

Abstract
Data from 1087 adolescent participants in three waves of the National Longitudinal Study of Adolescent Health was used to examine the effects of peer selection and socialization processes in adolescence on later reports of sexually-transmitted infections (STI) and unintended pregnancies. Friends’ attitudes and behavior were assessed with friends’ reports. Among males, there was evidence for selection effects on STI diagnoses and socialization effects on reports of unintended pregnancy, both involving friends’ attitudes. Among females, there was evidence for long-term effects of both socialization and selection processes involving same-sex friends’ attitudes. Discussion focuses on the importance of peer and individual attitudes as potential intervention targets.
Studying transmission networks in high-risk populations has yielded important information about preventing HIV and other sexually-transmitted infections (STI) among adults (Derlega & Barbee, 1998; Potterat, Rothenberg, & Muth, 1999). Research also links adolescent peer network characteristics to HIV/STI risk behaviors (Brown, Dolcini, & Leventhal, 1997; Ozer, Weinstein, Maslach, & Siegel, 1997; Wood, Nagoshi, & Dennis, 1992; Worth & Rodriguez, 1987). Among these characteristics are selection (choosing friends whose attitudes or behavior are like one’s own) and socialization (changing one’s own attitudes or behavior to become more like those of friends). Both processes increase similarity between adolescents and their peers (McPherson, Smith-Lovin, & Cook, 2001). Developmental risk studies (Brown, DiClemente, & Park, 1992; Henry, Schoeny, Deptula, & Slavick, 2007) and interventions (Walter, Vaughan, Gladis, & Ragin, 1993) both suggest the importance of adolescent peer relationships in sexual risk. This study investigates whether peer effects on sexual risk are limited to adolescence or have detectable longer-term effects on adult outcomes. Further, this study explores the extent to which selection or socialization processes in adolescence are involved in any longer-term peer effects. Finally, this study assesses the contributions of change in attitude and change in behavior to longer-term effects.
Antecedents and consequences of risky sexual behavior
Adolescent rates of STIs continue to cause concern, with teenage females reporting the highest rates of Chlamydia infection (Centers for Disease Control and Prevention, 2009). Studies have identified numerous predictors of risky sexual behavior. For instance, adolescents who lack close relationships with their parents are more likely to engage in risky sexual activity (See Fisher, 2004; Miller, Benson, & Galbraith, 2001 for reviews.). More positive attitudes about the benefits of sex and fewer beliefs about the costs of sex also predict sexual initiation (Deptula, Henry, Schoeny, & Slavick, 2005). Buhi and Goodson’s (2007) review identified several key predictors of early adolescent sexual initiation, namely an intention to initiate sex, perceptions of peer sexual behavior and attitude norms, perceptions of parental attitudes about sex, and unsupervised time at home.
A past history of STI infection is a strong risk factor for future STI infections (Wagstaff, Delamater, & Havens, 1999). This pattern is likely tied to condom use, as adolescents who use condoms during their first sexual experience are more likely to use condoms as young adults, and have lower STI rates as measured by biological tests (Shafili, Stovel, & Holmes, 2007).
Young adult effects of adolescent peer relationships
Based on Moffitt’s (1993), now classic taxonomy of adolescent-limited and life-course persistent antisocial behavior, there exists a general belief that peer influence, like adolescent-limited delinquency, is primarily confined to adolescence. Moffitt (1993) suggested that adolescent-limited delinquency begins with “social mimicry” of the antisocial lifestyles of peers. Life-course persistent delinquents affiliate with deviant peers also, but such affiliation is more likely to result from selection of peers by youth predisposed to antisocial behavior than from socialization of an adolescent by antisocial peers.
Recent evidence suggests that peer affiliations in adolescence may have effects that persist into young adulthood. Capaldi, Dishion, Stoolmiller, and Yoerger (2001) tested a developmental model of the association between adolescent peer behavior and adult partner violence with 206 male participants in the Oregon Youth Study. They found that observed deviant peer associations at 13-16 years of age were associated with aggression toward romantic partners at 20-23 years of age. This relation was mediated through observed hostile talk about women and antisocial behavior at ages 17-18. Shortt and colleagues (Shortt, Capaldi, Dishion, Bank, & Owen, 2003) found, also using data from the Oregon Youth Study, that the relation between affiliation with antisocial peers in adolescence (ages 15-16) and adulthood (ages 23-24) was mediated by observed antisocial talk in late adolescence (ages 17-18). Finally, Wanner, Vitaro, Carbonneau, and Tremblay (2009), analyzing the Montreal Youth Study, found that adolescent gambling problems (age 16) were associated with adult theft (age 23) in youth who had deviant peer associations in adolescence, but not in youth without such associations.
No study to date has found a similar association between adolescent peer relationships and young adult outcomes associated with sexual risk, but there is evidence for peer effects on sexual risk within adolescence, and such effects are similar to those found for delinquency. This study examines longer-term peer effects on sexual risk.
Individual processes linking adolescent peer relationships and young adult outcomes
Adolescent peer relationships and young adult outcomes may be linked by changes in attitudes or changes in behavior. Changes in behavior due to peer relationships may be facilitated, in part, by brain development during adolescence. The cognitive mechanisms underlying impulse control are developing at the same time that the influence of peers and peer relations is at its zenith. For example, it is now widely acknowledged that executive function may not be fully developed until early adulthood. (Casey et al., 2005; Luna et al., 2001). In addition, early adolescence may be a sensitive period during which environmental events, such as may occur in socialization by peers, can permanently alter brain development (Andersen & Teicher, 2008; Andersen, et al., 2008), affecting the propensity for risky sexual behavior (Luna et al., 2001). Additionally, violation of peer expectations may be a source of psychological pain for adolescents. Imaging studies have produced evidence that violation of norms is associated with activation of the same brain regions that activate when a mistake is noted (Klucharev, Hytönen, Rijpkema, Smidts, & Fernández, 2009). Psychological pain associated with norm violation could be a factor in selection of peers exerting influence on individual attitudes and behavior (Henry, et al., 2007).
Social processes linking adolescent peer relationships and young adult outcomes
The peer relations processes of selection and socialization are processes involved in producing similar levels of delinquent behavior and substance use in adolescents and their peers (Kandel, 1987). Selection refers to adolescents choosing or retaining friends who are like them (Wills & Cleary, 1999). Evidence for selection has been found beginning in kindergarten (Cairns & Cairns, 1994, p. 108), and appears to be a driving mechanism in forming peer groups later in development (Brown, et al., 1997).
Socialization refers to behavior change in individual adolescents that is brought about through the influence of peers (Kandel, 1987). Studies for many years have documented risks posed by deviant peers (Brook, Whiteman, Gordon, & Cohen, 1986; Dishion, Patterson, & Reid, 1988; Elliott, Huizinga, & Ageton, 1985; Hawkins, Catalano, & Miller, 1992; Hawkins, Lishner, & Catalano, 1985; Klein, Forehand, Armistead, & Brody, 1994). Dishion and colleagues (Dishion, Spracklen, Andrews, & Patterson, 1996) observed a process they called deviancy training. Videotaped conversations showed that delinquent adolescents offer advice on deviant activities and reward their friends with verbal and nonverbal indications of approval when the friends talked about deviant activities.
The present study explores the longer-term effects of adolescent peer selection and socialization processes on STI diagnoses and unintended pregnancy in later adolescence and young adulthood. Figure 1 displays the conceptual model of the question addressed in this study. Specifically, to what extent are the peer relationship processes of selection and socialization in adolescence associated with the longer-term outcomes of sexually transmitted infections and unintended pregnancy? It is important to understand the relative strength of selection and socialization processes because they have differing implications for intervention. If peer influence is carried primarily through selection, intervention to form or change individual attitudes would be most effective if offered before adolescence. In contrast, strong socialization effects might suggest a need to enhance protective or resistance mechanisms later in adolescence.
Figure 1.

Theoretical model of the effects of adolescent peer relations on young adult outcomes.
Recent evidence suggests that selection and socialization effects may vary by gender. Henry and colleagues (Henry, et al., 2007) found that girls whose friends believed the costs of sex to be high were less likely to have unprotected sex (i.e., without a condom). Selection effects were stronger among males than among females. Young men tended to choose new friends and retain existing friends whose sexual attitudes were similar to their own. Sexual behavior of both sexes was strongly affected by attitudes of the individual (Deptula, et al., 2005) and of friends (Henry, et al., 2007).
The present study
This study tests three hypotheses about sexually transmitted infections (STI) and unintended pregnancy in young adulthood, and whether those outcomes can be predicted by the peer relations processes of selection and socialization in adolescence. Based on previous evidence and because the personal costs of unintended pregnancy are higher for females than for males, we evaluated variation in these effects by gender. Because of the centrality of attitudes to peer influence processes (Henry, et al., 2007) and intervention strategies (e.g., Prochaska & DiClemente, 1983), we included measures of sexual attitudes as well as sexual behavior in our assessment of peer relations processes in adolescence. The following hypotheses were tested:
Hypothesis 1
Peer socialization in adolescence would affect unintended pregnancy among females as measured in young adulthood. Specifically, we expected to find an indirect effect of early peer attitudes and behavior on unintended pregnancy, through individual attitudes or behavior (the socialization path in Figure 1).
Hypothesis 2
Past findings of stronger selection effects among males (Henry et al., 2007) led us to hypothesize that there would be indirect effects of individual attitudes or sexual behavior on later STI diagnosis among males, through later peer attitudes or behavior (the selection path in Figure 1).
Hypothesis 3
Consistent with previous research, we hypothesized that, for both sexes, the effects of attitudes on STI diagnosis and unintended pregnancy would be stronger than the effects of high risk sexual behavior in adolescence.
Method
Sample
Individuals
The sample for this study consisted of 1087 students participating in the saturated schools sub-sample of the National Longitudinal Study of Adolescent Health (Add Health; Bearman, Jones, & Udry, 1997; Udry, 2003). In this sub-sample, an attempt was made to assess all subjects in each of 9 high schools or feeder schools (middle schools or junior high schools) in order to facilitate analysis of friendship networks. Individuals were included based on 3 criteria: (a) non-missing Wave III data (collected when subjects were 21-26 years of age), (b) non-missing data from at least one of their nominated friends at both Waves I and II, and (c) non-missing individual data in Waves I and II. Table 1 reports demographic characteristics of the sample, in toto, and by gender. The saturated school sub-sample was a convenience sample of schools and was not designed to be nationally representative, as was the full Add-Health sample. The distribution by gender did not differ significantly from the full sample, χ2(1, N=18,022) < 1, ns. The saturated sample had a lower proportion of whites (48.8% vs. 53.3%, p < .01) and African-American youth (15.2% vs. 23.4%, p < .01); and a higher proportion of Asian youth than the remainder of the full Add-Health sample (14.5% vs. 5.1%, p < .01).
Table 1.
Demographic Characteristics and Wave III Outcomes
| Variable | Female | Male | Total |
|---|---|---|---|
| N | 537 | 550 | 1087 |
| Race/Ethnicity | |||
| Latino/Hispanic – N (%) | 107 (19.9%) | 109 (19.8%) | 216 (19.9%) |
| White – N (%) | 325 (60.4%) | 345 (62.5%) | 670 (61.5%) |
| African-American – N (%) | 63 (11.7%) | 47 (8.5%) | 110 (10.1%) |
| American Indian – N (%) | 21 (3.9%) | 25 (4.5%) | 46 (4.2%) |
| Asian or Pacific Islander – N (%) | 104 (19.3%) | 95 (17.2%) | 199 (18.3%) |
| Other – N (%) | 56 (10.4%) | 75 (13.6%) | 131 (12.0%) |
| Mean (SD) Age at Wave I** | 16.57 (0.88) | 16.76 (0.93) | 16.67 (0.91) |
| Mean (SD) Age at Wave III** | 22.43 (0.95) | 22.66 (1.01) | 22.55 (0.98) |
| Any WIII STI Diagnosis – N (%)** | 14 (2.6%) | 12 (2.2%) | 26 (2.4%) |
| WIII Unintended Pregnancy – N (%)** | |||
| One | 110 (19.9%) | 64 (11.6%) | 174 (16.0%) |
| More than one | 11 (2.1%) | 6 (1.1%) | 17 (1.6%) |
| WI Individual Mean (SD) Unprotected Sex Partners | .00 (.24) | .01 (.28) | .01 (.26) |
| WII Individual Mean (SD) Unprotected Sex Partners | .12 (.43) | .08 (.29) | .09 (.36) |
| WI Friends’ Mean (SD) Unprotected Sex Partners | .21 (.38) | .22 (.45) | .22 (.42) |
| WII Friends’ Mean (SD) Unprotected Sex Partners | .14 (.35) | .11 (.24) | .12 (.30) |
| WI Individual Costs Attitudes Mean (SD)* | 3.09 (.68) | 2.98 (.63) | 3.04 (.66) |
| WII Individual Costs Attitudes Mean (SD)* | 3.53 (.72) | 3.45 (.68) | 3.49 (.70) |
| WI Friends’ Costs Attitudes Mean (SD) | 3.51 (.50) | 3.49 (.47) | 3.50 (.48) |
| WII Friends’ Costs Attitudes Mean (SD) | 3.49 (.54) | 3.45 (.48) | 3.47 (.51) |
Note:
p < .05,
p < .01 in tests of gender differences
Race/ethnicity percentages may sum to more than 100%.
Comparing participants who completed the Wave III assessment with those who did not revealed that Wave III participants were slightly younger at Wave I than non-participants, 16.7 yrs. vs. 16.8 yrs, t(1418) = 3.57, p < .01. Controlling for age at Wave I, Wave III participants also were less likely to have initiated sex before Wave II than were non-participants, 47.14% vs. 54.65%, χ2(1, N=1420) = 5.76, p < .05. Wave III participants did not differ from non-participants on gender composition or race.
Friendship networks
In Waves I and II, we used peer nomination data to estimate each participant’s friendship network, regardless of whether friendship nominations were reciprocated or not. This approach is consistent with past research, such as by Ennett and colleagues (2006) in their study of social network effects on drug abuse. As a check of this approach, we compared the results using reciprocated networks to non-reciprocated networks, and found that the results did not differ substantially. Therefore, we chose to use the models using non-reciprocated networks due to the sample size advantages of the approach.
Each student was asked to nominate up to five male and five female friends, separately by sex, in order of preference. Students could nominate any friends but study identification numbers were assigned only to nominated friends who attended the same school or a feeder school. Romantic partners and siblings were not counted as friends, but special codes were provided that allowed identification of youth who nominated siblings or romantic partners among their friends.
Procedures
This study was approved by the Institutional Review Board of the University of Illinois at Chicago. The Wave I Add-Health Study in-home interviews were conducted between April and December 1995, and the Wave II interviews were conducted approximately one year later (Bearman, et al., 1997). All respondents were given the same interview, which took from one to two hours to complete depending on the respondent’s age and experiences. The majority of interviews were conducted in the respondents’ homes. For questions concerning sexual behavior and attitudes, the respondent listened to pre-recorded questions through earphones and entered the answers directly on the computer (audio-CASI). Adolescents younger than 15 years of age were not asked questions regarding their attitudes about sex, and thus were excluded from this study.
The Wave III data (Carolina Population Center, 2004) contained follow-up interviews from original Wave I respondents located by field interviewers between August 2001 and April 2002 (six years after the collection of Wave II data). Participants in Wave III were between 21 and 26 years old. Interviews were conducted mostly in homes, but some interviews were conducted in schools, workplaces, or other public places.
Measures
Individual measures
Demographic variables, including age, gender, ethnicity (using 2000 census categories), and whether or not a romantic partner was identified among friends were assessed in the in-home interview. Self-reports of gender and ethnicity were augmented by interviewer observations.
Unprotected intercourse (Waves I and II)
This was defined as the number of heterosexual partners with whom a subject had engaged in vaginal sexual intercourse without using a condom during the preceding year. Participants reported up to three romantic relationships and three casual encounters in the preceding year. Those who never had intercourse received a score of zero, as did those who reported no relationships or casual encounters in the preceding year. Because the survey queried only six partners (three relationships and three casual encounters), individual scores of unprotected intercourse had an upper limit of six.
Costs attitudes (Waves I and II)
Cost attitudes were assessed using a measure with 9 items anchored by a five-point Likert-type scale representing strong agreement to strong disagreement. Examples of items are “If you had sexual intercourse, you would feel guilty” and “If you got (someone) pregnant you would have to quit school.” This scale has acceptable reliability (alpha = .78) and validity, as evidenced by its ability to predict intercourse both cross-sectionally and longitudinally (Deptula, et al., 2005). Scores ranged from 1.0 to 5.0, and were approximately normally distributed.
Friends’ measures (Waves I and II)
We constructed measures representing friends’ unprotected intercourse and friends’ attitudes about the costs of sex at Waves I and II by taking the mean of the self-report measures of each friend nominated by each adolescent. This procedure provided a single friends’ score on each variable for each individual adolescent in the study. Representing friends’ influence using the mean of friends’ scores has been used in numerous studies of friends’ influence (Henry, et al., 2000; Henry & Kobus, 2007; Kiesner, Poulin, & Nicotra, 2003). We created overall friend scores and scores for same-sex and opposite-sex friends for each adolescent on measures of attitudes and condom non-use.
Late adolescent/young adult outcomes
Reports of sexually transmitted infection (STIs) diagnoses were represented by a binary variable coded 1 if the respondent reported being diagnosed with any of the following STIs in the 12 months preceding the interview: Chlamydia, gonorrhea, trichomoniasis, syphilis, genital herpes, genital warts, human papilloma virus (HPV), bacterial vaginosis, pelvic inflammatory disease (PID), cervicitis or mucopurulent cervicitis (MPC), urethritis (NGU), vaginitis, or HIV infection or AIDS.
We measured the reported number of unintended pregnancies between Waves II and III using items administered for each sexual encounter in the Wave III interview. One question asked whether the encounter had resulted in a pregnancy. We coded a pregnancy as unplanned if the respondent indicated on another question that he/she did not want to have a child at that time or did not want the partner to be the child’s parent. The number of unplanned pregnancies reported was the score for each subject.
Data analysis
We examined the relations of adolescent peer selection and socialization processes to later outcomes using a path model fit through MPLUS 5.2 (Muthén & Muthén, 2007). For this model, STI diagnoses were represented by a binary variable (none, any), and unintended pregnancies were represented by an ordinal variable (none, one, more than one). The model predicted these variables from Wave II individual and peer intercourse without a condom and attitudes about the costs of sex. These Wave II values were, in turn, predicted by Wave I values of these same variables. This strategy allowed us to evaluate the direct effects of Wave II variables on Wave III outcomes, and the indirect effects of Wave I variables on Wave III outcomes. Prior to obtaining the best-fitting model, and because of the gender differences found in previous research (Henry, et al., 2007), we initially fit models to test for gender moderation of each structural path coefficient between Wave II predictors and Wave III outcomes. In each of these tests, a model with all of the structural path coefficients constrained to equality across genders was compared to a model in which a single structural path coefficient was free to vary across genders. Terms for age at Wave I and ethnicity were included as covariates in each model. Covariances within waves, variances, means, and scale parameters were free to vary by gender. All models were fit using mean and variance adjusted weighted least squares (WLSMV) estimation in MPLUS 5.2 (Muthén & Muthén, 2007). The test for the difference in fit between models was based on a saved matrix of derivatives as advocated by Muthén and Muthén (2007). Once it was determined that separate models by gender fit the data better than models constrained to equality across genders, we fit a final multiple group model with all path coefficients freed to vary by gender. We used bootstrapped standard errors for all significance tests of parameters, due to the skewness of the distribution of the outcomes and some predictors.
We fit additional models aimed at clarifying the results. One was a multiple group model that tested the equality of parameters across samples defined by whether or not the adolescent nominated a romantic partner as a peer in Wave I or Wave II. Other models were fit that tested the effects of same- and opposite-sex peer variables. Because not every adolescent in the sample nominated both same- and opposite-sex peers, we fit these models (1) with a sample that nominated peers of both sexes, (2) with a sample including all those who nominated same-sex peers, and (3) with a sample of those who nominated opposite-sex peers.
Because the focus of this study is on the effects of adolescent peer relationships on young adult outcomes, and because of the large number of effects produced by these models, we report only those relations that offer the potential for mediated relations of Wave I variables on Wave III variables through Wave II variables, and interpret mediated effects only when both the Wave I-II and Wave II-III relations are significant (MacKinnon, 2008, p. 395; MacKinnon, Lockwood, Hoffman, West, & Sheets, 2002) or when the bootstrapped confidence interval for the mediated effects did not include zero (MacKinnon, Lockwood, & Williams, 2004). All possible indirect effects were explored and are reported for each significant Wave II to Wave III direct effect.
Results
Table 1 reports the outcome variable proportions and the means and standard deviations of the predictors with tests of gender differences. Females were more likely than males to report at least one STI diagnosis by Wave III, and were significantly more likely than males to report one or more unintended pregnancies. Females also had higher levels of attitudes about the costs of sex than males at both Waves I and II.
The initial multiple-group test of the path between Wave II friends’ attitudes about the costs of sex and Wave III reports of STI diagnoses differed by gender, χ2(1, N = 1087) = 4.50, p < .05. In addition, there were several gender differences on the relations between the attitude and behavior variables and covariates. Accordingly, we report the best fitting models separately by gender.
The final overall model was an excellent fit to the data, according to the appropriate WLSMV chi-square goodness-of-fit test, χ2(32) = 45.15, ns, the comparative fit index of 0.98, and the root mean squared error of approximation of 0.02. In Table 2 we report the full mediated relations for significant Wave II to Wave III effects. Thus, if the path from individual attitudes at Wave II to unintended pregnancy at Wave III was significant, we included tests of all of the Wave I-II relations involving Wave II individual attitudes that suggested the possibility of peer effects. We do not report relations within the same variable across waves or cross-lagged relations within individuals or friends; confining our reporting to adolescent-friend or friend-adolescent relations across waves.
Table 2.
Potential Indirect Effects by Gender (Total Sample, N = 1087)
| WIII Outcome | Initial-Mediator (a) | Mediator-Final (b) | Indirect Effect (ab) | |||
|---|---|---|---|---|---|---|
| WI-WII Indirect Effect | B (SE) | 95% CI | B (SE) | 95% CI | B (SE) | 95% CI |
| Females (n = 537) | ||||||
| Unintended Pregnancy (Socialization Effect) | ||||||
| Friends’ Behavior - Individual Attitudes | -0.11 (.07)+ | -.24 to .02 | -0.35 (0.09)** | -.54 to -.17 | 0.04 (.03) | -.01 to .10 |
| Friends’ Attitudes - Individual Attitudes | 0.08 (0.05)+ | -.01 to .17 | -0.35 (0.09)** | -.54 to -.17 | -0.03 (0.02) | -.07 to .01 |
| Males (n = 550) | ||||||
| Unintended Pregnancy (Socialization Effect) | ||||||
| Friends’ Behavior – Individual Attitudes | -0.09 (0.05)+ | -.19 to .00 | -0.26 (.11)* | -.47 to -.05 | 0.03 (0.02) | -.01 to .09 |
| Friends’ Attitudes - Individual Attitudes | 0.19 (.06)** | .07 to .30 | -0.26 (.11)* | -.47 to -.05 | -0.05 (.03) + | -.07 to .01 |
| STI Diagnoses (Selection Effect) | ||||||
| Individual Attitudes - Friends’ Attitudes | 0.09 (.03)** | .03 to .16 | -0.58 (.22)** | -1.0 to -.16 | -0.03 (.02) * | -.06 to 0.0 |
| Individual Behavior – Friends’ Attitudes | -0.04 (.07) | -.18 to .09 | -0.58 (.22)** | -1.0 to -.16 | 0.03 (.05) | -.07 to .12 |
p < .10.
p < .05.
p < .01.
Youth who considered sex to have higher costs at Wave II (~ age 17) were less likely to report unintended pregnancy at Wave III (~ age 24). This effect was significant for females, B = -.35, SE = .09, t(535) = 3.74, p < .01, and for males, B = -.26, SE = .11, t(548) = 2.42, p < .05. Males whose friends considered sex to have higher costs at Wave II also were less likely to report STI diagnoses at Wave III, B = -.58, SE = .22, t(548) = 2.68, p < .01. Given the significant relations between individual attitudes and unintended pregnancy in both males and females, and between individual attitudes and STI diagnoses among males, we tested the possible indirect effects on these outcomes of Wave I friends’ attitudes and behavior through Wave II individual attitudes. All of these effects were consistent with socialization by peers. Among females, having friends who were less likely to engage in risky sexual behavior (B = -.11, SE = .07, Z = 1.74, p < .10) and having friends who viewed sex as having higher costs (B = .08, SE = .05, Z = 1.68, p < .10) both were marginally associated with believing sex had higher costs one year later in Wave II. Neither product test of indirect effects was significant.
Among males, having friends engaging in less risky sexual behavior was marginally associated with adolescents’ beliefs that sex had higher costs at Wave II, B = -.09, SE = .05, Z = 1.91, p < .10. Friends’ attitudes that sex had higher costs at Wave I was significantly associated with the adolescent believing sex to have higher costs at Wave II, B = .19, SE = .06, Z = 3.28, p < .01.
In Figure 2 we illustrate paths with significant evidence consistent with indirect effects in the full sample. For the young adult outcome of unintended pregnancy, the test of the indirect effect of Wave I friends’ behavior through individual attitudes was not significant, but the test of the indirect effect of Wave 1 friends’ attitudes through individual attitudes was marginal (B = -.05, SE = .03, Z = 1.85, p < .10). Despite this, by the joint significance criterion (MacKinnon, et al., 2002), there was evidence that, among males, friends’ attitudes affected unintended pregnancy through individual attitudes.
Figure 2.
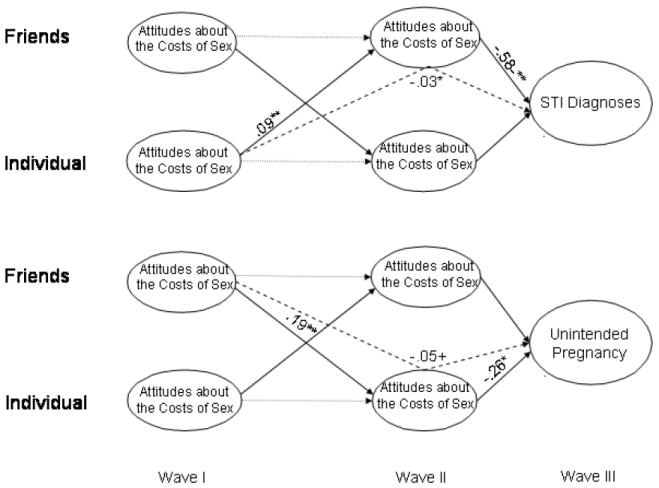
Mediated paths for STI Diagnoses and Unintended Pregnancies among Males. Total Sample, N = 1087. Note: Indirect effects are indicated by dashed lines. + p < .10. * p < .05. ** p < .01.
Because the effect of Wave II friends’ attitudes was significant for STI diagnoses among males, we tested for indirect effects consistent with peer selection. Adolescent males who in Wave I believed sex to have higher costs tended to have friends at Wave II who believed similarly (B = .09, SE = .03, Z = 2.76, p < .01), but risky sexual behavior at Wave I was not significantly related to friends’ attitudes at Wave II. Only the indirect effect test of the effect of individual Wave I attitudes on STI diagnoses through Wave II friend attitudes among males was significant, B = -.03, SE = .02, Z = 1.97, p < .05, and the joint significance criterion also suggested an indirect effect.
Effects Involving Same-sex vs. Opposite-sex Friends
We also tested the model with separate scores for same-sex and opposite-sex friends, using the subsample of youth who reported friends of both sexes. This model, like the main analysis, was an excellent fit to the data, χ2(44, N=731) = 50.82, ns; CFI = .98; RMSEA = .02. The results of this analysis are reported in Table 3. As can be seen there, the socialization effects found with the full sample appear to be a function of the attitudes of same sex peers rather than those of opposite sex peers.
Table 3.
Potential Indirect Effects by Gender (Sample Reporting Same-sex and Opposite-sex Friends, N = 731)
| WIII Outcome | Initial-Mediator (a) | Mediator-Final (b) | Indirect Effect (ab) | |||
|---|---|---|---|---|---|---|
| WI-WII Effect | B (SE) | 95% CI | B (SE) | 95% CI | B (SE) | 95% CI |
| Females (n = 377) | ||||||
| Unintended Pregnancy (Socialization Effects) | ||||||
| Same Sex Friends’ Attitudes - Individual Attitudes | 0.04 (.02)* | .01 to .17 | -0.30 (0.12)* | -.54 to -.17 | 0.03 (0.02)+ | -.07 to .01 |
| Opposite Sex Friends’ Attitudes – Individual Attitudes | 0.01 (.01) | -.02 to .03 | -0.30 (0.12)* | -.54 to -.17 | 0.002 (.004) | -.006 to .009 |
| Same Sex Friends’ Behavior – Individual Attitudes | -0.02 (.05) | -.11 to .07 | -0.30 (0.12)* | -.54 to -.17 | 0.00 (.001) | -.02 to .03 |
| Opposite Sex Friends Behavior – Individual Attitudes | -0.01 (.05) | -.11 to .08 | -0.30 (0.12)* | -.54 to -.17 | 0.003 (.01) | -.02 to .03 |
| Unintended Pregnancy (Selection Effects) | ||||||
| Individual Attitudes- Same-sex Friends’ Attitudes | 0.37 (.06)** | .25 to .50 | -0.26 (.12)* | .03 to .49 | -0.10 (.05)* | -.19 to -.01 |
| Individual Behavior - Same-sex Friends’ Attitudes | -0.24 (.17) | -.57 to .09 | -0.26 (.12)* | .03 to .49 | .06 (.05) | -.04 to .15 |
| Males (n = 354) | ||||||
| Unintended Pregnancy | ||||||
| Same Sex Friends’ Attitudes– Individual Attitudes | 0.02 (0.02) | -.01 to .05 | -0.37 (.14)** | -.47 to -.05 | 0.03 (0.02) | -.01 to .09 |
| Opposite Sex Friends’ Attitudes – Individual Attitudes | 0.02 (.01) | -.05 to .01 | -0.37 (.14)** | -.47 to -.05 | -0.02 (.01) + | -.07 to .01 |
| Same Sex Friends’ Behavior – Individual Attitudes | -0.06 (.05) | -.15 to .04 | -0.37 (.14)** | -.47 to -.05 | 0.02 (.02) | -.02 to .06 |
| Opposite Sex Friends Behavior – Individual Attitudes | 0.02 (.05) | -.07 to .11 | -0.37 (.14)** | -.47 to -.05 | -.006 (.02) | -.04 to .03 |
| STI Diagnoses | ||||||
| Same Sex Friends’ Attitudes– Individual Attitudes | -0.02 (0.02) | -.05 to .01 | -0.33 (.18)+ | -.67 to .02 | .007 (.006) | -.004 to .02 |
| Opposite Sex Friends’ Attitudes – Individual Attitudes | -0.02 (.01) | -.05 to .01 | -0.33 (.18)+ | -.67 to .02 | 0.01 (.01) | -.005 to .02 |
| Same Sex Friends’ Behavior – Individual Attitudes | -0.06 (.05) | -.15 to .04 | -0.33 (.18)+ | -.67 to .02 | .02 (.02) | -.02 to .06 |
| Opposite Sex Friends Behavior – Individual Attitudes | 0.02 (.05) | -.07 to .11 | -0.33 (.18)+ | -.67 to .02 | -0.005 (.01) | -.04 to .03 |
Note:
p < .10.
p < .05.
p < .01
Model fit: χ2(44, N = 731) = 50.82, ns; CFI = .98; RMSEA = .02
Among females, the effect of Wave I same sex friends’ attitudes on Wave II adolescent attitudes was significant (B = .04, SE = .02, Z = 2.24, p < .05) but the effects on individual attitudes of opposite-sex friend attitudes and behavior of friends of both sexes were not significant. It should also be noted from Table 3 that when same- and opposite-sex friend attitudes were considered separately, there emerged a selection effect that had not been present in the overall analysis. Females who perceived higher costs of sex at Wave I tended to have same-sex friends whose attitudes were similar at Wave II (B = .37, SE = .07, Z = 5.76, p < .01), and same-sex friends’ attitudes at Wave II were significant predictors of unintended pregnancies in young adulthood (B = -.26, SE = .12, Z = 2.19, p < .05). The test of the ab indirect effect in this analysis also was significant (B = -.10, SE = .05, Z = 2.08, p < .05). Figure 3 illustrates the paths for which there was evidence of significant indirect effects, either from the product tests or the joint significance method, or both.
Figure 3.
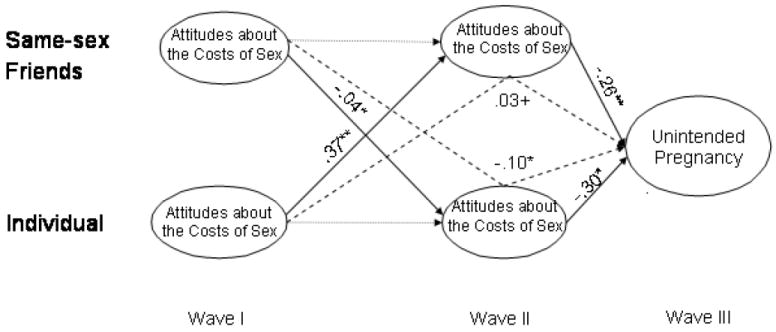
Mediated paths for Unintended Pregnancies among Females. Same-sex Friends Sample, N = 731. Note: Indirect effects are indicated by dashed lines. + p < .10. * p < .05. ** p < .01
Among males there remained a significant association between Wave II attitudes of adolescents and Wave III unintended pregnancies (B = -.37, SE = .14, Z = 2.62, p < .01) and a marginal relation of Wave II attitudes with Wave III STI diagnoses (B = -.33, SE = .18, Z = 1.82, p < .10). However in analyses separating same- and opposite sex friends, no significant Wave I-II associations and no significant indirect effects emerged.
Differences in Effects by Nomination of a Romantic Partner
As was noted above, Add Health did not include the ID numbers of romantic partners or siblings who were nominated as friends. Because we used the research ID numbers of nominated friends to construct the friend measures, the effects of friends’ attitudes and behaviors reported in this study are solely the effects of friends who were not romantic partners or siblings. The inclusion of a special code in place of an ID number when a romantic partner was nominated made it possible to test whether nomination of a romantic partner was associated with differences in the obtained effects. Using the special code as an indicator, we formed two subsamples: One including those who did not nominate a romantic partner at either Wave I or Wave II (n = 799), and the other including those who nominated a romantic partner at either Wave I or Wave II (n = 288).
A multiple group model fixing structural paths to equality across groups defined by nomination of a romantic partner showed no significant evidence of difference from a similar model that freed the structural paths, χ2(8, N=1087) = 2.46, ns. This suggests that the results are consistent across individuals with and without romantic partners.
Magnitude of the Effects
One measure of the strength of the overall effects is the multiple correlation coefficients for reported STI diagnoses and unintended pregnancy from the main MPLUS analysis. Among females, three percent (R2 = .032) of the variance in reported STI diagnoses and nine percent (R2 = .090) of the variance in unintended pregnancies was accounted for by the model. Among males, these figures were 13% (R2 = .13) and four percent (R2 = .04) respectively. An assessment of the magnitude of the effects of friends’ attitudes comes from the rates of the outcomes at different average levels of the friends’ costs attitudes measure. Females whose friends had scores representing disagreement to neutrality on the costs of sex had rates of 5.4 reported STI diagnoses and 62.7 unintended pregnancies per thousand per year, and those whose friends scored between neutrality and agreement had rates of 3.2 reported STI diagnoses and 37.6 unintended pregnancies per thousand per year. Among males, those whose friends scored between disagree and neutral had rates of 7.3 reported STI diagnoses and 31.1 unintended pregnancies per thousand per year, and those whose friends’ attitudes were between neutral and agree had rates of 3.3 reported STI diagnoses and 23.0 unintended pregnancies per thousand per year.
Discussion
This study tested a model of the effects of adolescent peer relations processes on reports of STI diagnoses and unintended pregnancies measured approximately six years after the peer relations processes were assessed.
Evaluation of Hypotheses
Our first hypothesis was that socialization processes in adolescence would be associated with unintended pregnancy among females. This hypothesis received partial support. Among females, perceiving sex to have higher costs in late adolescence is associated with lower likelihood of unintended pregnancy reported in young adulthood, and the attitudes of female friends earlier in adolescence appear to have a role in that relation. Surprisingly, a similar effect was found for males. Friends’ attitudes influence individual attitudes one year later, and individual attitudes in late adolescence are associated with reports of unintended pregnancy in young adulthood.
Our second hypothesis expected selection effects on STI diagnoses among males. The evidence is consistent with the notion that male adolescents select or retain friends who have similar attitudes about the costs of sex, and this mediated relation is associated with STI diagnoses in young adulthood. Surprisingly it also appears that female adolescents select and/or retain female friends with similar attitudes and that this process in adolescence is associated with unintended pregnancy in young adulthood.
Our third hypothesis also received partial support. We expected evidence that selection and socialization effects would operate through friends’ attitudes rather than through friends’ behavior, and most of the obtained effects were consistent with that expectation. However, for both males and females there was marginal evidence that friends’ behavior in early adolescence affects individual attitudes in later adolescence.
Implications for Development
Peer relations processes in adolescence affect young adult STI diagnoses and unintended pregnancies, but the nature of these relations found in these analyses is counterintuitive. Females’ greater social orientation (Cross & Madson, 1997) led us to expect that females would be more influenced by attitudes and behaviors of friends than males (socialization), but only marginal evidence consistent with long-term effects of socialization was found among females. Surprisingly, the only significant indirect effects, according both to joint significance tests and product mediation tests, were found among males.
Finding that attitudes appear to bridge adolescent peer relations and later outcomes is consistent with emerging evidence about the persistence of characteristics between childhood and adulthood, the importance of environmental factors in brain development, and the likelihood that such development is taking place precisely at the time when peer relations have their greatest influence. Attitudes formed in relationships with peers during adolescence have detectible effects on the consequences of risk behaviors measured in young adulthood. Although studies of antisocial behavior development link peer relations in adolescence with young adult outcomes, our literature review found no previous study making such a connection in the area of sexual risk. That the present study demonstrates such a link serves to underscore the potential importance of peer relations as a factor in planning interventions to reduce STI risk or unintended pregnancy.
When compared with previous research, the results of this study suggest that the peer-relations processes involved in adolescent risk behaviors and the processes that best predict adult outcomes may differ. Wills and colleagues (2003) examined the predictors of substance use and sexual behavior in a sample of African American early adolescents. They found that individual attitudes toward persons who engaged in sex (prototype perceptions) were related to sexual behavior, mediated by friends’ sexual behavior, consistent with a selection effect. Henry and colleagues’ (2007) results also suggest that peer selection has somewhat stronger effects than socialization during adolescence, except among females, for whom peer socialization effects were found on attitudes and intercourse without a condom. The present study found little evidence for selection effects on the longer-term outcomes of unintended pregnancy and self-reported STI diagnoses.
Despite inconsistencies between the influence processes important in adolescence and those linking adolescence with adult outcomes, this study, like previous research findings (Henry, et al., 2007; Wills, et al., 2003), underscores the pivotal role of attitudes in sexual risk. Attitudes about the costs of sexual activity had effects on later unintended pregnancies among both males and females and effects on STI diagnoses among males.
Implications for Intervention
These results may have implications for practice and intervention, most of which stem from the finding that attitudes are important in peer influence and longer-term outcomes. Sex education and/or relationship education programs are conducted in over 90% of public schools (Sabia, 2006), and the curricula for such programs typically include sessions on peer pressure. The results of this study suggest that it may be important to add discussion of the attitudes of peers and the desire to imitate peers to the topics addressed in such programs. Such discussions may be particularly important with adolescent males. Although there were short-term socialization and selection effects among males and females, only among males were socialization and selection processes linked to young adult outcomes.
The centrality of attitudes in the effects found in this study supports existing intervention strategies based on exploring and changing attitudes, such as the Transtheoretical Model of Change (Prochaska & DiClemente, 1983). Additionally, the centrality of attitudes in these results suggests the potential value of feeding back information on the normative attitudes of peers as part of an intervention strategy. Interventions that provide feedback on the norms of peers have been widely applied in alcohol prevention to reduce risk by correcting misperceptions of peer norms. The important role of friends’ attitudes found in this study suggests that such interventions also may be effective for sexual risk (Wechsler, et al., 2003).
There is evidence that normative feedback interventions may be effective in reducing sexual risk. Chernoff and Davison (2005) found that men randomly assigned to receive normative feedback on sexual behavior increased condom use and women assigned to normative feedback decreased the number of sexual partners, both relative to treatment-as-usual controls. The feedback provided was on sexual behavior of peers. The importance of attitudes in this study suggests that further research is needed to determine whether normative feedback on peer attitudes in the context of preventive intervention can also reduce risky sexual behavior.
This study also suggests, consistent with previous research (e.g., Capaldi, et al., 2001) that individual attitudes may be the link between adolescent peer relationships and young adult outcomes. Investigation of how and when, developmentally, peer relationships shift individual attitudes would be another important focus of future research. Shortt and colleagues’ (2003) findings suggest that conversations with deviant peers may contribute to attitude change. Because of the mobility of families and the emergence of other influential relationships (e.g., marital partners and children) in young adulthood, it is unlikely that persistence of adolescent friendships into young adulthood connects peer risk in adolescence to adult outcomes. Future research should also explore the neurodevelopmental factors that affect the association between peer relationships and changes in attitudes and behaviors of adolescents and young adults.
Limitations
There are some important limitations that should be considered when interpreting these results. First, the sample consisted solely of students in the saturated school sample of the Add Health data set. This sub-sample attempted to assess all students in each school. It was designed to permit study of peer relationships but is not representative of the U.S. population as a whole. Second, in order to maximize the available sample size we used non-reciprocated as well as reciprocated friendship nominations to represent friends’ influence on the individual. The limitation of this method is that we cannot differentiate between the effects of actual and desired friendships, although it has been argued that desired or perceived friendships are as important as actual friendships when assessing peer influence (Brown, et al., 1992). Third, the Add Health data set did not provide information that would allow us to construct a measure of the number of incidents of sex without a condom, which would have been preferable for predicting unintended pregnancy particularly. Fourth, it is possible that the power to detect significant effects of friends’ behavior may have been limited, relative to the power provided by the attitude measures, because of the low base rate of high risk sex among adolescents. We used methods appropriate for predicting binary and ordinal data to further assure the accuracy of our significance tests, but these measures would not address a potential power differential. A fifth limitation is the difference in time frame for assessing unintended pregnancies (past 6 years) and STI diagnoses (preceding 12 months). We would have preferred a longer-term assessment of STI diagnoses, but 12 months was the time frame use in the Add Health study. Because sexual risk is inextricably tied to romantic partners, a sixth limitation is our inability to assess or control for the effects of romantic partners on the outcomes. There is no way of eliminating romantic partners of participants who were included in the sample. Their inclusion would have tended to inflate the effects as each time a romantic partner was included, the relationship would have twice the influence on the effect as would have been the case if only one partner were counted. We did, however, determine that the obtained effects did not differ between those who did and did not nominate a romantic partner, evidence that such inflation of effects may not be present to any great extent. Finally, as was noted in the sample description, the sample that completed the Wave III assessment had slightly lower sexual risk at Wave I than did those who did not complete the Wave III assessment. This difference in risk due to attrition is consistent with attrition of higher risk youth found in other studies, and suggests that the effects found in this study may be conservative estimates of population effects.
Despite these limitations, the results of this study move forward our understanding of the role of peer relationships in risk for sexually-transmitted infections and unintended pregnancy. They underscore the importance of attitudes in the transmission of risk from adolescence to adulthood. Such knowledge may be useful for increasing the effectiveness of clinical practice and preventive interventions.
Acknowledgments
This article was supported by grant R01-HD052444 from the National Institute on Child Health and Human Development to the first author. It is based, in part, on a paper presented at the 2008 biennial meeting of the Society for Research on Adolescence. This research uses data from Add Health, a program project directed by Kathleen Mullan Harris and designed by J. Richard Udry, Peter S. Bearman, and Kathleen Mullan Harris at the University of North Carolina at Chapel Hill, and funded by grant P01-HD31921 from the Eunice Kennedy Shriver National Institute of Child Health and Human Development, with cooperative funding from 23 other federal agencies and foundations. Special acknowledgment is due Ronald R. Rindfuss and Barbara Entwisle for assistance in the original design. Information on how to obtain the Add Health data files is available on the Add Health website (http://www.cpc.unc.edu/addhealth). No direct support was received from grant P01-HD31921 for this analysis.
References
- Andersen SL, Teicher MH. Stress, sensitive periods and maturational events in adolescent depression. Trends in Neurosciences. 2008;31(4):183–191. doi: 10.1016/j.tins.2008.01.004. [DOI] [PubMed] [Google Scholar]
- Andersen SL, Tomada A, Vincow ES, Valente E, Polcari A, Teicher MH. Preliminary evidence for the sensitive periods in the effect of childhood sexual abuse on regional brain development. The Journal of Neuropsychiatry and Clinical Neurosciences. 2008;20(3):292–301. doi: 10.1176/appi.neuropsych.20.3.292. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bearman PS, Jones J, Udry JR. The National Longitudinal Study of Adolescent Health: Research Design [WWW document] 1997 [Google Scholar]
- Brook JS, Whiteman M, Gordon AS, Cohen P. Dynamics of childhood and adolescent personality traits and adolescent drug use. Developmental Psychology. 1986;22:403–414. [Google Scholar]
- Brown BB, Dolcini MM, Leventhal A. Transformations in peer relationships at adolescence: Implications for health-related behavior. In: Schulenberg J, Maggs JL, Hurrelmann K, editors. Health risks and developmental transitions during adolescence. New York, NY: Cambridge University Press; 1997. pp. 161–189. [Google Scholar]
- Brown LK, DiClemente RJ, Park T. Predictors of condom use in sexually active adolescents. Journal of Adolescent Health. 1992;13:651–657. doi: 10.1016/1054-139x(92)90058-j. [DOI] [PubMed] [Google Scholar]
- Buhi ER, Goodson P. Predictors of adolescent sexual behavior and intention: A theory-guided systematic review. Journal of Adolescent Health. 2007;40:4–21. doi: 10.1016/j.jadohealth.2006.09.027. [DOI] [PubMed] [Google Scholar]
- Cairns RB, Cairns BD. Lifelines and Risks: Pathways of Youth in Our Time. New York, NY: Harvester-Wheatsheaf; 1994. [Google Scholar]
- Capaldi DM, Dishion TJ, Stoolmiller M, Yoerger K. Aggression toward female partners by at-risk young men: The contribution of male adolescent friendships. Developmental Psychology. 2001;37(1):61–73. [PubMed] [Google Scholar]
- Carolina Population Center. National Longitudinal Study of Adolescent Health: Wave III Data Documentation 2004 [Google Scholar]
- Centers for Disease Control and Prevention. Trends in reportable sexually transmitted diseases in the United States, 2007. 2009 http://www.cdc.gov/STI/stats07/trends.htm.
- Chernoff RA, Davison GC. An evaluation of a brief HIV/AIDS prevention intervention for college students using normative feedback and goal setting. AIDS Education and Prevention. 2005;17:91–104. doi: 10.1521/aeap.17.3.91.62902. [DOI] [PubMed] [Google Scholar]
- Cross SE, Madson L. Models of the self: Self-construals and gender. Psychological Bulletin. 1997;122(1):5–37. doi: 10.1037/0033-2909.122.1.5. [DOI] [PubMed] [Google Scholar]
- Deptula D, Henry D, Schoeny ME, Slavick J. Adolescent sexual behavior and attitudes: A costs and benefits approach. Journal of Adolescent Health. 2005;38:35–43. doi: 10.1016/j.jadohealth.2004.08.026. [DOI] [PubMed] [Google Scholar]
- Derlega VJ, Barbee AP. HIV and social interaction. Thousand Oaks, CA, US: Sage Publications, Inc; 1998. [Google Scholar]
- Dishion T, Patterson GR, Reid J. Parent and peer factors associated with early adolescent drug use: Implications for treatment. In: Rahdert E, Grabowski J, editors. Adolescent drug abuse: Analyses of treatment research: NIDA Research Monograph. Vol. 77. Washington, DC: U.S. Government Printing Office; 1988. pp. 69–93. [PubMed] [Google Scholar]
- Dishion TJ, Spracklen KM, Andrews DW, Patterson GR. Deviancy training in male adolescents friendships. Behavior Therapy. 1996;27:373–390. [Google Scholar]
- Elliott D, Huizinga D, Ageton S. Explaining delinquency and drug use. Beverly Hills, CA: Sage; 1985. [Google Scholar]
- Ennett ST, Bauman KE, Hussong A, Faris R, Foshee VA, Cai L, et al. The peer context of adolescent substance use: Findings from social network analysis. Journal of Research on Adolescence. 2006;16(2):159–186. [Google Scholar]
- Fisher TD. Family foundations of sexuality. In: Harvey JH, Wenzel A, Sprecher S, editors. The Handbook of Sexuality in Close Relationships. Hillsdale, NJ: Lawrence Erlbaum Associates; 2004. [Google Scholar]
- Hawkins JD, Catalano RF, Miller JY. Risk and protective factors for alcohol and other drug problems in adolescence and early adulthood: Implications for substance abuse prevention. Psychological Bulletin. 1992;112:64–105. doi: 10.1037/0033-2909.112.1.64. [DOI] [PubMed] [Google Scholar]
- Hawkins JD, Lishner DM, Catalano RF. Childhood predictors and the prevention of adolescent substance abuse. National Institute on Drug Abuse: Research Monograph Series. 1985;56:75–126. [PubMed] [Google Scholar]
- Henry D, Guerra NG, Huesmann LR, Tolan PH, VanAcker R, Eron LD. Normative influences on aggression in urban elementary school classrooms. American Journal of Community Psychology. 2000;28:59–81. doi: 10.1023/A:1005142429725. [DOI] [PubMed] [Google Scholar]
- Henry D, Kobus K. Early adolescent social networks and substance use. Journal of Early Adolescence. 2007;27:346–362. [Google Scholar]
- Henry D, Schoeny M, Deptula D, Slavick J. Peer selection and socialization effects on adolescent intercourse without a condom and attitudes about the costs of sex. Child Development. 2007;78:825–838. doi: 10.1111/j.1467-8624.2007.01035.x. [DOI] [PubMed] [Google Scholar]
- Kandel DB. Homophily, selection, and socialization in adolescent friendships. Substance Use & Misuse. 1987;22(4):319–342. [Google Scholar]
- Kiesner J, Poulin F, Nicotra E. Peer relations across contexts: Individual-network homophily and network inclusion in and after school. Child Development. 2003;74:1328–1343. doi: 10.1111/1467-8624.00610. [DOI] [PubMed] [Google Scholar]
- Klein K, Forehand R, Armistead L, Brody G. Adolescent family predictors of substance use during early adulthood: A theoretical model. Advances in Behaviour Research & Therapy. 1994;16:217–252. [Google Scholar]
- Klucharev V, Hytönen K, Rijpkema M, Smidts A, Fernández G. Reinforcement learning signal predicts social conformity. Neuron. 2009;61(1):140–151. doi: 10.1016/j.neuron.2008.11.027. [DOI] [PubMed] [Google Scholar]
- MacKinnon DP. Introduction to Statistical Mediation Analysis. New York, NY: Lawrence Erlbaum Associates; 2008. [Google Scholar]
- MacKinnon DP, Lockwood CM, Hoffman JM, West SG, Sheets V. A comparison of methods to test mediation and other intervening variable effects. Psychological Methods. 2002;7(1):83–104. doi: 10.1037/1082-989x.7.1.83. [DOI] [PMC free article] [PubMed] [Google Scholar]
- MacKinnon DP, Lockwood CM, Williams J. Confidence limits for the indirect effect: Distribution of the product and resampling methods. Multivariate Behavioral Research. 2004;39:99–128. doi: 10.1207/s15327906mbr3901_4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McPherson M, Smith-Lovin L, Cook J. Birds of a feather: Homophily in social networks. Annual Review of Sociology. 2001;27:415–444. [Google Scholar]
- Miller BC, Benson B, Galbraith KA. Family relationships and adolescent pregnancy risk: A research synthesis. Developmental Review. 2001;21:1–38. [Google Scholar]
- Moffitt TE. Adolescent-limited and life-course-persistent antisocial behavior: a developmental taxonomy. Psychol Rev. 1993;100(4):674–701. [PubMed] [Google Scholar]
- Muthén LK, Muthén BO. Mplus user’s guide. 5. Los Angeles, CA: Muthén & Muthén; 2007. [Google Scholar]
- Ozer EJ, Weinstein RS, Maslach C, Siegel D. Adolescent AIDS prevention in context: The impact of peer educator qualities and classroom environments on intervention efficacy. American Journal of Community Psychology. 1997;25:289–323. doi: 10.1023/a:1024624610117. [DOI] [PubMed] [Google Scholar]
- Potterat JJ, Rothenberg RB, Muth SQ. Network structural dynamics and infectious disease propagation. International Journal of STD and AIDS. 1999;10:182–185. doi: 10.1258/0956462991913853. [DOI] [PubMed] [Google Scholar]
- Prochaska JO, DiClemente CC. Stages and processes of self-change of smoking: Toward an integrative model of change. Journal of Consulting and Clinical Psychology. 1983;51:390–395. doi: 10.1037//0022-006x.51.3.390. [DOI] [PubMed] [Google Scholar]
- Sabia JJ. Does sex education affect adolescent sexual behaviors and health? Journal of Policy Analysis and Management. 2006;25(4):783–802. doi: 10.1002/pam.20208. [DOI] [PubMed] [Google Scholar]
- Shafili T, Stovel K, Holmes K. Association between condom use at sexual debut and subsequent sexual trajectories: A longitudinal study using biomarkers. American Journal of Public Health. 2007;97:1090–1095. doi: 10.2105/AJPH.2005.068437. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shortt JW, Capaldi DM, Dishion TJ, Bank L, Owen LD. The role of adolescent friends, romantic partners, and siblings in the emergence of the adult antisocial lifestyle. Journal of Family Psychology. 2003;17(4):521–533. doi: 10.1037/0893-3200.17.4.521. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Udry JR. The National Longitudinal Study of Adolescent Health (Add Health), Waves I & II, 1994–1996; Wave III, 2001–2002 [machine-readable data file and documentation] Chapel Hill, NC: Carolina Population Center, University of North Carolina at Chapel Hill; 2003. [Google Scholar]
- Wagstaff DA, Delamater JD, Havens KK. Subsequent infection among adolescent African-American males attending a sexually transmitted disease clinic. Journal of Adolescent Health. 1999;25:217–226. doi: 10.1016/s1054-139x(99)00025-7. [DOI] [PubMed] [Google Scholar]
- Walter HJ, Vaughan RD, Gladis MM, Ragin DF. Factors associated with AIDS-related behavioral intentions among high school students in an AIDS epicenter. Health Education Quarterly. 1993;20:409–420. doi: 10.1177/109019819302000310. [DOI] [PubMed] [Google Scholar]
- Wanner B, Vitaro F, Carbonneau R, Tremblay RE. Cross-lagged links among gambling, substance use, and delinquency from midadolescence to young adulthood: Additive and moderating effects of common risk factors. Psychology of Addictive Behaviors. 2009;23(1):91–104. doi: 10.1037/a0013182. [DOI] [PubMed] [Google Scholar]
- Wechsler H, Nelson TE, Lee JE, Seibring M, Lewis C, Keeling RP. Perception and reality: A national evaluation of social norms marketing interventions to reduce college students’ heavy alcohol use. Journal of Studies of Alcohol. 2003;64:484–494. doi: 10.15288/jsa.2003.64.484. [DOI] [PubMed] [Google Scholar]
- Wills TA, Cleary SD. Peer and adolescent substance use among 6th-9th graders: Latent growth analyses of influence versus selection mechanisms. Health Psychology. 1999;18:453–463. doi: 10.1037//0278-6133.18.5.453. [DOI] [PubMed] [Google Scholar]
- Wills TA, Gibbons FX, Gerrard M, Murry VM, Brody GH. Family communication and religiosity related to substance use and sexual behavior in early adolescence: A test for pathways through self-control and prototype perceptions. Psychology of Addictive Behaviors. 2003;17(4):312–323. doi: 10.1037/0893-164X.17.4.312. [DOI] [PubMed] [Google Scholar]
- Wood MD, Nagoshi CT, Dennis DA. Alcohol norms and expectations as predictors of alcohol use and problems in a college student sample. American Journal of Drug and Alcohol Abuse. 1992;18:461–476. doi: 10.3109/00952999209051042. [DOI] [PubMed] [Google Scholar]
- Worth D, Rodriguez R. Latina women and AIDS. SIECUS Rep. 1987:5–7. [PubMed] [Google Scholar]