

Abstract
Background:
Increase in the prevalence of hypertension, obesity and obesity related diseases has become significant cause of disability and premature death in both developing and newly developed countries, with over bearing demand on national health budgets.
Aim:
To evaluate the impact of various levels of education on obesity and blood pressure.
Materials and Method:
325 male and 254 female Nigerians of ages 20-80 years of the Ibo ethnicity through random sampling, were selected for this study. The participants were broken into three major groups based on their educational levels; primary, secondary and tertiary levels. systolic and diastolic blood pressure (SBP & DBP) levels, body mass index (BMI), waist hip ratio (WHR), waist height ratio (WHtR), waist circumference (WC),various skin fold thicknesses, and other anthropometric parameters were measured.
Result:
For all the indicators of subcutaneous fat, general obesity, and central obesity, largest mean deposition was noted to be highest in the lowest education group and least in the highest education group. Mean blood pressure parameters were also highest in the least education group. While fat deposition was noted to be highest in all the females of all the groups, the males showed larger mean BP values. Education was noted to have a significant inverse relationship with most of the fat indicators and blood pressure parameters and cardiovascular disease risk highest in the least education groups.
Conclusion:
Education showed a significant impact on obesity and blood pressure and could be one of the major tools to reduce the high prevalence of obesity, hypertension and other obesity associated diseases.
Keywords: Anthropometry, obesity, adiposity, blood pressure, BMI, obesity prevalence, obesity related disorder, hypertension, cardiovascular disease risk, waist hip ratio
Introduction
The exponential unabated rise in the prevalence of overweight and obesity and their associated risk factors in both developed and developing countries has become a source of concern now than it has ever been in the past[1]. Over one billion adults worldwide have been estimated to be overweight and at least three hundred million of those are considered to be clinically obese[2]. Several factors have been associated with this trend range from changes in the physical, social and economic way of life and environments of the people[3], to genetic and physiologic factors.
Education is one of the media that influences greatly the attitude, social, economic and physiologic behaviors of the people. Many studies have established relationship between education and socioeconomic status (SES)[4–6]. While education can be seen to influence both SES and obesity, a number of works has been done on the relationship of obesity and SES, but the same cannot be said for obesity and education.
Part of the growing concern in the increasing rate of obesity and overweight is the varying rates at which they are distributed across social groups, by levels of education, SES and ethnic background. Lipowics[7] commented on the increase in the association between obesity and higher social class among men, women and children in developing countries, but noted a strong inverse relationship between obesity and social class only among women in developed countries. While Sobal and Stunkard[8] noted inconsistent and general non-linear direction in the relationship of obesity and SES in men and children, they noted consistent relationship with women, where obesity was more prevalent in women of low SES, than those of upper SES.
In view of the present increase in the prevalence of obesity in developing countries[9] and accelerated increase in blood pressure (BP) amongst black population adopting western lifestyle[10]. This work has been designed to determine the impact of education on obesity and BP in the Ibo ethnic group of Nigeria.
Subjects and Methods
This was based on a random sampling of 567 subjects aged 20 to 80 years of the Ibo ethnic group of Nigeria. This is of the three major ethnic groups (Ibos, Hausa and Yoruba) in Nigeria having a population density of over 800- 1500 per square kilometer[11]. After focused grouped discussions on the objective of the study, and with the consent of the participants, questionnaires were distributed to them and BP and anthropometric measurements were taken. Pregnant women and hypertensive patients and individuals with structural deformities were excluded from the measurement. The participants were broken into three major groups based on their educational levels. The first group called the Primary Education level consisted of candidates who had no form of formal education at all and also candidates who did not go beyond the first 6years of formal primary education. The second group called the secondary education level included candidates that did not go beyond the secondary or college education. The third group, tertiary education level, included candidates that have gone beyond the secondary education to tertiary education.
Blood Pressure Measurement (BP)
BP measurements were taken following standard protocol[12]. Participants were allowed to rest at least for 10minutes in a seated position with arms supported at the level of the heart. The BP was measured three times with the cuff completely evacuated and recovery allowed between readings. The average of the readings was used as the systolic (SBP) and diastolic blood pressures (DBP).
Anthropometry
Height (HT) was measured to the nearest 0.5cm using a vertical scale of portable stadiometer with the participant in erect position without shoes and head held in the frank fort plane. Weight was measured to the nearest 0.1kg with a bathroom scale with the participant lightly clothed. BMI was calculated as weight divided by square of height (kg/m2). Waist circumference (WC) was measured in centimeters at the narrowest waist. Hip circumference (HC) was measured at the largest posterior extension of the buttocks. WHR was calculated by dividing the WC with HC. Thigh circumference (TC) was measured at the midpoint of the thigh. Waist-height ratio (WHTR) was calculated by dividing WC with HT. Arm circumference (AC) and forearm circumference (FAC) were taken at the midpoints respectively. Skin fold thickness was measured on the subject's body at 3 sites (triceps, subscapular and calf) with a large caliper (Cambridge, MD). The triceps skin fold (TSF) was measured in midline of the posterior aspect of the arm over the triceps muscles, midway between the lateral projections of acromion process of the scapula and the inferior margin of the ulna olecranon process. The subscapular skin folds (SSF) was taken beneath the inferior angle of the scapula. Calf skin fold thickness was measured in the midline over the level of maximum protrusion. In each case a double thickness of skin and underlying tissue were raised and measured. A sum of the three skin folds (STS) was calculated. All measurements were taken on the right side.
Measurement Cut-off Points
Based on the WHO definition for cardiovascular disease risk[13], the following were accepted as cut-off points for obesity, BMI > 29.9 Kg/m2, WC>102cm for men and 88cm for women, WHR > 1.0 in men and 0.85 in women. WHtR > 0.05 was used as a cut-off point[14]. Following WHO standard for definition of elevated blood pressure[5]; the following were accepted as elevated BP; SBP > 140mmHg and/ or DBP > 90mmHg.
Statistical Analyses
Data were analyzed using SPSS 15.0. The population characteristics, anthropometric indicators, SBP and DBP for both rural and urban populations are shown as means and standard deviations. The frequencies and percentage frequencies of adiposity indication by the various indicators noted. Pearson correlation between the blood pressure indicators with adiposity indicators were carried out and also differences between the various adiposity indications between the two populations were also noted using the t-test.
Results
A total number of 567 individuals from the ages of 18 to 80 years were used for this study. 325 (57.3%) of the individuals were males while 254 (42.7%) were females. The mean age of the study group was 33.6 + 14 years, and 33.7 + 14 and 33.5 + 13 years, for males and females respectively. The mean ages of the males and females of the various groups and also the mean values of all the anthropometric measurements, blood pressure values, and obesity indicators have been summarized in Table 1.
Table 1.
Summary of the means and standard deviations of the various anthropometric and blood pressure parameters by sex across the educational levels
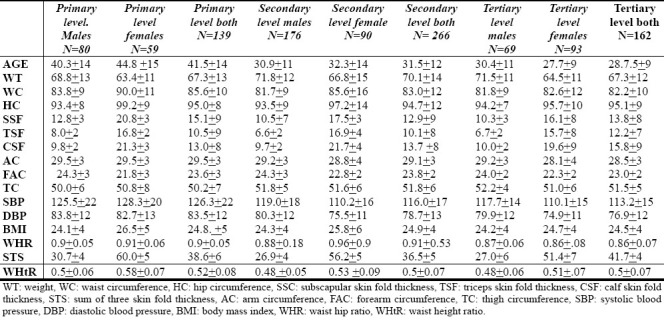
The largest mean value of subcutaneous fat for both males and females was noted in the primary education group, followed by the secondary education group. The BMI assessment has the smallest mean value for both males and females in the tertiary education group. In the measurements of the central obesity indicators, the largest mean WC was noted within the males and females of the primary education group while the least was noted in the tertiary education group. Both mean values of WHR and WHtR were noted to be smallest in the males and females of the tertiary education group. The mean blood pressure values were also largest for the primary education group and least for the tertiary education group.
For all the indicators of subcutaneous fat (SSF, TSF, CSF, and STS), general obesity (BMI), and central obesity (WC, WHR, WHtR) largest mean deposition of both subcutaneous, general and abdominal fats were noted amongst women of the primary education group. The males showed larger mean BP values than the females in all the groups.
In the summary of the obesity and cardiovascular disease risk occurrence, shown in Table 2, the primary education group was noted to be at most risk as against the tertiary education group.
Table 2.
Prevalence of obesity and cardiovascular disease risk by various indicators by sex across educational levels
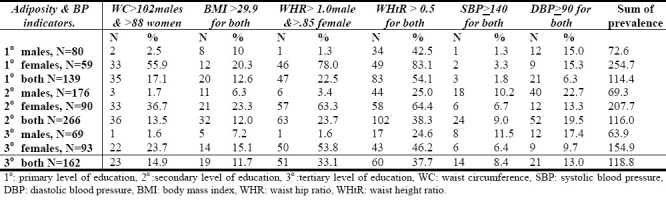
The prevalence of obesity and cardiovascular disease risk was found to be highest amongst females of the primary education group.
All the obesity and blood pressure indicators used in this study (WC,BMI, SBP, DBP, WHR, WHtR, STS) showed inverse correlations with educational levels, which are significant for WC, SBP, DBP, and WHtR. A higher and more consistent relationship was noted amongst the females. The highest and most consistent relationship was noted with blood pressure (SBP, DBP). The various degrees of correlation within the sexes has been summarized in Table 3.
Table 3.
Pearson correlation matrix of the various adiposity and BP indicators with educational level

Discussion
Obesity with hypertension is a common and important problem in primary health care[16]. It is an important risk factor for major chronic diseases, such as diabetes, heart disease, stroke and certain cancers[17] and its link with education and socio-economic status in the various communities and ethnicities has been the query of most researches.
This work has looked at the relationship between adiposity and blood pressure with education. Education has been shown to be a major determinant of health status, particularly in poor countries[18]. Varying results have been reported on the effect of education on obesity and blood pressure from the different researches on various ethnicities and countries[19,20].
The work noted an inverse relationship between education and obesity and blood pressure. Higher mean values of the measured anthropometric dimensions and ratios were observed in the individuals that had little or no education than in those that had better education. This same group also was more vulnerable to obesity and all the related cardiovascular disease risks. Both general, subcutaneous and abdominal obesities were worse for all the females of the various education group and worst for the females of the least educated group.
This work has noted a strong education gradient in obesity for the studied population with the education gradient in obesity being stronger in women than in men. Similar findings have being reported for other countries and ethnicities[18,20,21]. Increasing education at any point along that spectrum would be expected to reduce obesity to a similar degree. Cutler and Lleras-Muney[18] found that those with more years of schooling are less likely to smoke, drink a lot, to be overweight or obese or to use illegal drugs. Grossman and Kaestner[22] in their work “Effects of Education on Health” concluded that years of formal schooling is the most important correlate of good health.
Various explanations have been proffered on the reasons for this strong relationship between education and obesity. Educated individuals have been reported to make better use of health related information than those who are less educated[23]. The lack of education about energy contents of foods has also been suggested to be a contributor to the effects of social class on obesity[24]. Cutler and Lleras-Muney[18] found that those with more years of schooling are less likely to smoke, drink a lot, to be overweight or obese or to use illegal drugs. They are also more likely to exercise and to obtain preventive cares. Yoon25 suggested that it is possible that more highly educated people have the knowledge to develop healthy lifestyles and have more awareness of the health risks associated with being obese. The positive effect of education on obesity can summarily be attributed to greater access to health-related information and improved ability to handle such information by the educated, clearer perception of the risks associated with lifestyle choices and improved self-control and consistency of preferences over time.
The establishment of a strong relationship between obesity and blood pressure within any community, group or country is important in the development of the most suitable education-based policies to counteract the present increase in obesity and related chronic diseases both in developed and developing communities and countries. The standard of living and health in the community can be improved by education. This relationship between education and health has been traced to the health information which is part of education. So health education programs aimed at promoting healthy lifestyles might in principle generate similar effects to those associated with school education by providing relevant health information. To this effect government and other relevant policy making bodies are called upon to intensify actions toward organizing and funding of public health education campaigns.
Conclusion
Education, whether through formal schooling or health promotion campaigns, has been identified as one of the factors that can be used to combat the present increase in the prevalence of elevated blood pressure, obesity and obesity related diseases. We therefore call for the right policies and prompt actions in this direction.
References
- 1.Doll S, Paccaud F, Bovet P, Burnier M, Wietlisbach V. Body mass index, abdominal adiposity and blood pressure: consistency of their association across developing and developed countries. Int J Obes. 2002;26:48–57. doi: 10.1038/sj.ijo.0801854. [DOI] [PubMed] [Google Scholar]
- 2.World Health Organization. Diet, Nutrition and the Prevention of Excess Weight Gain and Obesity, Report of a joint WHO/FAO expert consultation, Geneva. 2003. [Accessed November 15, 2009]. at http://whqlibdoc.who.int/trs/who_trs_916.pdf .
- 3.Ramadan J, Barac-Nieto M. Reported frequency of physical activity, fitness, and fatness in Kuwait. Am J Hum Bio. 2003;15(4):514–521. doi: 10.1002/ajhb.10190. [DOI] [PubMed] [Google Scholar]
- 4.James WP, Ralph A. New understanding in obesity research. Proc Nutr Soc. 1999;58:385–393. doi: 10.1017/s0029665199000506. [DOI] [PubMed] [Google Scholar]
- 5.Sobal J, Rauschenbauch BS, Frogillo EA., Jr Marital status, fatness and obesity. Soc Sci Med. 1992;35(7):915–923. doi: 10.1016/0277-9536(92)90106-z. [DOI] [PubMed] [Google Scholar]
- 6.Rogueka E, Bielicki T. Social contrasts in the incidence of obesity among adult large city dwellers in Poland in 1986 and 1996. J Bio Soc Sci. 1999;31:419–423. doi: 10.1017/s0021932099004198. [DOI] [PubMed] [Google Scholar]
- 7.Lipowicz A. Effect of husbands’ education on fatness of wives. Am J Hum Biol. 2003;15:1–7. doi: 10.1002/ajhb.10119. [DOI] [PubMed] [Google Scholar]
- 8.Sobal J, Stunkard AJ. Socioeconomic status and obesity: a review of the literature. Psycho Bull. 1989;105:260–275. doi: 10.1037/0033-2909.105.2.260. [DOI] [PubMed] [Google Scholar]
- 9.Flegal KM, Carroll MD, Kuczmarski RJ, Johnson CL. Overweight and obesity in the United States. Int J Obes Relat Metab Disord. 1998;22:39–47. doi: 10.1038/sj.ijo.0800541. [DOI] [PubMed] [Google Scholar]
- 10.Cooper R, Rotimi C, Ataman S, et al. The prevalence of hypertension in seven populations of West African origin. Am J Publ Health. 1997;87:160–168. doi: 10.2105/ajph.87.2.160. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Onwuka O. Nigeria peoples and cultures. Historical Socio-cultural Perspective. Echrisi and Company. 2002 [Google Scholar]
- 12.Beevers G, Lip GYH, O’Brien E. ABC of hypertension: Blood Pressure Measurement Part II: Conventional Sphygomonometry: Technique of auscutatory blood pressure measurement.Clinical Review. Br Med J. 2001;322:1110–1114. doi: 10.1136/bmj.322.7293.1043. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.World Health Organization consultation on obesity: Preventing and managing the global epidemic. Geneva, Switzerland: Division of Non Communicable Diseases, Programme of Nutrition, Family and Reproductive Health, World Health Organization. 1998. [Accessed November 15, 2009]. at http://who.int/cardiovascular_diseases/resources /index.html .
- 14.Hsieh SD, Muto T. A simple and practical index for assessing the risk of metabolic syndrome during routine health checkups. Nippon Rinsho. 2004;62:1143–1149. [PubMed] [Google Scholar]
- 15.The guidelines subcommittee of the WHO-ISH Mild Hypertension Liaison committee. 1999 World Health Organization-International Society of Hypertension guidelines for the management of hypertension. J Hypert. 1999;17:151–183. [PubMed] [Google Scholar]
- 16.Engberg M, Christensen B, Karlsmose B, Lous J, Lauritzen T. General health screens to improve cardiovascular risk profiles: A randomized controlled trial in general practice with 5-year follow up. J Fam Pract. 2002;51:546–552. [PubMed] [Google Scholar]
- 17.Stevens J, Couper D, Pankow J. Sensitivity and specificity of anthropometrics for the prediction of diabetes in a biracial cohort. Obes Res. 2001;9:696–705. doi: 10.1038/oby.2001.94. [DOI] [PubMed] [Google Scholar]
- 18.Cutler D, Lleras-Muney A. “Education and Health: Evaluating Theories and Evidence”, NBER Working Paper 12352. 2006. [Accessed November 15, 2009]. at www.ideas.repec.org/p/nbr/nberwo/12352.htm .
- 19.Ordunez P, Munoz JLB, Espinosa-Brito A, Silva LC, Cooper RS. Ethnicity, Education, and Blood Pressure in Cuba. Am J Epidemiol. 2005;162:49–56. doi: 10.1093/aje/kwi163. [DOI] [PubMed] [Google Scholar]
- 20.Webbink D, Martin NG, Visscher PM. Does Education Reduce the Probability of Being Overweight? CPB Discussion Papers 102, CPB Netherlands Bureau for Economic Policy Analysis. 2008. [Accessed November 15, 2009]. at http://www.genepi.qimr.edu.au/contents/p/…/Webbink_JnrlHealthEcon_Feb2010.pdf .
- 21.Sanchez-Vaznaugh EV, Kawachi I, Subramanian SV, Sanchez BN, Acevedo-Garcia D. Do Socioeconomic Gradients in Body Mass Index Vary by Race/Ethnicity, Gender and Birthplace? Am J Epidemiol. 2006;169(9):1102–1112. doi: 10.1093/aje/kwp027. [DOI] [PubMed] [Google Scholar]
- 22.Grossman WM, Kaestner R. Effects of Education on Health. In: Behrman J.R., Stacey N., editors. The Social Benefits of Education. Ann Arbor, MI: University of Michigan Press; 1997. [Accessed November 15, 2009]. at www.nber.org/paper/w7078.refxt . [Google Scholar]
- 23.Kemna H. Working Conditions and the Relationship between Schooling and Health. J Health Econ. 1987;6:189–210. doi: 10.1016/0167-6296(87)90008-7. [DOI] [PubMed] [Google Scholar]
- 24.Speakman JR. Associations between BMI, Social Strata and the Estimated Energy Content of Foods. Intl J Obes. 2005;29(10):1281–1288. doi: 10.1038/sj.ijo.0803018. [DOI] [PubMed] [Google Scholar]
- 25.Yoon YS, Oh SW Park HS. Socio-Economic Status in Relation to Obesity and Abdominal Obesity in Korean Adults: A Focus on Sex Differences, Obesity (Silver Spring) 2006;14:909–919. doi: 10.1038/oby.2006.105. [DOI] [PubMed] [Google Scholar]