the nation's economy in the nearest future considering the impact of skilled manpower in national development. General behavioral change about sex is very paramount. A situation whereby over 50% Nigerian girls have had sex even before their first menstruation[27] should be discouraged in totality.
In the past, attempts to provide sex education for young people were hindered by cultural and religious insinuations. However, with the increasing rate of the infection among youths it has become very necessary to legislate the development of new academic curriculum that will take into consideration sex education at all levels in Nigeria, Africa, and even the world at large. Adequate consultation with religious, traditional, and community leaders is very essential for the success of this arrangement. HIV screening should be made mandatory before admission is given by any educational institution. Finally, since several studies[28–30] have associated high rate of HIV with other common sexually transmitted infections, epidemiological studies of such infections should be carried out among students as part of control measures toward reducing the spread of the dreaded virus among them.
Conclusion
The prevalence of HIV among the studied student population is high and worrisome. There is need to intensify more effort on HIV prevention strategy especially among students. General behavioral changes about sex among them are also suggested.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
References
- 1.Richard CO. 1st ed. Port-Harcourt, Nigeria: Finejob Publications; 2006. The untold origin of HIV/Aids and lies about condom; pp. 1–61. [Google Scholar]
- 2.UNAIDS. Epidemiology of HIV/AIDS in Africa 2003, UNAIDS/HIV/AIDS/03 document [Google Scholar]
- 3.FMOH. Republic of Nigeria, National HIV sentinel surveillance 2005 Federal Ministry of Health Expert Committee Report Series. 2006 [Google Scholar]
- 4.CDC. The global HIV and AIDS epidemic. Morb Mortal Wkly Rep. 2001;50:434–9. [PubMed] [Google Scholar]
- 5.CDC. Update AIDS in United State. Morb Mortal Wkly Rep. 2002;51:592–5. [PubMed] [Google Scholar]
- 6.Okechi OO, Apuaka FC, Ekpo Bo. HIV Seropositive cases among undergraduates in institutions of higher learning in Abia and Imo States, Nigeria. Niger Biomed Sci J. 2005;1:131–3. [Google Scholar]
- 7.Thomas SB, Gilliam AG, Iwey CG. Knowledge about AIDS and reported risk behaviours among black college students. J Am Coll Health. 1989;38:61–6. doi: 10.1080/07448481.1989.9938417. [DOI] [PubMed] [Google Scholar]
- 8.Manning D, Balson DM, Barenberg N, Moore TM. Susceptibility to AIDS: Students Knowledge and attributes at a mid-western university. J Am Coll Health. 1988;36:214–22. [Google Scholar]
- 9.Landefeld CS, Chren MM, Shega J, Speroof T. Mcciure Students’ sexual behaviour knowledge and Immunodeficiency Syndrome. J Gen Intern Med. 1988;3:161–5. doi: 10.1007/BF02596125. [DOI] [PubMed] [Google Scholar]
- 10.Sexually transmitted Diseases statistics, 1987 No. 136, Atlanta Centers for Disease control. 1988:1–58. [Google Scholar]
- 11.Mascola L, Albritton WL, Cates WJ, Reyolds GH. Gonorrhea in American teenagers 1980-1981. Pediatr Infect Dis. 1983;2:302–3. doi: 10.1097/00006454-198307000-00010. [DOI] [PubMed] [Google Scholar]
- 12.Leslie-Harwih M, Meheus A. Sexually transmitted diseases in young people: The importance of health education. Sexually Transimtted Diseases. 1989;16:15–20. doi: 10.1097/00007435-198901000-00004. [DOI] [PubMed] [Google Scholar]
- 13.Armstein RL. Sex and anxiety on the campus: Thirty-five years thereof. J Am Coll Health. 1989;37:247–53. doi: 10.1080/07448481.1989.9937490. [DOI] [PubMed] [Google Scholar]
- 14.Delva MD, McSherry JA. Herpes genitalia in a student population. J Fam Pract. 1984;18:397–400. [PubMed] [Google Scholar]
- 15.Mccormack WM, Rosner B, McComb DE, Evrard JR, Zonner SH. Infection with Chlamydia trachomatis in female college students. Am J Epidemiol. 1985;121:107–15. doi: 10.1093/oxfordjournals.aje.a113971. [DOI] [PubMed] [Google Scholar]
- 16.Lee H. Genital Chlamydia infection in female and male college students. J Am Coll Health. 1989;37:288–91. doi: 10.1080/07448481.1989.9937497. [DOI] [PubMed] [Google Scholar]
- 17.Spear SF, Degar DK. Screening for Chlamydia by University Health centres. Is it necessary and feasible? J Am Coll Health. 1989;37:293–5. doi: 10.1080/07448481.1989.9937498. [DOI] [PubMed] [Google Scholar]
- 18.Earlie JR, Perricone PJ. Sexuality: A ten-year study of attitude and behaviour of a mall university company. J Sex Res. 1986;22:311–9. [Google Scholar]
- 19.Adisssa Abababa, Ethiopia: Publication of Economic Commission for Africa; 2004. CHGA. Socio-economic impacts of HIV/AIDS in Africa. [Google Scholar]
- 20.Aschwartz SA, Nair MP. Current concepts in Human Immunodeficency Virus Infectin and AIDS. Clin Diagn Lab Immunol. 1999;6:295–305. doi: 10.1128/cdli.6.3.295-305.1999. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Schrenher GB, Busch MP, Kleiman SH, Koretitz JJ. The risk of transfusion transmitted Viral infection.The retrovirus epidemiology: Donor study. N Engl J Med. 1996;334:1685–6. doi: 10.1056/NEJM199606273342601. [DOI] [PubMed] [Google Scholar]
- 22.National Intelligence Council. The next wave of HIV/AIDS in Nigeria, Ethopia Russia, India and China. Intelligence Community Assessment 202. 2000-04:4–27. [Google Scholar]
- 23.Abdulazeez A. A comparative study of trichomonas vaginalis and HIIV infections among women in Yola, Nigeria. Masters Degree Thesis, Federal University of Technology, Yola. 2005 [Google Scholar]
- 24.Msuga M, Mayand P, Mkanje R, Grosskurth H. Taking early action in emergencies to reduce the spread of STDs and HIV in Tanzania Amref. Afr Health. 1999;1:18–24. [PubMed] [Google Scholar]
- 25.Adomed DJ, Adeyemi O, Ezimah CU, Okoye RN, Usman HA, Goni HL. Multivariate assessment of sexually transmitted bacterial infection in Potiskum, Yobe state Nigeria. J Life Environ Sci. 2005;7:422–30. [Google Scholar]
- 26.Centre for disease control HIV/AIDS Surveillance report. 1990 Oct [Google Scholar]
- 27.Ukwandu CD, Kudi AA. Human immunodeficiency virus and sexually transmitted diseases. J Med Lab Sci. 2000;9:103–12. [Google Scholar]
- 28.WHO. Guidelines for the management of sexually transmitted infections. 2001 WHO/01 Document. [Google Scholar]
- 29.Allen S, Funnye MD, Abbasi J. Syphilis and Human Immunodeficiency virus co-infection. J Natl Med Assoc. 2003;95:263–82. [PMC free article] [PubMed] [Google Scholar]
- 30.Fleming DT, Wasserheit JN. From epidemiological synergy to public health policy and practice, the contribution of other sexually transmitted diseases to sexual transmission of HIV. Sex Transm Dis. 1999;23:433–40. doi: 10.1136/sti.75.1.3. [DOI] [PMC free article] [PubMed] [Google Scholar]