

Abstract
Background:
Otitis Media continues to be a major presentation in the ear, nose and throat clinic.
Aim:
This study aimed to isolate, characterize and identify the bacteriological and mycological etiologic agents of otitis media in Benin city.
Patients and Methods:
Ear discharge from 569 (299 males and 270 females) patients diagnosed clinically of otitis media between August 2009 and August 2010 were processed to recover the bacterial and fungal etiologic agents. Susceptibility test was performed on all bacterial isolate.
Result:
Pseudomonas aeruginosa (28.3%) was the predominant bacteria isolate causing otitis media followed by Staphylococcus aureus (21.0%), Klebsiella sp (8.9%), Proteus sp (8.2%), Alkaligenes spp (4.3%), Streptococcus pneumoniae (3.9%), Escherichia coli (3.0%) and Citrobacter freundi (1.7%). Fungi isolated were Aspergillus niger (9.2%), Candida albicans (5.4%), Candida tropicalis (3.0%), Aspergillus flavus (2.1%) and Candida parasilopsis (1.5%). 413 had a single organism isolated from the middle ear culture while twenty (3.51%) patients had mixed organisms isolated. Infection was highest among 0 - 5 years, and lowest among aged 18 - 23. All bacterial isolates were poorly susceptible to the antibacterial agents.
Conclusion:
The study uncovers a high frequency of bacteria associated otitis media with the finding of fungi too as a significant etiologic agent.
Keywords: Otitis media, etiologic agents, prevalence, Benin city
Introduction
Otitis Media (OM) is highly prevalent worldwide[1]. Otitis media is inflammation of the middle ear drum and the inner ear, including a duct known as the Eustachian tube[2]. Otitis media is very common in children[3]. Children below the age of seven years are much more susceptible to otitis media since the Eustachian tube is shorter and at more of a horizontal angle than in the adult and this is also because they have not developed the same resistance to bacteria, fungi and viruses as found in adults[4]. Exposure to smoke crowded living conditions and low socio-economic class are among the risk factor of otitis media[5].
Over 50 percent of the cases of otitis media are caused by bacteria[6]. Occasionally, otitis media may be caused by fungi, viruses, Mycoplasma pneumoniae and Chlamydia trachomatis[7]. A number of studies have reported on the prevalence of otitis media[5,8]. However, majority of these studies have focused on clinical diagnosis with little or no report on the bacteriological and mycological etiology of otitis media. There exists a dearth of knowledge on a study carried out in this area on the prevalence of otitis media incorporating bacteriological and mycological examination. Against this background, this study aimed to isolate, characterize and identify the bacteriological and mycological etiologic agents of otitis media in Benin City.
Patients and Methods
Benin City ‘The Cradle of Black civilization’ as it is popularly known, is an urban area and capital city of Edo state, southern Nigeria. The city is approximately 25miles north of the Benin River and situated 200miles by road east of Lagos. It is home to about 1,147188 million individuals[9], who are predominantly ‘Edo's’ with smaller population of other tribal groups from neighboring states. This study was carried out during the period August 2009-August 2010 in Benin City at the Ear, Nose and Throat Clinic in University of Benin Teaching Hospital, Benin City, Nigeria (UBTH). UBTH is a tertiary hospital with a referral status and serves the many private hospitals and government owned specialist hospitals in the state and neighboring states. Five hundred and sixty nine patients with clinical manifestations suggestive of Otitis Media (Discharging ears) (299 males and 270 females) were investigated. The age range of patients was (1 day - 70 years).
Collection of specimens
The samples were collected with sterile swab sticks which were properly labeled for each patient. The swab sticks were taken to the Medical Microbiology Laboratory, University of Benin Teaching Hospital for analysis, within 4 – 6 hours after collection.
Isolation of bacteria
Specimens were inoculated onto blood, chocolate and MacConkey agar plates. All plates were incubated for 24 hours aerobically with the exception of chocolate agar that was incubated in a candle jar. Emergent colonies were identified according to standard bacteriological methods[10]. Disc susceptibility test was performed according to National Committee for Clinical Laboratory Standards (NCCLS)[11].
Isolation of fungi
The swab sticks were streaked directly on the well labeled Sabouraud Dextrose Agar (SDA) plates and incubated at room temperature. The growth was identified based on their morphological and cultural characteristics and microscopic examination was done using lactophenol blue staining technique[12]. Germ tube method and clamidospore formation where used to differentiate Candida albicans from other species of Candida. API 20C (Biomerieux France) was also used for the speciation of Candida.
Statistical analysis
Data were analyzed using chi square (X2) test using the statistical software SPSS v 16.P value of less than 0.05 was considered significant.
Results
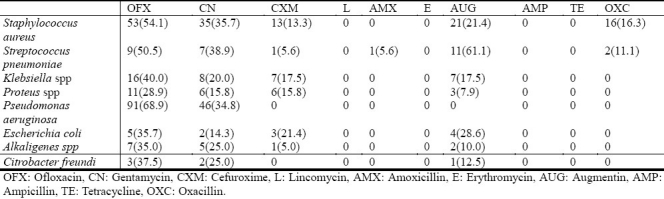
From the 569 patients enrolled in the study, there were 466 isolates. Four hundred and thirteen patients (72.6%) had a single organism isolated from the middle ear culture, while twenty (3.51%) patients had mixed organisms isolated. Pseudomonas aeruginosa was the most prevalent etiologic agent of otitis media while the least was Candida parasilopsis (Table I). Patients that were 5 years or younger had significantly higher prevalence of otitis media compared with other children and adults; but there was no significant difference in gender in the prevalence of otitis media (Table 2). The antibiotic susceptibility profile of the bacteria isolates revealed high level resistance (Table 3). Lincomycin, erythromycin, ampicillin and tetracycline were not active against any of the bacterial isolate.
Table 1.
Prevalence of bacterial and fungal etiologic agents of otitis media
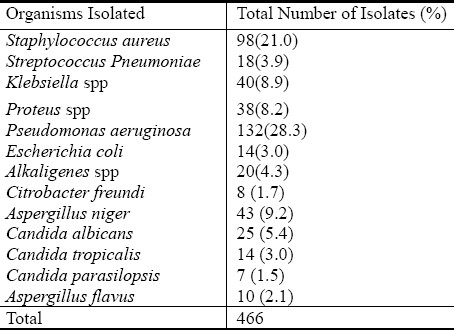
Table 2.
Gender and age related prevalence of etiologic agents of otitis media
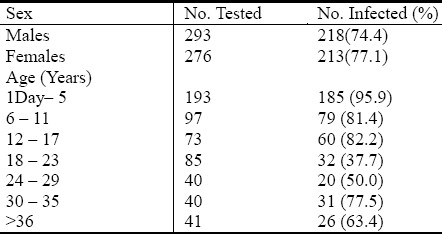
Table 3.
Antibiotic susceptibility profile of the bacterial isolates
Discussion
Otitis media is frequently encountered in tropical and subtropical areas[13]. Diagnosis of this disease is often based solely on the clinical symptoms. The objectives of this study were to determine the prevalence, bacterial and fungal etiologic agents associated with Otitis media in Benin City, Nigeria. Otitis media was found in (76.1%) of cases of patients presenting with clinical manifestations of otitis media from a total of 569.
It has been reported that children less than 5 years are more prone to otitis media due to shorter and more horizontal Eustachian tube, lower immunity of children compared to adults and the fact that bacteria adhere better to epithelial cells of children that adults[3,4,14]. This was observed in this study as children 5 years and younger had a higher prevalence of otitis media (95.9%). In this study there was no significant difference between male and female patients in the prevalence of otitis media (74.4%, 77.1%), respectively. This result is in agreement with others[15]. Some studies have reported male gender to be a significant risk factor for acquisition of otitis media[4,14]. The most common pathogen isolated from the ear canal of patients with otitis media is bacteria[15].
Pseudomonas aeruginosa was the predominant isolate causing otitis media generally. This is in agreement with previous studies in Nigeria[14,16], but differs from studies in developed countries were Streptococcus pneumoniae, Haemophilus influenzae and Moraxella catarrhalis predominate[17,18]. Other bacteria isolates recovered in descending order were Staphylococcus aureus, Klebsiella spp, Proteus spp, Streptococcus pneumoniae, Escherichia coli, Alkaligenes spp and Citrobacter freundi.
Fungal species with the highest frequency was Aspergillus niger while the fungi with the lowest frequency were Candida albicans, Aspergillus flavus, Candida tropicalis and Candida parasilopsis. Aspergillus niger is an opportunistic filamentous fungi, it has been identified as the cause of bilateral otomycosis[19]. Aspergillus niger grows on cerumen, epithelial scales and detritus deep in the external canal. The resulting accumulation of these inflammatory materials along with cerumen and fungal debris result in plug formation, which is extremely significant and usually leads to diminished hearing ability; pruritis, irritation of the surface layer of the external ear itself is a predisposing factor for bacterial colonization. There may be superficial erosion of membranes.
The susceptibility profile of the bacteria isolates recovered revealed high level resistance. Prescriptions of antibiotics without laboratory guidance as well as over the counter sales of antibiotics without prescription is common in the Nigerian setting and have been suggested as possible reasons for increase resistance observed in the country[20,21].
Conclusion
In conclusion, an overall prevalence of 76.1% of otitis media was observed among patients attending the ear, nose and throat clinic in University of Benin Teaching Hospital, Benin City, Nigeria. Pseudomonas aeruginosa and Aspergillus niger was the predominant bacterial and fungal isolate causing otitis media. Susceptibility rates to antibiotics were generally poor.
Acknowledgement
We wish to thank the staff of Medical microbiology and ENT Departments University of Benin teaching hospital, Benin City, Nigeria for their cooperation.
References
- 1.Ifante-Rivard C, Fernandez A. Otitis Media in Children: Frequency, Risk factors and research avenues. Epidemiol Rev. 1993;15:446–65. doi: 10.1093/oxfordjournals.epirev.a036129. [DOI] [PubMed] [Google Scholar]
- 2.Arroll B. Antibiotics for upper respiratory tract infections. “An Overview of Cochrane Reviews” Med. 2005;3:255–261. doi: 10.1016/j.rmed.2004.11.004. [DOI] [PubMed] [Google Scholar]
- 3.Li WC, Chiu NC, HSU CH, Lee KS, Hwang HK, Huang-Fu Pathogens in the middle ear effusion of children with persistent otitis media: Implications of drug resistance and complications. J Microbiol Immunol Infect. 2001;34:190–194. [PubMed] [Google Scholar]
- 4.Weiner R, Collison PJ. Middle Ear pathogens in Otitis prone children. South Dakota J Med. 2003;56:103–107. [PubMed] [Google Scholar]
- 5.Aich ML, Biswas AC, Ahmed M, Joarder MAH, Datta PG, Alauddin M. Prevalence of Otitis media with effusion among school going children in Bangladesh. Bangladesh J Otorhinolaryngol. 2009;15:31–34. [Google Scholar]
- 6.Bluestone CD. Otitis media; to treat or not to treat. Consultant. 1998:1421–1433. [Google Scholar]
- 7.Block SL. Causative Pathogens, antibiotic resistance and Therapeutic Considerations in Otitis media. Paediatr Infect Dis J. 1997;16:449–456. doi: 10.1097/00006454-199704000-00029. [DOI] [PubMed] [Google Scholar]
- 8.Minja BM, Machemba A. Prevalence of Otitis media, hearing impairment and cerumen impaction among school children in rural and urban Dar es Salam, Tanzania. Int J Pediatr Otorhinolaryngol. 1996;37:29–34. doi: 10.1016/0165-5876(96)01363-8. [DOI] [PubMed] [Google Scholar]
- 9.National population commission. Census figures 2006, National population commission, FCT Abuja [Google Scholar]
- 10.Cowan ST, Steel KJ. 2nd edn. Cambridge: Cambridge University press; 1974. Manual for the Identification of Medical Bacteria. [Google Scholar]
- 11.National Committee for Clinical Laboratory Standards. Approved Standard M2 – A5 for antibacterial disc susceptibility test. Villanova. 1993 [Google Scholar]
- 12.Collins CH, Lyne PH. 5th Ed. Ibadan: Butterworth and Co-publisher Ltd; 2000. Microbiological Methods. [Google Scholar]
- 13.Yehia MM, Habib HM, Shehab NM. Ear infections J Laryngol Otol. 1990;104:387–389. doi: 10.1017/s0022215100158529. [DOI] [PubMed] [Google Scholar]
- 14.Egbe CA, Mordi R, Omoregie R, Enabulele O. Prevalence of Otitis media in Okada Community, Edo State, Nigeria. Macedonian J. Med. Sci. 2010;3(3):299–302. [Google Scholar]
- 15.Parry D, Roland D. Middle Ear Chronic Suppurative otitis media. Medical treatment. 2002:12–15. [Google Scholar]
- 16.Nwabuisi C, Ologe FE. Pathogenic agents of chronic suppurative otitis media in Ilorin, Nigeria. East Afr Med J. 2002;79(4):202–205. doi: 10.4314/eamj.v79i4.8879. [DOI] [PubMed] [Google Scholar]
- 17.Brook I, Gober AE. Microbiological Characteristic of Persistent otitis media. Arch Otolaryngol. 1998;124:1350–1352. doi: 10.1001/archotol.124.12.1350. [DOI] [PubMed] [Google Scholar]
- 18.Bluestone CD, Stephenson JS, Martin LM. Ten-year review of Otitis media pathogens. Paediatr infect Dis J. 1992;11:57–11. doi: 10.1097/00006454-199208001-00002. [DOI] [PubMed] [Google Scholar]
- 19.Gugnai HC, Okafor BC, Nzeilb F, Njoku-Obian M. Aetiological agent of Otomycosis in Nigeria. Mycoses. 1989;32(5):224–229. doi: 10.1111/j.1439-0507.1989.tb02236.x. [DOI] [PubMed] [Google Scholar]
- 20.Omoregie R, Eghafona NO. Urinary Tract Infection among Asymptomatic HIV patients in Benin City, Nigeria. Br J Biomed sci. 2009;66:190–193. doi: 10.1080/09674845.2009.11730272. [DOI] [PubMed] [Google Scholar]
- 21.Okeke IN, Lamikara A, Edelman R. Socio-economic and behavioural Factors leading to acquired bacterial resistance to antibiotics in developing countries. Emerg Infect Dis. 1999;5:18–27. doi: 10.3201/eid0501.990103. [DOI] [PMC free article] [PubMed] [Google Scholar]