

Abstract
Aim:
The aim of this study is to compare the occurrence of enamel fractures, sealant fractures and marginal fissures after placement of three sealants: Helioseal F, Conseal F and Clinpro.
Materials and Methods:
Thirty individuals between 13 and 15 years of age, diagnosed with pit and fissure caries by visual and DIAGNOdent examination, were chosen for sealant placement on their mandibular molars. The sealants were placed at random, after which, impressions were made with polyvinyl siloxane and casts were fabricated. Dies were prepared, each of which were sputter coated with gold in order to be examined under a scanning electron microscope. The following morphologies were analyzed from dies from each of the sealant groups: Continuous margins, sealant fractures, marginal fissures and enamel fractures. After six months, they were recalled for impression making. Dies were prepared and microscopically analyzed as mentioned. Based on the time of evaluation, there were two groups: Initial group (soon after placement) and final group (after six months). Statistical analysis was done using the paired ‘t’ test and One-way analysis of variance (ANOVA).
Results and Conclusions:
Clinpro had the greatest fracture resistance, followed by Conseal F and Helioseal F. The occurrence of marginal fissure was found to be least with Clinpro.
Keywords: Conseal, Clinpro, helioseal, sealant
INTRODUCTION
The pits and fissures especially on the occlusal surfaces of the teeth make them vulnerable to dental caries. Although occlusal surfaces constitute only 12.5% of the total surfaces of teeth, they account for 50% of all the carious lesions in school children.[1] Pits and fissures have unfavorable morphology that makes salivary access to these areas difficult, thus minimizing fluoride deposition and remineralization.[2,3] Preventive resin restoration was first suggested by Simonsen, whereby, the susceptible fissures where opened up with a small tapered fissure bur prior to restoring the cavity with diluted composite.[4] The advantages of sealing include: Lower cost in comparison to that of restorations, and a nine fold decrease in the occurrence of caries in comparison to unsealed teeth.[5] The technique was developed by Buonocore, whereby the enamel surface was first etched using orthophosphoric acid. Etching removes contaminants, creates micropores and microprojections. It also increases the surface energy, making the surface easily wettable.[6] Resin then penetrates and polymerizes in the enamel micropores, forming a mechanical bond with the tooth.[7]
The use of flowable restorative systems has increased mainly because of their beneficial properties such as low viscosity, low modulus of elasticity and ease of handling. However, the preventive effects of these sealants would depend on their ability to meticulously seal pits, fissures and anatomical defects, without detaching either partially or completely.[8] In this study, we wanted to compare the ocurrence of enamel fractures, sealant fractures and marginal fissures immediately and six months after the placement of three sealants: Helioseal F (ivoclarvivadent), Conseal F (SDI) and Clinpro (3M ESPE US). The null hypothesis assumed was that there would be no difference among the sealants with regard to the factors considered.
MATERIALS AND METHODS
Individuals aged between 13 and 15 years, who visited the Department of Conservative Dentistry and Endodontics, were inspected for the following criteria:
The permanent mandibular first and second molars were erupted.
These teeth were affected with pit and fissure caries on visual examination (after air-drying), and revealed values between 16 and 20 on the DIAGNOdent (KaVo, USA).
These teeth had no visible hypoplastic defects or fractures.
The first 30 individuals who fulfilled the above criteria were chosen for the study after a written consent was obtained from each of them for the procedures to be carried out. Alginate impressions were made of the lower arch for each patient, from which casts were fabricated with Type 3 dental stone. Modeling wax of one millimeter thickness was used as a spacer with four orientation stops. The special tray was prepared with self-cure acrylic on the cast after the spacer was covered with aluminum foil. After the special tray was prepared, the wax was gently removed along with the aluminum foil. The tray was trimmed and retention holes were made on them. Among the permanent mandibular molars, the first molars and either of the two second molars (whichever had a larger clinical crown length facilitating better rubber dam placement) were chosen for sealant placement in each of the subjects.
The selected teeth were isolated under rubber dam (HYGENIC DENTAL DAM, coltènewhaledent) with high and low volume suction units, cleaned with pumice and rubber cup, and washed thoroughly with water through a three way syringe. A round diamond abrasive point (Fissurotomy micro STF, SS White) on an air-rotor headpiece with water spray was run across the occlusal pits and fissures maintaining a depth of one millimeter. There was no carious material left behind on the concerned teeth after the preparations. The cavities were etched for 15 seconds with 35% orthophosphoric acid (ivoclarvivadent). The three different sealants were placed at random on the selected teeth for each patient in the following way: In the first subject, sealant A was placed on 36, sealant B on 46 and sealant C on 37/47. In the next subject, the order was shifted from the next tooth onwards, that is, sealant A on 46, sealant B on 37/47 and sealant C on 36, and so on. The type of sealant and the concerned teeth were noted for each of the subjects. The sealants were placed strictly according to their manufacturers’ instructions. After sealant placement, they were checked for high points with articulating paper, and if found, were reduced with composite finishing stone (Shofu, Shofu Dental Corporation). Thereafter, the restorations were polished with pumice and rubber cup. A tray adhesive (Virtual, ivoclarvivadent) was applied to the acrylic special tray, after which, monophase polyvinyl siloxane (Virtual, ivoclarvivadent) was loaded on the tray and teeth with a dispensing gun (ivoclarvivadent). Impressions were made according to manufacturers’ instructions and casts were fabricated with high strength Type 4 die stone, 30 minutes after the impressions were taken. Dies were prepared for each tooth, under which, the type of sealant placed was noted by an operator to ensure a blind microscopic analysis. The dyes were then sputter coated with gold (SPI-MODULE) in order to be examined under a scanning electron microscope (SEM JEOL JSM 5800 LV).
The following morphologies were analyzed for teeth in each of the groups under the SEM using the SEM scale (1 μm):
Continuous margins [Figure 1a]
Sealant fracture [Figure 1b]
Marginal fissures [Figure 1c]
Enamel fracture
Figure 1.
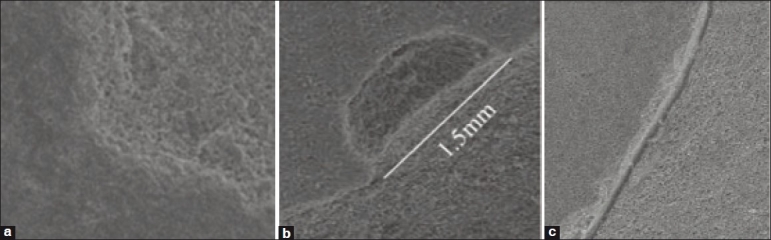
(a) Continuous margin (b) Sealant fracture (c) Marginal fissures
The microscopic measurements were then tallied with the corresponding sealant used. The values were statistically analysed with the paired ‘t’ test (for intra-group comparisons) and One-way ANOVA (for inter-group comparisons). None of the subjects had any post-operative symptoms in the next six months. Thereafter, they were recalled for impression making, die preparation and microscopic evaluation in the above mentioned manner. Hence, the die samples were classified into three groups (n=30 for each group) based on the sealant used: Group A (Helioseal F), Group B (Conseal F) and Group C (Clinpro). Based on the time of evaluation, there were two groups: Initial group (soon after sealant placement) and final group (after six months).
RESULTS
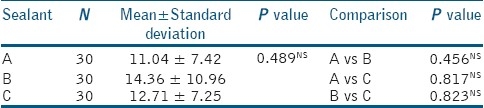
Statistical analysis using the paired ‘t’ test was done for intra-group comparisons [Tables 1–3]. The differences in sealant fracture values [Table 2] between initial and final samples were found to be highly significant for sealant A, significant for sealant B, and insignificant for sealant C. The differences in marginal fissure values [Table 3] were found to be statistically significant for sealant A and sealant B, and insignificant for sealant C. However, the One-way ANOVA, that was used for inter-group comparisons along with Post-hoc Tukeyhonestly significant difference (HSD) for individual group comparisons, revealed no significant results [Tables 4–10]. Therefore, it may be considered that Clinpro has the greatest fracture resistance, followed by Conseal F and Helioseal F. The occurrence of marginal fissures was found to be least with Clinpro. Clinpro showed the best performance, six months post-operatively.
Table 1.
Enamel fracture
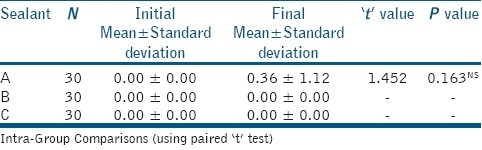
Table 3.
Marginal fissure
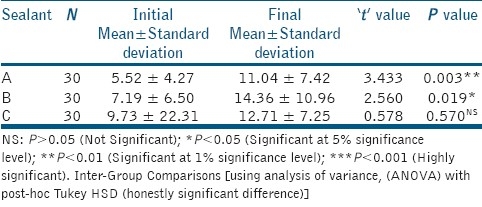
Table 2.
Sealant fracture
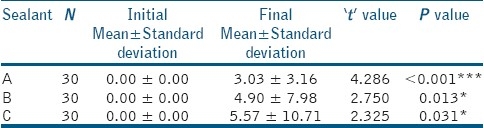
Table 4.
Enamel fracture, initial
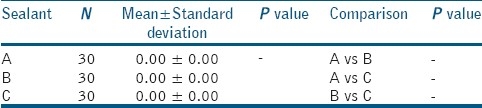
Table 10.
Comparison of change from initial to final

Table 5.
Enamel fracture, final
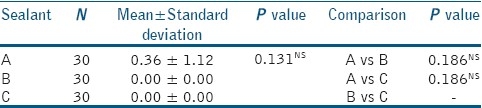
Table 6.
Sealant fracture, initial
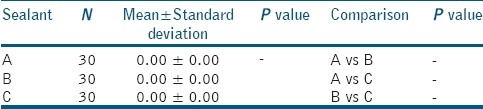
Table 7.
Sealant fracture, final
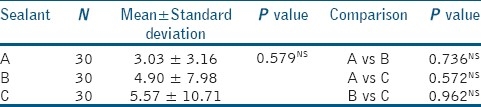
Table 8.
Marginal fissure, initial
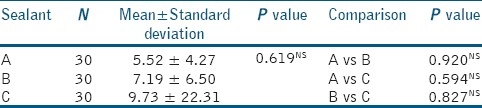
Table 9.
Marginal fissure, final
DISCUSSION
DIAGNOdent has been a popular device used worldwide in the diagnosis of dental caries. According to the operating instructions, DIAGNOdent readings between 11 – 20 signify the presence of outer half enamel caries.[9] Also, in a study by Shinohara et al., it was proved that DIAGNOdent readings between 16 and 21 were indicative of pit and fissure caries.[10] However, in this study a combination of DIAGnodent readings and visual examination was used to ascertain the presence of dental caries. The success of sealants depends on three factors: Penetrability of the acid-etched enamel; marginal sealing; and, wear and abrasion resistance. A tolerable amount of sealant extending into the enamel of cuspal inclines is the key to successful bonding.[11] Fissure enlargement using a bur enhances retention by allowing deeper penetration of the sealant and increasing the surface available for bonding.[2,12] Moreover, it removes the outermost prismless layer of enamel described as ‘coral-like’ by Garcia godoy and gwinett.[13] In this study, the Fissurotomy Micro STF (SS White) bur was used, which are designed for recontouring fissures and accessing decay with minimal enamel removal. These are fast cutting, yet conservative during preparation. These are specifically indicated for enameloplasty, as its head length is 1.5 mm. The tapered shape of the bur allows the cutting tip to encounter very few dentinal tubules at any given time. It also minimizes heat build-up and vibration.
It is for the first time that the three sealants (Helioseal F, Conseal F and Clinpro) have been tested for marginal integrity. All the three sealants are resin based, fluoride releasing and light curable sealants. Helioseal F and Clinpro contained Bis-GMA (Bisphenol A Diglycidyl methacrylate) and TEGDMA (Triethyl glycol dimethacrylate) that function as matrix resin monomers. However, Conseal F is Bis-GMA free. It instead contains UDMA (Urethane Dimethacrylate) which has low shrinkage ability. UDMA is also a constituent of Helioseal F. The filler loading (percentage by weight) in Clinpro and Conseal F are six percent and seven percent, respectively. Lesser filler loading contributes to low viscosity values in these sealants. It also enables better penetrability into pits and fissures. However, Helioseal F has a filler loading of 43% by weight, making it more viscous in comparison to Clinpro and Conseal F. High viscosity contributes to stability and homogeneity of the sealant.
In this study, the differences between initial and final values were found to be highly significant for Helioseal F, significant for Conseal F and insignificant for Clinpro, with regard to sealant fracture. Moreover, the differences between initial and final values were found to be significant for Helioseal F and Conseal F and insignificant for Clinpro, with regard to marginal fissure formation. However, all other comparisons revealed insignificant results.
Marginal fissures occur due to polymerization shrinkage, which in turn is related to cavity geometry, quality of adhesion, curing process and the visco-elastic properties of the materials.[14] However, the higher viscosity of Helioseal F did not seem to make the sealant more resistant to fracture or marginal fissure formation in comparison to the low viscosity sealants, Clinpro and Conseal F. Composites with high modulus of elasticity undergo high polymerization shrinkage, resulting in breakdown of the enamel-sealant micro-mechanical union.[15] Moreover, depending on the size of the orifice and the support offered by the cuspal inclines, a potential weakness may occur in the sealant, and its loss might re-expose the fissure.[16] The thermal expansion coefficient of sealants is significantly different from that of enamel, and the mechanics of expansion and contraction of teeth are different from those of sealants. These factors also contribute to microleakage and marginal fissure formation.[17] Sealants are affected by salivary flow and composition that vary throughout the day.[18,19] Acidic pH affects the properties of restorative materials[20–22] and causes deterioration of the matrix-filler interface.[23] These factors would certainly contribute to the fracture resistance of sealants. Sealant fracture and marginal fissure formation eventually contribute to microleakage, that ultimately leads to failure of the restoration. Hence it is necessary to use sealants of superior quality to minimize the occurrence of failures. Recently, the role of TiF4 as a pit and fissure sealant has been suggested based on its advantages such as high resistance; long retention period; less technical sensitivity; and reduced operating time.[24]
In vitro methodologies such as the one used in this study have the advantage of quantifying the loss of sealant material, rather than an in vivo approach which would calibrate loss of material as present, partially present or absent. However, minor errors could have occurred while impressions were being taken, as little aberrations on the sealant might not have been registered by the impression material. Since linear measurements were taken through the SEM, minor curvatures in fracture lines could not be included while measurements were being taken. We suggest future studies comparing sealants after a longer post-application period with advanced evaluation techniques.
CONCLUSION
It may be concluded from the confines of this study that Clinpro has the greatest fracture resistance, followed by Conseal F and Helioseal F. The occurrence of marginal fissures was found to be least with Clinpro.
Footnotes
Source of Support: Nil,
Conflict of Interest: None declared.
REFERENCES
- 1.Ripa LW. Occlusal sealing: Rationale of the technique and historical review. J Am SocPrev Dent. 1973;3:32–9. [PubMed] [Google Scholar]
- 2.Salama FS, Al-Hammad NS. Marginal seal of sealant and compomer materials with or without enameloplasty. Int J Pediatr Dent. 2002;12:39–46. [PubMed] [Google Scholar]
- 3.El-Housseiny AA, Sharaf AA. Evaluation of fissure sealant applied to topical fluoride treated teeth. J ClinPediatr Dent. 2005;29:215–9. doi: 10.17796/jcpd.29.3.f335gm6732253241. [DOI] [PubMed] [Google Scholar]
- 4.Simonsen RJ. Preventive resin restorations (1) Quintessence Int Dent Dig. 1978;1:69–76. [PubMed] [Google Scholar]
- 5.Simonsen RJ. Retention and effectiveness of a single application of white sealant after 10 years. J Am Dent Assoc. 1987;115:31–6. doi: 10.14219/jada.archive.1987.0199. [DOI] [PubMed] [Google Scholar]
- 6.Lee HL. Adhesion between living tissues and plastics I.Adhesion of epoxy and polyurethane resins to dentin and enamel. J Biomed Mat Res. 1969;3:349–67. doi: 10.1002/jbm.820030213. [DOI] [PubMed] [Google Scholar]
- 7.Buonocore MG. A simple method of increasing the adhesion of acrylic filling materials to enamel surfaces. J Dent Res. 1955;34:849–53. doi: 10.1177/00220345550340060801. [DOI] [PubMed] [Google Scholar]
- 8.Autio-Gold JT. Clinical evaluation of a medium filled with flowable resin material as a pit and fissure sealant. Oper Dent. 2002;27:325–9. [PubMed] [Google Scholar]
- 9.KaVoDIAGNOdent Brief Operating Instructions (What do the numbers mean?) Available from: http://www.kavousa.com/img_cpm/global/files/009/diagnodent/DIAGNOdent_Setup.pdf .
- 10.Shinohara T, Takase Y, Amagai T, Haruyama C, Igarashi A, Kukidome N, et al. Criteria for a diagnosis of caries through the DIAGNOdent. Photomed Laser Surg. 2006;24:50–8. doi: 10.1089/pho.2006.24.50. [DOI] [PubMed] [Google Scholar]
- 11.Taylor CL, Gwinnet AJ. A study of penetration of sealants into pits and fissures. J Am Dent Assoc. 1973;87:1181–8. doi: 10.14219/jada.archive.1973.0601. [DOI] [PubMed] [Google Scholar]
- 12.Blackwood JA, Dilley DC, Roberts MW, Swift EJ., Jr Evaluation of pumice, fissure enameloplasty and air abrasion on sealant microleakage. Pediatr Dent. 2002;24:199–203. [PubMed] [Google Scholar]
- 13.Garcia-Godoy F, Gwinnett AJ. Effect of etching times and mechanical pretreatment on the enamel of primary teeth: A SEM study. Am J Dent. 1991;4:115–8. [PubMed] [Google Scholar]
- 14.Versluis A, Tantbirojin D, Douglas WH. Do dental composites always shrink toward the light? J Dent Res. 1998;77:1435–45. doi: 10.1177/00220345980770060801. [DOI] [PubMed] [Google Scholar]
- 15.Duangthip D, Lussi A. Variables contributing to the quality of fissure sealants used by general dental practitioners. Oper Dent. 2003;28:756–64. [PubMed] [Google Scholar]
- 16.Tillis TS, Stach DJ, Hatch RA, Cross-Poline GN. Occlusal discrepancies after sealant therapy. J Prosthet Dent. 1992;68:223–8. doi: 10.1016/0022-3913(92)90318-5. [DOI] [PubMed] [Google Scholar]
- 17.Theodoridou-Pahini S, Tolidis K, Papadogiannis Y. Degree of microleakage of some pit and fissure sealants: An in vitro study. Int J Pediatr Dent. 1996;6:173–6. doi: 10.1111/j.1365-263x.1996.tb00237.x. [DOI] [PubMed] [Google Scholar]
- 18.Flink H, Tegelberg A, Lagerlof F. Influence of the time of measurement of unstimulated human whole saliva on the diagnosis of hyposalivation. Arch Oral Biol. 2005;50:553–9. doi: 10.1016/j.archoralbio.2004.10.015. [DOI] [PubMed] [Google Scholar]
- 19.Rudney JD. Does variability in salivary protein concentrations influence oral microbial ecology and oral health? Crit Rev Oral Biol Med. 1995;6:343–67. doi: 10.1177/10454411950060040501. [DOI] [PubMed] [Google Scholar]
- 20.Buchalla W, Attin T, Hellwig E. Brushing abrasion of luting cements under neutral and acidic conditions. Oper Dent. 2000;25:482–7. [PubMed] [Google Scholar]
- 21.Gordan VV, Patel SB, Barrett AA, Shen C. Effect of surface finishing and storage media on bi-axial flexure strength and microhardness of resin-based composite. Oper Dent. 2003;28:560–7. [PubMed] [Google Scholar]
- 22.Turssi CP, Hara AT, Magalhães CS, Serra MC, Rodrigues AL., Jr Influence of storage regime prior to abrasion on surface topography of restorative materials. J Biomed Mater Res B ApplBiomater. 2003;65:227–32. doi: 10.1002/jbm.b.10005. [DOI] [PubMed] [Google Scholar]
- 23.Soderholm KJ, Richards ND. Wear resistance of composites: A solved problem? Gen Dent. 1998;46:256–63. [PubMed] [Google Scholar]
- 24.Wahengbam P, Tikku AP, Lee WB. Role of titanium tetrafluoride (TiF(4)) in conservative dentistry: A systematic review. J Conserv Dent. 2011;14:98–102. doi: 10.4103/0972-0707.82598. [DOI] [PMC free article] [PubMed] [Google Scholar]