

INTRODUCTION
Renal replacement lipomatosis (RRL) is an extremely rare condition, which occurs secondary to atrophy or destruction of renal parenchyma, with proliferation of excessive lipomatous tissue in renal sinus, renal hilum and perirenal space. Clinical presentation, radiological features and pathological findings aid in confirming the diagnosis. Magnetic resonance imaging (MRI) has evolved as a valuable alternative and complementary imaging modality to ultrasound (US) and computed tomography (CT) in renal replacement lipomatosis, especially in patients with renal failure and those allergic to iodinated contrast agents. Till date, there are only a few case reports regarding the MR imaging findings in RRL. Herein, we are reporting a rare case of RRL depicting most of the radiological findings.
CASE REPORT
History and examination
A 52-year-old lady was admitted to our hospital, with a complaint of a mass in her right abdomen since the last 6 months with previous history of right renal calculi. On physical examination, a vague tender mass was palpable from the right upper abdomen.
Plain radiograph of the abdomen revealed calculi of varying sizes in the right renal area with increased lucency in the area of renal density; with obscured renal outline. Ultrasound revealed parenchymal atrophy with few echogenic calculi and hyper echoic tissue surrounding the renal parenchyma on right side. Unenhanced CT scan [Figure 1] revealed severe right renal parenchymal atrophy and multiple calculi. There was extensive fatty infiltration replacing the kidney, nearly filling the right abdominal cavity. MR findings revealed severe renal parenchymal atrophy, replaced by the adipose tissue. T2-weighted [half Fourier acquisition single-shot turbo-spin echo (HASTE)] sequence [Figure 2] revealed simple cysts in left kidney, minimal right perirenal fluid collection with fatty replacement of kidney. On dynamic MR urography [Figure 3], nonfunctioning of right kidney was demonstrated. After nephrectomy, histopathology of the lesion confirmed replacement of renal parenchyma with fat.
Figure 1.
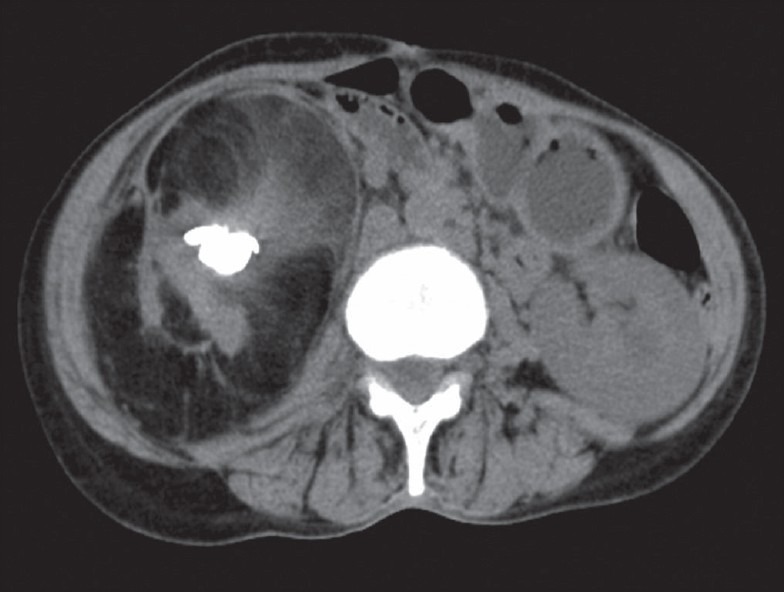
Plain axial CT scan shows severe right renal parenchymal atrophy, strandings surrounding renal outline with calculi and extensive fatty infiltration
Figure 2.
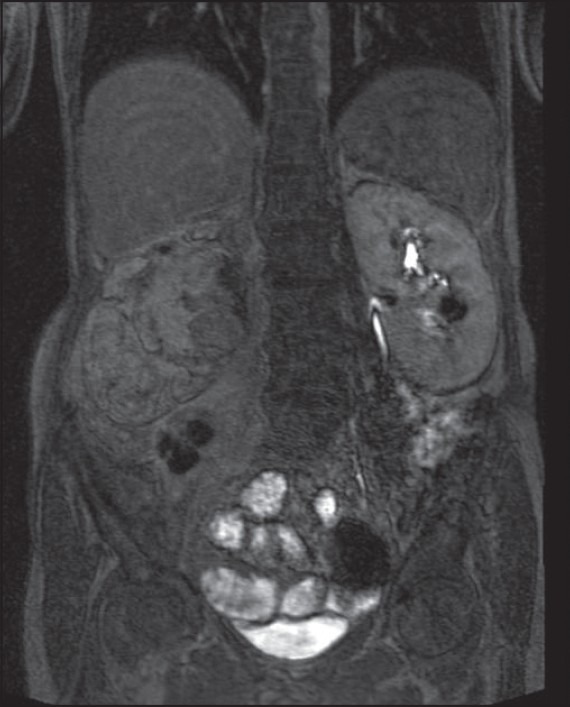
VIBE sequence shows nonfunctioning of right kidney, completely suppressed fat and excretion of contrast in left kidney, ureter
Figure 3.

Axial scan HASTE sequence shows left kidney cysts and posterior right pararenal fl uid collection along with fatty replacement of entire kidney
DISCUSSION
RRL is an uncommon, chronic debilitating disorder, usually occurring unilaterally. There is marked proliferation of fatty tissue within the renal sinus, hilum and perirenal space, usually secondary to destruction or atrophy of renal parenchyma due to longstanding inflammation.[1,2] This condition most commonly follows calculous disease. However, associations with conditions such as aging, renal tuberculosis and post renal transplantation have also been reported.[3,4]
Fatty proliferation in kidney represents a spectrum of disorders ranging from mild lipomatosis in the renal sinus with underlying normal parenchyma (renal sinus lipomatosis) to a severe variety with lipomatosis involving renal sinus, hilum and peri-nephric region with underlying atrophic parenchyma (renal replacement lipomatosis). The presence of atrophic renal parenchyma distinguishes this condition from other causes of fibro-fatty proliferation in and around the kidney, as in obesity, Cushing's disease or excessive corticosteroid therapy and idiopathic.[1]
There is no specific clinical feature to diagnose this condition. Patients usually present with complaints of recurrent flank pain, fever, weight loss and mass per abdomen.
By using conventional radiological methods, it is very difficult to diagnose this condition. Ultrasound, CT and MRI aid in accurate diagnosis. Sonologically, RRL appears as a hyperechoic mass in the renal fossa, suggestive of fatty tissue with variable atrophic parenchyma with or without visualization of calculus.[2] Computed tomography is the most accurate imaging modality. It differentiates with certainty the fatty nature of the lesion from other non-fatty lesions, can define the extent of the fatty proliferation in the renal fossa,[5] and can detect associated complications like peri-nephric abscesses, hydronephrosis and renal/ ureteric calculi.
MRI provides further confirmation of disease. HASTE sequence is a heavily T2-weighted sequence; hence depicting hydronephrosis, renal cysts and perirenal edema explicitly. Moreover, being an ultrashort sequence, it is not affected by respiratory motion artifact. TRUFI [True (FISP) Fast Imaging with steady precession] is a fast sequence which provides great anatomic detail.[3] A recently introduced post-contrast gradient-echo technique with a volumetric interpolation during breath-hold (VIBE) sequence depicts excretory function of kidney without motion-related artifacts.
Using combined modalities, it is possible to differentiate RRL from other fat-containing neoplasms in the renal fossa, such as angiomyolipoma, lipoma and liposarcoma. It is very difficult to differentiate RRL from xanthogranulomatous pyelonephritis, since both these conditions are associated with longstanding inflammation and calculous disease. However, pathologically, Xanthogranulomatous pyelonephritis shows increased lipid-laden inflammatory foam cells infiltrating the renal parenchyma. In contrast, RRL shows increased lipid content outside the renal parenchyma.[6] CT and MRI show the characteristic radiological features in both conditions. But in patients allergic to iodinated contrast and with raised renal parameters, inconclusive CT scan findings; MRI is a valuable alternative modality to diagnose the condition.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Ambos MA, Bosniak MA, Gordon R, Madayag MA. Replacement lipomatosis of the kidney. AJR Am J Roentgenol. 1978;130:1087–91. doi: 10.2214/ajr.130.6.1087. [DOI] [PubMed] [Google Scholar]
- 2.Subramanyam BR, Bosniak MA, Horii SC, Megibow AJ, Balthazar EJ. Replacement lipomatosis of the kidney: Diagnosis by computed tomography and sonography. Radiology. 1983;148:791–2. doi: 10.1148/radiology.148.3.6878703. [DOI] [PubMed] [Google Scholar]
- 3.Casas JD, Cuadras P, Mariscal A, Domènech S. Replacement lipomatosis related to renal tuberculosis: Imaging findings in one case. Eur Radiol. 2002;12:810–3. doi: 10.1007/s003300101056. [DOI] [PubMed] [Google Scholar]
- 4.Chang SD, Coakley FV, Goldstein B. Renal replacement lipomatosis associated with renal transplantation. Br J Radiol. 2005;78:60–1. doi: 10.1259/bjr/31723131. [DOI] [PubMed] [Google Scholar]
- 5.Kantarci M, Onbas O, Bozkurt M, Alper F, Okur A. Renal replacement lipomatosis: MR findings in one case. Magn Reson Imaging. 2004;22:275–9. doi: 10.1016/j.mri.2003.07.009. [DOI] [PubMed] [Google Scholar]
- 6.Kiris A, Kocakoc E, Poyraz AK, Dagli F, Boztosun Y. Xanthogranulomatous pyelonephritis with nephrocutaneous fistula and coexisting renal replacement lipomatosis: The report of a rare case. Clin Imaging. 2005;29:356–8. doi: 10.1016/j.clinimag.2004.12.002. [DOI] [PubMed] [Google Scholar]