

Abstract
Background:
It is a well known fact that HIV, HBV and HCV are global infectious pathogens contributing to mortality and morbidity in all ages thereby making them infections of grievous public health importance. As donor's potend a possible risk of transfusing these infections of global importance, it makes it imperative for the screening of blood and blood products for these pathogens.
Aim:
This study aims at determining the seroprevalence of HIV, HBV and HCV among intending blood donors.
Subjects and Methods:
A retrospective data analysis for seroprevalence of antibodies to HIV, HBV and HCV was carried out between the 2nd of January and 15th of June 2010 among intending blood donors aged 18-45 and the association of these infections with age group and blood group were analyzed. Sterile venous anticoagulated blood was collected from each of the donors and analyzed for HIV, HBV and HCV using highly sensitive and specific kits. All the positive samples for HIV- 1/2 were sent for reconfirmation using polymerase chain reaction.
Results:
Of the 427 samples analyzed, 203 were positive for HIV, 200 for HBV and 24 for HCV, representing a prevalence of 47.54%, 46.83% and 5.71% respectively among intending blood donors. Among them, blood group O “positive” was the most common blood group with 59.25% followed by blood group B “positive”, A “positive” and O “negative” respectively (p<0.001). The analysis of relationship showed a tendency of high association of these infections in subjects with O “positive” blood group.
Conclusion:
This study emphasizes the need for proper screening of blood donors for HIV, HBV and HCV.
Keywords: HIV, HBsAg, HCV, mortality, morbidity, blood group, infectious pathogens
Introduction
Despite having abundant natural resources and favorable geographical diversities, Nigeria still falls in the category of developing countries in the world. In general, the developmental status of a nation also reflects the health status of her people and the health status of most blood donors in Benin city, Nigeria is generally unsatisfactory. This is necessitated by widespread poverty, non-adherence to public health enlightenment campaigns and difficulty in accessing health facilities occasioned by bad roads. Because of the current blood banking system which encourages non-remunerated or voluntary donation especially to relatives who are hospitalized, we have had occasions to screen all intending donors. Since screening includes blood grouping, serological screening for human immunodeficiency virus (HIV), hepatitis B (HBV), hepatitis C (HCV) and syphilis, it has made it mandatory for donors to be screened for these diseases of global importance. Since last decade both HIV and HBV infections have drawn global attention owing to their grievous public health impact. HIV infection is caused by a retrovirus known as human immunodeficiency virus (type1 and 2) which breaks down the body's immune system and leads to acquired immune deficiency syndrome (AIDS) leaving the person susceptible to opportunistic infections and some malignancies[1]. AIDS in human was first reported in 1981 in USA and HIV was first isolated in 1983[2]. Since then, it has killed more than 25 million people in the world.
The first two cases of HIV and AIDS in Nigeria were identified in 1985, and were reported at an international AIDS conference in 1986[3]. At first the Nigerian government was slow to respond to the increasing rates of HIV transmission and it was only in 1991 that the Federal Ministry of Health made their first attempt to assess Nigeria's AIDS situation[4]. By the end of 2009 it was estimated that there will be only one HIV testing and counseling facility for approximately every 53,000 Nigerian adults, which shows how desperately the government needs to scale up HIV testing services[5].
Statistics show that by the end of 2009, about 3 million people were living with HIV in Nigeria[6]. However, the National Agency for the Control of AIDS (NACA) has just launched its National Strategic Framework to cover 2010 to 2015[6]. This Framework is to reach 80 percent of sexually active adults and 80 percent of most at-risk populations with HIV counseling and testing by 2015; ensure 80 percent of eligible adults and 100 percent of eligible children are receiving ART by 2015; and to improve access to quality care and support services to at least 50 percent of people living with HIV by 2015[7]. Nigeria, therefore, still has a long way to go in combating its devastating AIDS epidemic.
Similarly, Hepatitis B is another pandemic disease caused by hepatitis B virus having some 10 times great impact than AIDS. It has been estimated that more than 2 billion people worldwide have evidence of past or current HBV infection and at least 350 million people are carrying virus[8]. Out of them, one fourth is dying due to cancer or cirrhosis of liver. The reported prevalence of carrier varies greatly from 0.1% in the developed countries to 20% in some developing countries.
Although the prevalence of hepatitis C is unknown, the World Health Organization (WHO) estimates that 3% of the world's population is infected with about 5 million of these in Western Europe[9]. Information is very scarce on the seroprevalence of HIV, HBV and HCV among intending blood donors in Benin city, Nigeria. It should be noted that testing for HIV, HBV and HCV infections is useful for epidemiological monitoring and for public health planning. As a result of this dearth of information, guidelines and other adequate information on the preventive and control measures are essentially lacking in many settings in Nigeria. The aim of this study, therefore, was to determine the seroprevalence of HIV, HBV and HCV in blood donors for epidemiological purpose and to prevent possible transmission of these viruses in blood to the recipients or the health workers.
Subjects and Methods
Study Area
This study was carried out in the University of Benin Teaching Hospital, Benin City, Nigeria between the 2nd of January and 15th of June, 2010. The hospital is a tertiary health care facility with a referral status and an effective blood banking system catering for all the blood needs of patients admitted in the hospital.
Study Population
Since the study was retrospective, health data for intending 427 blood donors who attended the blood donor's bank of the University of Benin Teaching Hospital, Benin City between the 2nd January and 15th June 2010 were collected. Verbal informed consent was obtained from the authorities of the blood bank and the protocol for this study was approved by the Ethical Committee of the University of Benin Teaching Hospital.
Collection and Processing of Samples
Blood samples were collected aseptically by veni-puncture from the donors and were analyzed for blood group, HIV 1 & 2, HBV, HCV, and syphilis.
Determine® HIV-1/2 Test cards (manufactured by Inverness Medical, Japan), Unigold™ Kit (manufactured by Trinity Biotec, Ireland) and HIV -1/2 Stat- Pak® Assay (manufactured by Chembio Diagnostic Systems, USA) were used in a stepwise order for the detection of HIV-1 and HIV-2 in the blood. These methods which are immunochromatographic and qualitative in nature, detect the presence of antibodies to HIV-1 and HIV-2 in human blood and can be read in-vitro having more than 99.9% sensitivity and 99.75% specificity. All the positive cases were sent for target amplification using a qualitative DNA Polymerase Chain Reaction (PCR) (AMPLICOR ® HIV-1 DNA test version 1.5, Roche). Using PCR, all cases were reconfirmed as HIV positive.
Clinitech® HBsAg and Anti-HCV Test Cards (manufactured by Clinotech® Diagnostics, Canada) were used to detect the HBsAg in the blood of study population, which is also a fairly reliable test having more than 99.9% sensitivity and specificity. It is also an in-vitro diagnostic test done by enzyme linked immunochromatographic method and gives qualitative visual read results.
ABO Blood Grouping and Rhesus (RH) Typing
ABO and Rh blood groups determinations were carried out on a slide using monoclonal blood grouping antisera; anti-A, anti-B, anti-AB, and anti-D (BIOTEC Laboratories Ltd, Great Britain).
Results
Out of the 427 subjects (250 males and 177 female) tested for HIV, HBV and HCV, 203 (47.4%) were HIV positive, 200 (46.83%) were HBsAg positive and 24 (5.71%) were HCV positive (Table 1). The results show that majority of the subjects have blood group O “positive” with 59.25%, followed by B “positive” (17.09%), A “positive” (15.69%) and O “negative” (6.08%) respectively. Age group and blood group wise distribution of HIV, HBsAg and HCV positive cases is shown in Tables 2 and 3.
Table 1.
Gender related prevalence of HIV, HBV and HCV among blood donors

Table 2.
Blood group wise distribution of HIV, HBV and HCV positive cases
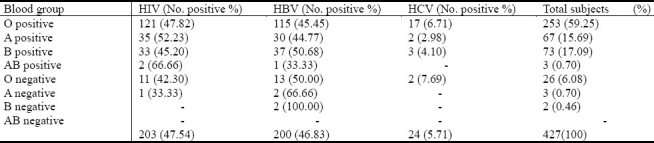
Table 3.
Age group wise distribution of HIV, HBV and HCV positive cases

Discussion
Against the background that Benin city is the cradle of black civilization in Africa, there is much to be desired as the current study reflects a far departure from this truth. This is necessitated by aforementioned factors such as bad roads, poor primary health care facilities and the government's lukewarm attitude towards health. It is a well known fact that HIV, HBV and HCV are global infectious pathogens contributing to mortality and morbidity in all ages[4,9].
A total of 203 (47.54%) out of the 427 subjects screened were seropositive for HIV, while 200 (46.83%) and 42 (5.71%) were positive for HBV and HCV respectively. The results obtained in this study for purpose of clarity will be discussed in turns.
The diseases studied are fairly age specific and behavior dependent. People of age 20-40 years have been found to be more sexually and economically the most active group and these diseases are at high prevalence in those groups[4]. In our study, HIV prevalence has been found highest in age group 30-39 compared to the age group 20-29 which is similar to earlier reports[4]. This variation in prevalence between two groups may be attributed to the variation in duration and opportunity for risk exposure, the continuous sharing of sharps and use of unsterilized materials such as barbing clippers. The fact that these subjects are intending donors does not exclude them from being potential sources or carriers of transfusion transmissible infections (TTI's), especially HIV. So this study uncovered the fact that donors themselves are not an exemption to the general HIV pandemic ravaging sub-Saharan Africa, Nigeria precisely.
Regarding hepatitis B, the prevalence of 45.76% in our study is similar to earlier reports[10] and potentiates the fact that hepatitis B is on the increase. With the exception of Tunisia and Morocco which have intermediate endemicity and Zambia which has intermediate/high endemicity, most countries in Africa including Nigeria have high endemicity for hepatitis B. This clearly explains the reason behind the high seroprevalence obtained in our study.
The prevalence of hepatitis C (5.71%) obtained in this study is close with that reported by Jesse et al[11] with the age group 20-29 more infected. However, the prevalence of HIV, HBV and HCV could be higher in commercial sex workers, their clients and intravenous drug users since they are involved in high risk behaviors and thus incomparable.
A major limitation to our study was the fact that our sample size was small. A study done on 427 subjects alone cannot provide overall prevalence of HIV, HBsAg and HCV status in the country as a whole; nevertheless, it can reflect the disease status in a larger Nigerian community. Also because this study was a retrospective study, we could not gather information about the socio-economic status and behavioral patterns as these are major indices in measuring the prevalence of infections. The seroprevalence data, behavioral patterns and socio-economic status of our community indicates that there is a high potential for the spread of HIV, HBsAg and HCV in Benin city, Nigeria. If adequate preventive measures are not put in place, these infections can lead to the death of the most productive ages of the general population thereby resulting in a vicious cycle of poverty and vulnerability.
Conclusion
The high prevalence of HIV, HBV and HCV observed among the intending blood donors in the study area calls for the need for an extensive blood screening practice in our blood banks.
Acknowledgments
We most sincerely are grateful to the Management of the University of Benin Teaching Hospital for permission to carry out this work.
References
- 1.Joshi SK, Ghimire GR. Serological Prevalence of Antibodies to Human Immunodeficiency Virus (HIV) and Hepatitis B Virus (HBV) among Healthy Nepalese Males–A Retrospective Study. Kathmandu University Medical Journal. 2003;4(1):251–255. [PubMed] [Google Scholar]
- 2.Weller IVD, Comlon CP, Peto TEA. HIV infection and AIDS.Oxford Textbook of Medicine on CD-ROM Version 1.0: 7-10-29 [Google Scholar]
- 3.Adeyi AE. ‘AIDS in Nigeria: A nation on the threshold’. The epidemiology of HIV/AIDS in Nigeria. Harvard Center for Population and Development Studies. 2006:67–69. [Google Scholar]
- 4.Kanki PJ, Adeyi O. ‘AIDS in Nigeria: A nation on the threshold’. Introduction. Harvard Center for Population and Development Studies. 2006:23–45. [Google Scholar]
- 5.WHO, UNAIDS & UNICEF. ‘Towards universal access: scaling up priority HIV/AIDS interventions in the health sector’. 2008 [Google Scholar]
- 6.National Agency for the Control of AIDS (NACA). ‘National HIV/AIDS strategic framework (NSF) 2009 [Google Scholar]
- 7.Sofo CA, Ali-Akpajiak, Toni Pyke. ‘Social development and poverty in Nigeria’, Chapter 3 in ‘Measuring poverty in Nigeria’, Oxfam Working Paper. 2003 [Google Scholar]
- 8.Hepatitis C: Global prevalence. Wkly Epidemiol Rec. 1997;72:341–348. [PubMed] [Google Scholar]
- 9.Mustapha SK, Jibrin YB. The Prevalence of Hepatitis B Surface Antigen in Patients with Human Immunodeficiency Virus Infection in Gombe, Nigeria. Ann Afr Med. 2004;3(1):10–12. [Google Scholar]
- 10.Bukbuk DN, Bassi AP, Mangoro ZM. Sero-prevalence of hepatitis B surface antigen among primary school pupils in rural Hawal valley, Borno State, Nigeria. Journal of Community Medicine and Primary Health Care. 2005;17(1):20–23. [Google Scholar]
- 11.Jesse AO, Babafemi OT, Titilola SA. Prevalence of hepatitis B and C seropositivity in a Nigerian cohort of HIV-infected patients. Ann Hepatol. 2008;7(2):152–156. [PubMed] [Google Scholar]