

Abstract
This paper aims to describe the wide range of compatibility issues between work in the medical profession and the family. Several topics are intertwined and overlap in some areas.
Family friendliness in curative medicine, healthcare, medical studies and the training, specialisation and CPD of doctors is a key theme in the current debate on the future of health and family policies. The rising proportion of women and changes in the medical community characterise the future of medicine. Topics such as working hours and organisation of work, as well as family support and maternity leave, must be discussed further and in particular regarding employees in the health services. This overview will describe where Germany has issues, what is already being done well in the hospitals but could still be improved.
Keywords: Career planning, family research, career-family balance, medical profession, flexible working models
Abstract
Der hier vorliegende Beitrag versucht das umfassende Spektrum der Vereinbarkeitsfragen von Arztberuf und Familie zu beschreiben. Viele Themen greifen ineinander und überlappen sich an einigen Stellen.
Familienfreundlichkeit in der kurativen Medizin, im Gesundheitswesen, im Medizinstudium und in der Ärzte Aus-, Fort- und Weiterbildung ist ein zukunftsweisendes Schlüsselthema der aktuellen Gesundheits- und Familienpolitik. Der steigende Frauenanteil und der Wandel in der Ärzteschaft charakterisieren die Medizin der Zukunft. Dabei müssen die Themen Arbeitszeit und Arbeitsorganisation ebenso wie Familienförderung und Mutterschutz stärker insbesondere für Beschäftigte im Gesundheitswesen diskutiert werden. In dieser Überblicksarbeit wird beschrieben, an welchen Stellen in Deutschland die Probleme liegen, was im Krankenhauswesen bereits gut gemacht wird, aber auch verbessert werden könnte.
Note
This article is based on a lecture by the primary author given at a meeting on 10.02.2011 on the topic of “Hospital Ltd of the Future.”
Current job debate and problem background
The debate on balancing a medical career and family has arrived, both in politics and the medical profession. Medical provision is no longer just a question of providing sufficient human resources in terms of quantity but more specific a question about quality of life and possibilities for arranging one’s private and professional life. In this context, there are also debates about the shortage of doctors, physician drain or distribution problems which are currently conducted on the basis of heterogeneous data [1], [2], [3], [4].
In the 2009 coalition agreement, the federal government made a clear commitment to make the issue of reconciling work and family in the health professions a central task of family and health policy. “People working in health and care services provide an important contribution to the community. They deserve our respect and recognition. The attractiveness of these professions must be improved in terms of the reconciliation of work and family” [5]. The Federal Ministry of Health in 2010 set up a round table on the compatibility of work and family in health care professions with the aim of, amongst other things, tackling barriers in education and training [6]. The Scientific Advisory Council for Family Affairs has dedicated an entire chapter to the medical profession in the new edition of their report on training, studying and parenting and notes that the organisation of studies and training has to change not only but especially because of increasing numbers of women in medicine [7]. The Conference of Medical Faculties in Germany has taken up the issue and in 2010 unanimously adopted a resolution for better reconciliation of family and career [8]. The President of the Conference of Medical Faculties stressed that “the reconciliation of family and work has the highest priority for the next generation” [9] .
Problem areas in medical careers are found especially where people are engaged in time-consuming hands-on work and therefore there is a need for increased attention, treatment and care (care time). In this regard, it must be considered how working hours and work processes can be made more flexible. The surgical subjects, mostly male-dominated, with long hours in the operating room, are particularly affected which means that in the future, concept for recruiting the next generation must be considered [10]. While 45% of first year students of both genders still consider surgery attractive, interest drops to 5% for students after their internship year. The traditional model of smaller hospitals has a male chief physician working virtually around the clock. In order to retain him at the hospital and to stabilise staffing as much as possible, allowances or other benefits are offered. In the future the model where smaller hospitals use personnel services and head hunters to poach these flexible and versatile male specialists from each other through ever more concessions cannot function. Instead, radical reorganisation is needed.
An increasing proportion of women in medical school and increasing proportion of women in medicine
There is much talk about the so-called ‘glass ceiling’ in personnel policy in general as well as in the university context [11]. This means that well-educated women do not reach the upper echelons of business, management boards and top academic positions, being blocked by an invisible “glass ceiling” preventing promotion to the top. Figures from Baden-Württemberg in Human Medicine/Health Sciences show the proportion of women in medical studies is increasing [http://www.destatis.de/jetspeed/portal/cms/]. Currently this figure stands at 61%, whereas in 2000 this percentage was 52%. The figures of women achieving doctoral degrees has risen from 42% (2000) to 55%. Amongst scientific staff, almost half (46%) are currently taken by women. However, in terms of women achieving professorship, the proportion just reaches 25%. In leadership positions, we find the share of women down to 11% but with a rapidly increasing tendency.
For example, at the Department of Child and Adolescent Psychiatry/Psychotherapy at the University Hospital of Ulm, the percentage of women is 78% amongst all employees currently, 5% of the staff are on maternity leave and in the project area, 88% of employees are women [12]. The percentage of women in psychology/social subject groups is often disproportionately high. One important concern is to ensure planning security for female employees who are pregnant or intend to have children. On the one hand, this requires increased staffing levels for the hospital management but it would also be possible, for example, to offer research positions with alternative work patterns to such female colleagues which are amenable to distance working and flexible working hours. In addition, solutions are sought which gradually (re-)integrate young mothers in research projects and participate in training programs or events even while still on maternity leave. However, it remains a problem that the project continuity will be at risk of “baby breaks”. While the DFG, through generous grants for additional maternity cover posts, has contributed a partial solution, most other projects run by research sponsors, such as the BMBF, other federal and state ministries or the EU have no comparable career support measures or work-family compatibility measures. Solutions for the issue of compatibility are, in our view, not just a private concern for employees but are key management tasks for modern future-oriented personnel policy in healthcare [13].
The Right Timing for the Family Phase
Figure 1 (Fig. 1) summarises the aspects of a family and career sensitive hospital, showing the current situation in medical education and at the same time making it clear that family and career in the medical education must be given equal importance.
Figure 1. Family-friendly and career sensitive aspects in medical education.

Family sociology has investigates family formation models especially in the case of male and female academics [14], [15]. Usually the timing of starting a family follows the life cycle model, with a succession of stages of development: education - starting a career - work experience - family (see Figure 2 (Fig. 2)). The phenomenon of women’s dual role in family and career was already described as early as the 60’s [16].
Figure 2. Life-planning models (own design after Kurscheid [17] and Myrdal [16]).
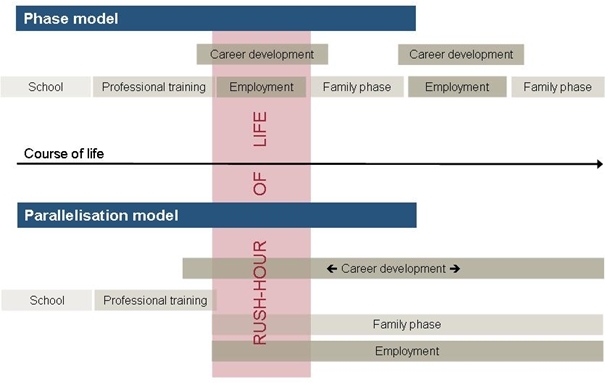
The proportion of those who break the phase model and achieve the parallelisation model, i.e. simultaneously juggling education or work and family, is still accordingly low in comparison [17]. The result is that there are more and more women in Germany who have their first child very late amongst female academia and a high proportion of the female academia who decide not to have a child at all [18], [19], [20], [21]. Therefore a change in thinking is also necessary regarding high positions that untangling rush-hour of life in the middle of medical training and further education requires support mechanisms on behalf of employer. This also means that Germany must consider to what extent it makes sense to have children while at university. In studies on family-friendliness in medical schools, students with children were questioned as experts on the realities of being in education with children. Based on these results, their problems are now better understood. More details are summed up in the following contributions to this special issue [22], [23]. 89% of medical students want children [24], with more men (79%) than women (66%) having concrete ideas about the timing of family formation [25]. When choosing a specialisation, 26% of the surveyed medical students decided for their subject on the basis of a better reconciliation of the medical specialisation with having a family, e.g. anaesthesia with its ordered shifts rather than a time-consuming surgical subject, while medical undergraduates tend to choose their subject on the basis of better future prospects and career prospects [25]. Family-friendly working conditions are the most important factor in decision making, for 96% of medical undergraduates [24] and 84% of clinicians [26]. 29% of male and female graduates are already married a year and a half after graduation and 11% have children [27].
Medical School with Children
Only 4.2% of medical undergraduates start a family while studying. In addition, these students tend to be older, have a prior qualification in a health professions and are still gainfully employed while studying [22], [28], [29], [30], [31], [32]. Working while studying and family responsibilities have a corresponding prolonging effect on the length of study. When asked about the right time to start a family, a third does not see an ideal time [22]; 42% of respondents favour the clinical period of studies. It is striking that 76.7% of respondents in the pre-clinical and 56.0% in the clinical period of studies realise compatibility problems, such as the high number of compulsory hours of attendance, late afternoon classes, increased exam stress and the rigid timetable. It is mostly mothers (72.0%) who take the hit of prolonged studying, while 78.4% of the surveyed fathers did not have to slow their studies.
The examples listed here are also transferable to a similar problem situation in medical postgraduate education, e.g. inflexible organization or labour, bad and unpredictable time management and strictly regulated training requirements which are less focused on content rather than structural factors. A key task for family-friendly under- and postgraduate education in medicine will be more flexible structures and more scope for the individual to arrange their studies. But family-friendliness must not endanger educational entitlement. The same training standards and performance requirements must exist for all medical under- and postgraduates. However, alternative training concepts should be developed which allow temporal flexibility and independence, e.g. e-learning and lecture recording, substitution opportunities for examinations and events with obligatory attendance, teaching and examinations during core working hours.
The ‘Parent Pass’, developed in Ulm the cross-semester agreement for student parents, can be transferred to the hospital in the form of an agreement with the employer for specialisation training [23], [33]. The ‘Parent Pass’ opens up the opportunity for parents to be perceived as a normality without continuously having to explain their situation. Although this is a type of symbolic policy, at the same time it marks a hospital as being family-friendly.
Maternity Regulations in Medical Under- and Postgraduate Studies
The round table on the reconciliation of work and family in the healthcare run by the Federal Ministry of Health noted that maternity leave regulations should not hamper medical under- and postgraduate education unreasonably. Maternity leave regulations should be revised accordingly [34]. At the European level there are currently attempts to extend maternity leave from 14 to 18 or 20 weeks, which would cost the German economy approximately €1.5 billion [35]. An inter-disciplinary maternity report shows that there is no medical evidence for the demands to extend maternity protection periods [36]. From a medical point of view, there is no gynaecological, paediatric, psychiatric and attachment theory research results which would justify an extension of maternity leave. Instead, there are other instruments in Germany, such as parental leave, which ensure the protection of children and young families. The German Society of Gynaecology and Obstetrics has also confirmed this statement [37]. An American study compared the health of children of female gynaecologists who did not comply with the protection period before birth with the health of children born to wives of gynaecologists [38]. They found that the children of those gynaecologists who had been working up until just before birth showed a higher rate of foetal growth retardation, preterm delivery and pre-eclampsia. It should therefore also be noted that demands for the reduction of protective measures which are based solely on the career or educational interests of the mother without regard to balanced risk assessment can create new risks for the mother and child. A more objective debate and a review of empirical findings seem imperative.
Replacement Models and Transfer of Human Capital
The German Research Foundation (DFG) by now will fund a second research position for male and female scientists who have to take leave due to pregnancy or family responsibilities (maternity leave, nursing months) [http://www.dfg.de]. But this creates a situation where there might be competition between employees who are on leave and the replacement. Concerns might arise about whether a stand-in might work better and could threaten continued employment. The Department of Child and Adolescent Psychiatry at the University Hospital of Ulm has taken up another model. The first Senior Replacement Professor of a female professor, who is an emeritus professor at another university, fills the maternity leave slot of a W3 professorship. Without career plans or intentions to stand out, the senior professor can start immediately and pass on her experience in scientific work to younger male and female colleagues. The costs are very low, as the pro bono chair is designed to operate without remuneration.
In medicine, active senior citizens could be involved more as supervisors of doctors in training, as practiced at the department for child and adolescent psychiatry in Ulm in a different context using an experienced specialist. Previously, transgenerational transfer was based more on the transfer of care and assets. The transfer of human capital should be given greater consideration in the media as well.
The Family-friendly Hospital
Both the Federal Ministry for Family Affairs (BMFSFJ) and the Federal Chamber of Physicians have published brochures on family-friendly workplaces in hospitals, describing best-practice examples and giving checklists for a family-friendly hospital [39], [40]. Offering equal career opportunities for men and women, particularly for male and female doctors and attractive basic conditions contribute majorly to an institutions family credentials. Working conditions in hospitals, however, are still mostly characterised by round-the-clock shifts and short-term changes in the work roster. However, for families reliable, long-term time management is a key factor. If many fathers and mothers work in a unit (ward, operating room), this also increases the risk of absences through, for example, childhood diseases and such events. Medical teams therefore need employees who are able and willing to fill in at extremely short notice [40]. Usually doctors have little influence on their working times because all services must be staffed, which leads to unattractive working hours. Time management will be a key challenge for the leadership. For example, one must be able to depend on handoffs and ward visits to occur at fixed times and not subject to unpredictable changes by the chief surgeon/chief physician.
Incentives for Family Support
The Medical School of Hanover (MHH), in addition to the research incentives as part of the performance-oriented allocation of funds (LOM) which are available at virtually all German university hospitals, has introduced a “family-LOM” [http://www.mh-hannover.de/familie.html]. A division of MHH receives a financial award, if a working female doctor returns to work within one year after the birth of her child. This supports young female doctors and scientists and the development of support structures at the hospital. Other hospitals, such as the Centre for Psychiatry of South Württemberg, have allocation models, i.e. pool models. Maternity replacements are not financed from the departmental budget but from a common pool budget. This does not replace the missing female doctor but the department heads are not in financial difficulties if an employee drops out.
Differences in Support
The contribution by Liebhardt et al. in this issue on practical approaches for family-friendly medical degrees shows [23] that family-friendly measures, such as childcare facilities, family services and counselling and family audits are offered more frequently in large hospitals. Smaller hospitals show clear deficits. Many leading medical universities and university hospitals are audited by berufundfamilie (career and family) audit of the Hertie Foundation. However, amongst smaller hospitals offering between 300-600 beds, only 25% offer family-friendly measures [39]. Germany needs models which help small hospitals outside the cities to practice family-friendliness successfully. The University of Ulm, together with their academic teaching hospitals, has set up a regional network, with the member hospitals meeting once a year to learn from each other. Baden-Württemberg will invest €7m in structural improvements in medical care outside the cities in the coming years. Baden-Württemberg’s Minister of Health, Dr. Monika Stolz, demanded the following during the presentation of this 10-point action plan in Mutlangen: “The medical profession is becoming more female. We urgently need structures on the ground that enable people to harmonise work and family life in order to make the profession of GP more attractive.” A key point of the funding program therefore is to give institutions an incentive to contribute with innovative, family-friendly approaches to outpatient medical care outside the cities [41].
There are also differences between universities and university hospitals. Universities, in particular, have professionalized their careers’ services, while university hospitals offer little guidance, for example regarding specialisation or scientific careers and work-family issues. Continued improvement must be done for young male and female doctors both in terms of advice, services and career planning and for reconciling work and family issues. Integrated career-family counselling is especially important against the backdrop of changing life concepts and aspirations because future generations will place increasing value on a healthy balance between work and family [24], [25].
Part-time Work in the Medical Profession a Women’s Thing to Date
The ratio of part-time employment in the medical profession stands at about 90% [20], with two-thirds of them female. As an increasing proportion of women in the medical profession is expected in the future, the traditional model of the “full-time specialist with continuous work overload up to retirement” will no longer be the image of the doctor of the future. The medical profession is changing, therefore clinical structures and working conditions must also change. Considerably more staff could be trained simultaneously who could then work in job sharing schemes for doctors. But this personnel will have to be on the same level of education which will cause additional costs. The basis for calculations and assumptions used to date to calculate the added value of a trained doctor must be revisited because there will be more family-related absences. Career breaks and part-time work are still gender-specific phenomena amongst women who often suffer long-term disadvantages caused by maternity leave.
Flexible Working Models
Reduced working time models, near full-time employment and flexible reduction of working hours are the models of the future. But this requires technical support, for example for more distance working and digital, networked working which enable location-independent employment, especially for the growing documentation workload in medicine, which need not be done at the bedside. Often, however, data protection issues prevent alternative solutions because firewalls deny access to an institution’s internal data from outside the hospital. Digital solutions in future must be developed with more reference to family-friendly working needs because only the expansion of digital solutions will enable higher flexibility in terms of time and location.
The culture of ward visits must change so that daily activities are restructured according to working time reduced models, without making part-time employees feel guilty. A new culture is needed for handovers and work rosters. For example, handover could be organised better using handheld devices with simultaneous documentation.
Medical Specialisation Regulations
In almost all educational systems, part-time specialisation is possible [23] which is a big step in the right direction. However, specialisation currently takes one to four or five years, which in a part-time model is extended to up to ten years. The problem is this leads to male or female specialists becoming available to the healthcare system very late. Medical associations should ponder to what extent the requirements should become more substance-based rather than defining them based on employment relationships. Here too, digital solutions could enrich specialisation and the development of viable alternatives to on-site training in order to reduce the length of training periods.
Summary and Outlook
Currently, large hospitals are better able to implement compatibility solutions. The biggest problem exists for medicine outside the cities and in the surgical specialties. Chambers and associations must do more to support compatibility solutions and to make the educational requirements in the regulations for postgraduate training more flexible by primarily implementing a review and re-orientation towards content. In-house childcare is important but does not solve all problems. Men are changing towards becoming more family oriented. The model of the “expensive specialist” is becoming a thing of the past. It will require flexible working models with collegial work-cover. While the understanding of issues surrounding the reconciliation of career and family and childcare is growing, the understanding of the ever-increasing challenges medical workers face in the care of their dependents is still very low despite the expertise of many hospitals for health problems and care for the elderly. With its draft law on nursing time, the BMFSFJ has put forward a rather cautious approach based on voluntary action. The healthcare system in particular has concepts to offer on which home-friendly services, care services and support of family care could be modelled. Such models created by experts, who are personally affected, could have a positive affect on the quality of care standards in general. Therefore, models which successfully combine a medical career and family should increasingly be tested in structurally weak areas. Ultimately, we do not have enough reliable data regarding the wishes and needs of young doctors of both genders and their desired solutions. Career-family balance models should be designed on the basis of empirical data and offered with advice structures alongside. E-learning and location-independent digital documentation systems should be used more. Family-friendliness can be promoted by ensuring that career breaks due to family duties are not to the detriment of employees and departments but by developing creative solutions for replacement models which are supported by allocation and incentive models for families and hospitals.
Competing interests
The authors declare that they have no competing interests.
References
- 1.Blum K, Löffert S. Ärztemangel im Krankenhaus. Ausmaß, Ursachen, Gegenmaßnahmen. Forschungsgutachten im Auftrag der Deutschen Krankenhausgesellschaft. Düsseldorf: Deutsches Krankenhausinstitut e.V.; 2010. p. Ärztemangel im Krankenhaus. [Google Scholar]
- 2.Jacob R, Heinz A. Berufsmonitoring Medizinstudenten. Bundesweite Befragung von Medizinstudenten. Trier: Universität Trier, Arbeitsgruppe angewandte Sozialforschung im Auftrag der Kassenärztlichen Bundesvereinigung; 2010. [Google Scholar]
- 3.Ostwald DA, Ehrhard T, Bruntsch F, Schmidt H, Friedl C. Fachkräftemangel. tationärer und ambulanter Bereich bis zum Jahr 2030. Darmstadt: Wifor und PricewaterhouseCoopers AG; 2010. Available from: http://www.vpkbb.org/uploads/media/Studie_Fachkraeftemangel_Gesundheit.pdf. [Google Scholar]
- 4.Kopetsch T. Dem deutschen Gesundheitswesen gehen die Ärzte aus! Studie zur Altersstruktur-und Arztzahlentwicklung. 5. aktualisierte und komplett überarbeitete Auflage. Berlin: Bundesärztekammer und Kassenärztliche Bundesvereinigung; 2010. [Google Scholar]
- 5.Bundesregierung. Wachstum. Bildung. Zusammenhalt. Der Koalitionsvertrag zwischen CDU, CSU und FDP. Berlin: Bundesregierung; 2009. p. 85. Available from: http://www.cdu.de/doc/pdfc/091026-koalitionsvertrag-cducsu-fdp.pdf. [Google Scholar]
- 6.Bundesministerium für Gesundheit. Empfehlungen des Runden Tisches Vereinbarkeit Familie und Beruf im Gesundheitswesen vom 1. Dezember 2010. Berlin: Bundesministerium für Gesundheit; 2010. [Google Scholar]
- 7.Bundesministerium für Familie, Senioren, Frauen und Jugend. Ausbildung, Studium und Elternschaft. Studium und Elternschaft. Analysen und Empfehlungen zu einem Problemfeld in Schnittpunkt von Familien- und Bildungspolitik. Gutachten des wissenschaftlichen Beirats für Familienfragen beim Bundesministerium für Familie, Senioren, Frauen und Jugend. 2. Auflage. Berlin: Bundesministerium für Familie, Senioren, Frauen und Jugend; 2011. [Google Scholar]
- 8.Medizinischer Fakultätentag Deutschland. Resolution zur Familienfreundlichkeit in Studium und Weiterbildung von Medizinerinnen und Medizinern. Verabschiedet am 4.6.2010 in Hannover. Berlin: Medizinischer Fakultätentag Deutschland; 2010. Available from: http://www.mft-online.de/dokument/2010_06_07_MFT_Familienfreundlichkeit_Resolution.pdf. [Google Scholar]
- 9.Bitter-Surmann D. Ärzteschwund/Ärztemangel. Wo liegen die Probleme? Forschung Lehre. 2011;1:42–44. [Google Scholar]
- 10.Joos U. Dringend gesucht: Chirurgen. Wie eine neu gegründete Deutsche Chirurgie Stiftung helfen will. Forschung Lehre. 2011;1:46–47. [Google Scholar]
- 11.Bundesministerium für Familie, Senioren, Frauen und Jugend. Frauen in Führungspositionen. Barrieren und Brücken. 3. Auflage. Berlin: Bundesministerium für Familie, Senioren, Frauen und Jugend; 2010. [Google Scholar]
- 12.Bleich S, Fegert JM. Personalstatistik der Klinik für Kinder- und Jugendpsychiatrie/Psychotherapie des Universitätsklinikum Ulm. Eigene Auswertung. Ulm: Universität Ulm; 2011. [Google Scholar]
- 13.Gemeinsame Wissenschaftskonferenz (GWK) Frauen in der Medizin - Ausbildung und berufliche Situation von Medizinerinnen. Mat Bildungsplan Forschungsförd. 2010;(117) [Google Scholar]
- 14.Hill PB, Kopp J. Familiensoziologie. Grundlagen und theoretische Perspektiven. 4.. überarbeitete Auflage. Wiesbaden: Vs Verlag; 006. [Google Scholar]
- 15.Huinik J, Konietzka D. Familiensoziologie. Eine Einführung. Frankfurt am Main: Campus Verlag; 2007. [Google Scholar]
- 16.Myrdal A, Klein V, Schroth-Pritzel U. Die Doppelrolle der Frau in Familie und Beruf. 2. Auflage. Köln: Kiepenheuer & Witsch; 1971. pp. 66–82. [Google Scholar]
- 17.Kurscheid C. Das Problem der Vereinbarkeit von Studium und Familie. Eine empirische Studie zur Lebenslage Kölner Studierender. Münster: LIT; 2005. [Google Scholar]
- 18.Schmitt C, Wagner G. Kinderlosigkeit von Akademikerinnen überbewertet. Wochenbericht. Dtsch Institut Wirtschaftsforsch (DIW) 2006;21:313–317. [Google Scholar]
- 19.Cornelißen W, Fox K. Studieren mit Kind. Die Vereinbarkeit von Studium und Elternschaft: Lebenssituationen, Maßnahmen und Handlungsperspektiven. Wiesbaden: VS Verlag für Sozialwissenschaften; 2007. p. 194. [Google Scholar]
- 20.Statistisches Bundesamt. Mikrozensus 2008. Neue Daten zur Kinderlosigkeit in Deutschland. Wiesbaden: Statistisches Bundesamt; 2009. pp. 1–38. [Google Scholar]
- 21.Metz-Göckel S. Wissenschaft als Lebensform - Eltern unerwünscht? Kinderlosigkeit und Beschäftigungsverhältnisse des wissenschaftlichen Personals aller nordrhein-westfälischer Universitäten. Opladen [u.a.]: Budrich; 2009. [Google Scholar]
- 22.Niehues J, Prospero K, Fegert JM, Liebhardt H. Familienfreundlichkeit im Medizinstudium in Baden-Württemberg. Ergebnisse einer landesweiten Studie. GMS Z Med Ausbild. 2012;29(2):Doc33. doi: 10.3205/zma000803. Available from: http://dx.doi.org/10.3205/zma000803. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Liebhardt H, Niehues J, Fegert JM. Praktische Ansätze für ein familienfreundliches Medizinstudium. GMS Z Med Ausbild. 2012;29(2):Doc32. doi: 10.3205/zma000802. Available from: http://dx.doi.org/10.3205/zma000802. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Jacob R, Heinz A. Berufsmonitoring Medizinstudenten. Bundesweite Befragung von Medizinstudenten. Trier: Universität Trier, Arbeitsgruppe angewandte Sozialforschung im Auftrag der Kassenärztlichen Bundesvereinigung; 2010. [Google Scholar]
- 25.Dettmer S, Kuhlmey A. Karriere- und Lebensplanung angehender Ärztinnen und ÄrzteErgebnisse der Erstbefragung angehender Absolventen der Humanmedizin an der Charité – Universitätsmedizin Berlin (KuLM-Studie) Berlin: Charité; 2009. [Google Scholar]
- 26.Flintrop J. Arbeitsbedingungen der Klinikärzte. Die Tarifverträge zeigen Wirkung. Dtsch Arztebl. 2011;7(108):A310–3011. [Google Scholar]
- 27.INCHER. Absolventenbefragung „Studienbedingungen und Berufserfolg“. Kassel: ICHER; 2008. [Google Scholar]
- 28.Liebhardt H, Fegert JM. Medizinstudium mit Kind: Familienfreundliche Studienorganisation in der medizinischen Ausbildung. Lengerich: Pabst Sciences Publisher; 2010. [Google Scholar]
- 29.Liebhardt H, Fegert JM, Dittrich W, Nürnberger F. Medizin studieren mit Kind. Ein Trend der Zukunft? Dtsch Arztebl. 2010;107(34-35):1613–1614. [Google Scholar]
- 30.Prospero K, Niehues J, Liebhardt H, Fegert JM. Studie: Zeit für Familiengründung während des Medizinstudiums? Ärztin. 2010;57(3):15–16. [Google Scholar]
- 31.Liebhardt H. Wie können Medizinstudium und Arztberuf familienfreundlicher werden? Hartmannbund BW aktuell. 2010;2(11):4. [Google Scholar]
- 32.Liebhardt H, Stolz K, Mörtl K, Prospero K, Niehues J, Fegert JM. Familiengründung bei Medizinerinnen und Medizinern bereits im Studium? Ergebnisse einer Pilotstudie zur Familienfreundlichkeit im Medizinstudium an der Universität Ulm. GMS Z Med Ausbild. 2011;28(1):Doc14. doi: 10.3205/zma000726. Available from: http://dx.doi.org/10.3205/zma000726. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Liebhardt H, Stolz K, Mörtl K, Prospero K, Niehues J, Fegert JM. Evidenzbasierte Beratung und Studienverlaufsmonitoring für studierende Eltern in der Medizin. Hochschulwesen. 2011;59(1):27–33. [Google Scholar]
- 34.Widmann-Mauz Familienfreundlichkeit im Medizinstudium in Baden-Württemberg. Ergebnisse einer Studie. GMS Z Med Ausbild. 2012;29(2):Doc37. doi: 10.3205/zma000807. Available from: http://dx.doi.org/10.3205/zma000807. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Frankfurter Allgemeine Zeitung. Längerer Mutterschutz kostet Milliarden. Frankfurt: FAZ; 2011. [Google Scholar]
- 36.Fegert JM, Liebhardt H, Reister F, Hummler H, Britsch P, Weber J, Ziegenhain U. Evidenzbasis für Mutterschutzfristen? Interdisziplinäres medizinisches Gutachten zur Frage der erforderlichen Dauer von Mutterschutzfristen vor dem Hintergrund der auf europäischer Ebene angestrebten Verlängerung des Mutterschaftsurlaubs. Berlin: Bundesministerium für Familie, Senioren, Frauen und Jugend; 2010. [Google Scholar]
- 37.Kreienberg R. Kurzgutachten der Deutschen Gesellschaft für Gynäkologie und Geburtshilfe (DGGG) zum Thema „Mutterschutz“. Berlin: Deutsche Gsellschaft füßr Gynäkologie und Geburtshilfe; 2010. [Google Scholar]
- 38.Gabbe SG, Morgan MA, Power ML, Schulkin J, Williams SB. Duty hours and pregnancy outcome among residents in obstetrics and gynecology. Obstet Gynecol. 2003;102(5 Pt 1):948–951. doi: 10.1016/S0029-7844(03)00856-1. Available from: http://dx.doi.org/10.1016/S0029-7844(03)00856-1. [DOI] [PubMed] [Google Scholar]
- 39.Bühren A, Schoeller AE. Familienfreundlicher Arbeitsplatz für Ärztinnen und Ärzte. Lebensqualität in der Berufsausübung. Berlin: Bundesärztekammer; 2010. [Google Scholar]
- 40.Bundesministerium für Familie, Senioren, Frauen und Jugend. Vereinbarkeit von Beruf und Familie im Krankenhaus. Berlin: Bundesministerium für Familie, Senioren, Frauen und Jugend; 2009. [Google Scholar]
- 41.Hillienhof A. Aktionsprogramm für Landärzte. Dtsch Arztebl. 2011;108(11):118. [Google Scholar]