

Abstract
Aims and Objectives:
To compare the marginal sealing ability of ormocer with a hybrid composite using an ormocer based bonding agent and a conventional fifth generation bonding agent.
Materials and Methods:
Fifty four human premolars were randomly distributed into four test groups of 12 teeth each and two control groups of 3 teeth each. Class I occlusal preparation of 1.5 mm depth were made in each tooth. These were restored using the adhesive and restorative material according to the group. The restorations were finished using a standard composite finishing and polishing kit. Thermocycling between 5° C and 55°C was carried out. Having blocked the root apex and the entire tooth surface except 1 mm around the restoration margin, the teeth were immersed in 2% methylene blue for 48 hours, after which the dye penetration through the margins of each sample was studied under a stereomicroscope.
Results and Discussion:
Group IV (Admira with Admira Bond) showed the minimum marginal leakage with a mean of 0.200 mm. Four samples in this group showed no microleakage at all and a maximum of 0.400 mm was seen in one sample. Group II (Spectrum TPH with Admira Bond) showed the maximum leakage with a mean of 0.433 mm. One sample showed as much as 1.00 mm of microleakage. Admira when used with Admira Bond showed lesser microleakage than Spectrum TPH used with Prime & Bond NT, the difference being statistically insignificant.
Keywords: Composite, dye penetration, marginal sealing, microleakage, ormocer
Introduction
An increasingly confusing array of promising new materials has now become available. To evaluate the factual clinical worth of a highly branded restorative material without being carried away by its proposed qualities is a challenge that we as clinicians must accept.
The principles of adhesive dentistry date back to 1955 when Buonocore,[1] employing techniques of industrial bonding, suggested that acids could be used as a surface treatment before applying resins. Along with adhesion, the most important phase has been the evolution of dental restorative composites. These have come a long way from being traditionally macrofilled (8-mm filler), to microfilled (0.01 to 0.04-mm filler), to hybrid (0.4 to 1-mm filler), and now to nanofilled (0.005 to 0.01-μm filler). But if we notice, all the changes have been made to the fillers. Although the resin matrix significantly influences the properties of composites, it is interesting to note that there have been few fundamental changes in that aspect of the restorative-adhesive system since the introduction of dimethacrylates in the form of bisphenol –A-diglycidyl dimethacrylate (Bis-GMA), urethane dimethacrylate, and triethylene glycol dimethacrylate. One of the greatest deficiencies associated with these resins is the high degree of polymerization shrinkage and high content of residual monomers in the cured composite material.
Ormocers
In an attempt to overcome some of the limitations and concerns associated with the traditional composites, a new packable restorative material was introduced called Ormocer,[2] which is an acronym for organically modified ceramic technology. Ormocer materials contain inorganic-organic co-polymers in addition to the inorganic silanated filler particles. It is synthesized through a solution and gelation process[3] (sol-gel process) from multifunctional urethane and thioether(meth)acrylate alkoxysilanes. Ormocers are described as three dimensionally cross-linked copolymers. The ormocer matrix is a polymer even prior to light curing. It consists of ceramic polysiloxane, which has low shrinkage as against the organic dimethacrylate monomer matrix seen in composites. To the polysiloxane chains in ormocer, polymerisable side chains are added to react during curing and form the setting matrix. These inorganic molecules are longer than Bis-GMA, which could explain the material's lower volumetric shrinkage. Incorporation of filler particles decreases volumetric shrinkage from 2–8% when it has no fillers to 1–3% when fillers are incorporated. The filler particles are 1–1.5 μm in size.[4,5] This material presents 77–78 wt% of filler loading, 61% filler volume, and a modulus of elasticity of 10.700MPA (manufacturer's information) The abundance of polymerization opportunities in these materials allows ormocers to cure without leaving residual monomers, thus having greater biocompatibility with the tissues. Ormocers have a capacity to double the conversion of monomers, improving the physical properties of the material. Ormocers were formulated in an attempt to overcome the problems created by the polymerization shrinkage of conventional composites and also because ormocers include low shrinkage, high abrasion resistance, biocompatibility, and protection against caries.[6] Their backbone is an inorganic network formed by polycondensation. This backbone is based on silicon dioxide and functionalized with polymerisable organic units to produce so called three-dimensional compound polymers. The silicon dioxide backbone of ormocers provides them with their name and accounts for their relationship with ceramics. They combine glass-like (inorganic) constituents with polymer (organic) constituents.
Review of Literature
Dental journals now abound in studies on various clinical features of ormocer.
Mahmoud SH et al.[7] evaluated and compared the 2-year clinical performance of an ormocer, a nanohybrid, and a nanofill resin composite with that of a microhybrid composite in restorations of small occlusal cavities made in posterior teeth. After 2 years, all three materials showed acceptable clinical performance similar to that of the microhybrid resin composite.
Gorucu J et al. compared the MOD restorations of posterior teeth restored with hybrid composite, packable composite, and ormocer, and concluded that the cuspal fracture resistance obtained by all three was similar to intact, unprepared teeth.
Civelek A et al.[8] studied the polymerization shrinkage and microleakage in class II cavities of various resin composites and found that ormocer showed lesser microleakage than the ion-releasing and hybrid composites lined only with bonding agent at the cemento–enamel junction.
N.M. Ayad et al.[9] The authors conducted an in vitro study to determine the effects of two bleaching systems on an ormocer and a conventional hybrid resin composite. Ormocer achieved a light color change on bleaching, and showed greater resistance to adverse microleakage and hardness effects.
Ajlouni R et al.[10] remarked that ormocers “were more biocompatible and had lower wear rate.”. They compared the shear bond strength of ormocer and a traditional Bis GMA matrix containing composite and found no significant differences in the same for both.
Hennig AC et al.[11] followed up and studied ormocer restorations placed on 70 carious and caries-free lesions (Class V) in 26 patients at baseline and 6 and 12 months, using modified LUTZ (1977) and RYGE (1980) criteria. They found the overall clinical behavior of the ormocer material to be acceptable up to 1 year.
Juergen G et al. carried out an in vivo study to compare the microleakage values of an ormocer and a commonly used composite and found no statistically significant differences for the same between the two.
Ruya Y et al. also carried out an in vitro study to compare the marginal sealing ability in Class V cavities of ormocer with three different resin composites and found no statistically significant differences between them.
Siso et al.[12] studied the diametral strength, depth of cure, flexural strength and compressive strength of ormocer, a hybrid composite and a packable composite, and concluded that the ormocer showed greater depth of cure and flexural strength as compared to the other two. Its flexural strength was between the packable composite and the hybrid composite while its compressive strength was lesser than the composite materials.
Materials and Methods
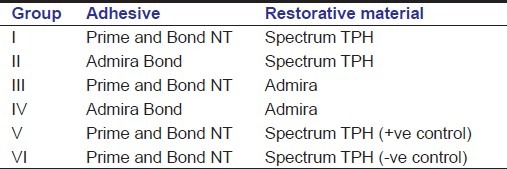
Fifty-four human premolars, free of any visible cracks and caries, freshly extracted for orthodontic reasons, were collected. All calculus and periodontal remnants were carefully removed with a scalpel blade. The teeth were distributed into six groups [Table 1].
Table 1.
Group distribution
Restoration
The teeth were divided randomly into four test groups of 12 teeth each and two control groups of three teeth each. Class I occlusal preparation of 1.5-mm depth was made in each tooth. These were restored using the adhesive and restorative material according to the group. The restorations were finished using a standard composite finishing and polishing kit (Shofu Incorporated, Japan).
Thermocycling
The samples were then kept in water at room temperature for one day. The teeth were subjected to thermocycling between 5°C (+/-2) and 55°C (+/-2) keeping them in a water bath at 5°C for 25 s, then in 37°C for 5 s, followed by 55°C for 25 s and again at 37°C for 5 s. The samples were subjected to 100 such cycles. After thermocycling, they were again kept in distilled water at room temperature for 24 h.
Dye insertion
The apical tip of each sample was covered with modeling wax to prevent dye penetration through the foramen. The teeth were then coated with two layers of nail paint, leaving a margin of approximately 1 mm all around the restoration margins, thus allowing dye penetration to occur only through the restoration margins. After the varnish had dried, the samples were immersed in a 2% solution of methylene blue for 48 h. After 2 days, the samples were washed under running water for 30 min to remove the dye completely.
Sectioning
Each sample was then sectioned buccolingually through the center of the restoration using a carborundum disc on a mandrel mounted on a slow speed hand piece.
Dye penetration measurement
Each sample was studied under a stereomicroscope. The linear dye penetration was studied with the help of the scale attached to the microscope. The linear dye penetration along the margin was noted for each sample.
Results
The linear dye penetration in tenths of 1 mm for each group [Tables 2–4] was recorded [Figures 1–6].
Table 2.
Dye penetration for group I and group II
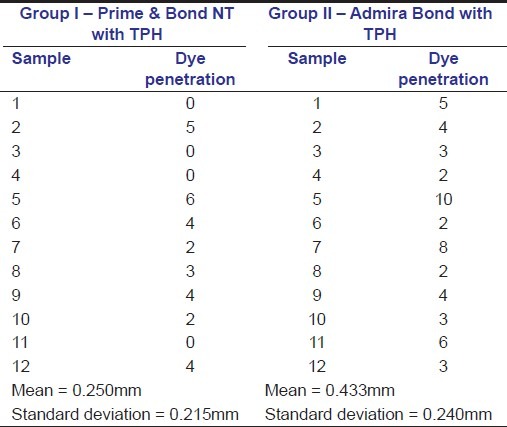
Table 4.
Dye penetration for control groups

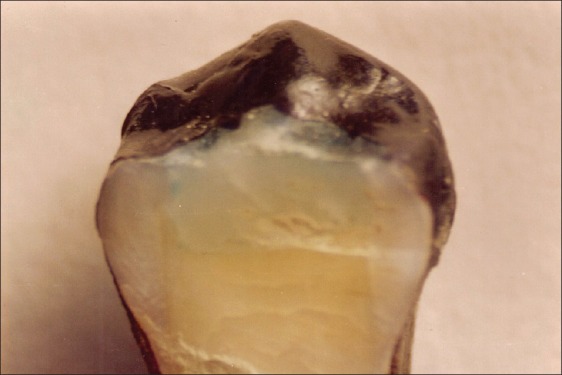
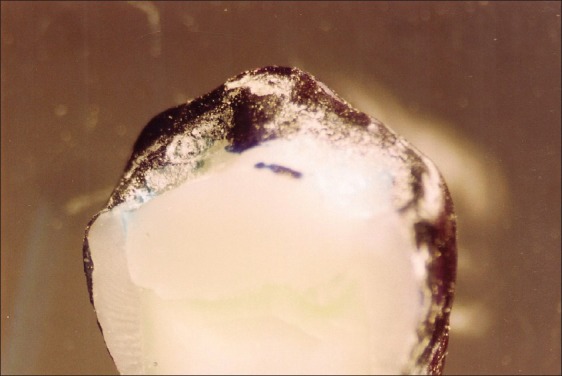
Figure 1.

Ormocer: An aesthetic direct restorative material. Linear dye penetration in Group I – Spectrum TPH with Prime and Bond NT, Mean – 0.250 mm
Figure 6.

Ormocer: An aesthetic direct restorative material, Linear dye penetration in Group VI – negative control, Mean – 0.000 mm
Table 3.
Dye penetration for Group III and Group IV
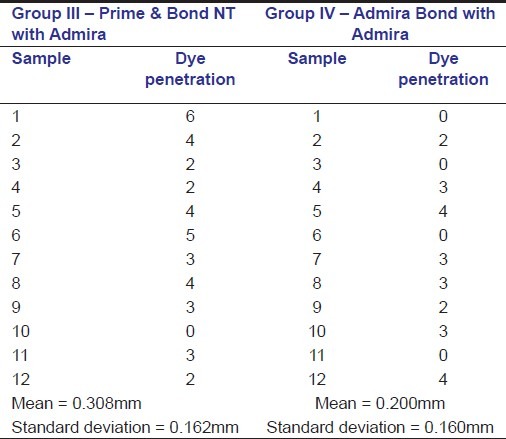
Figure 2.
Ormocer: An aesthetic direct restorative material. Linear dye penetration in Group II – Spectrum TPH with Admira Bond, Mean – 0.433 mm
Figure 3.
Ormocer: An aesthetic direct restorative material. Linear dye penetration in Group III – Admira with Prime and Bond NT, Mean – 0.308 mm
Figure 4.

Ormocer: An aesthetic direct restorative material. Linear dye penetration in Group IV – Admira with Admira Bond, Mean – 0.200 mm
Figure 5.

Ormocer: An aesthetic direct restorative material. Linear dye penetration in Group V – positive control, Mean – 1.500 mm
Based on the readings obtained, a statistical analysis was carried out to estimate the significance of the level of difference between the various groups [Tables 5–6]. Since the sample size of each group was less than 30, an unpaired ‘t’ test was applied, having calculated the standard deviations for each group using the standard formulae.
Table 5.
Standard deviation, t and P values
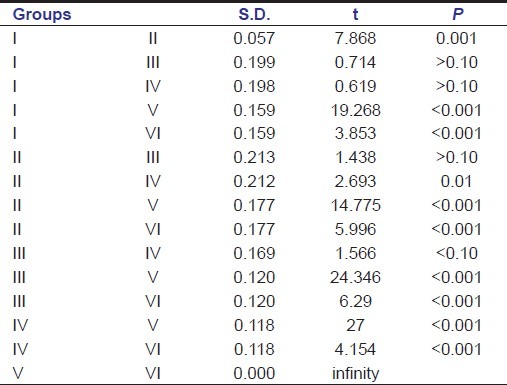
Table 6.
Mean dye penetration values
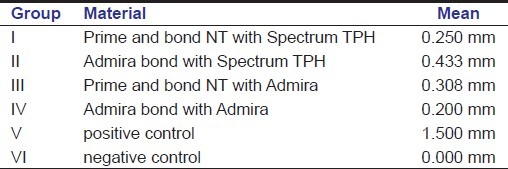
Group IV (Admira with Admira Bond, Voco, Cuxhaven, Germany) showed the minimum marginal leakage with a mean of 0.200 mm. Four samples in this group showed no microleakage at all and a maximum of 0.400 mm was seen in one sample.
Group II (Spectrum TPH [Dentsply Caulk, Milford, USA] with Admira Bond) showed the maximum leakage with a mean of 0.433 mm. One sample showed as much as 1.00 mm of microleakage.
Admira when used with Admira Bond showed lesser microleakage than Spectrum TPH used with Prime and Bond NT (Dentsply Caulk, Milford, USA), the difference being statistically insignificant.
Discussion on reduced microleakage in ormocers
Polymerization contraction, inherent to some materials such as composite resins, leads to the development of significant forces, resulting in marginal gap formation.[13] The quest for the perfect composite as an aesthetic posterior restorative material has brought about numerous modifications in its composition, ranging from the inclusion of beta quartz to glass inserts. Although, plenty of improvements have resulted, a lot more needs to be achieved. So far, all the changes have been made to the filler content of the material.
The gap formation around a resin based restoration may be caused by:
Poor placement technique
Polymerization contraction
Mismatch of coefficient of thermal expansion between the restorative material and the tooth
Role of bonding agents.
The placement technique in this study was incremental, which was used for both the materials.
The ormocer matrix is a polymer even prior to light curing. They are hybrid polymer materials synthesized by the sol-gel process. This process starts by building up an inorganic network through controlled hydrolysis and condensation of organically modified Si alkoxides. Co-condensation with other metal alkoxides (Ti, Zr, Al alkoxides) is also possible. In a subsequent step, the polymerisable groups, which are fixed to the inorganic network, react with each other in a thermal or ultraviolet-initiated process. In this two-stage process, an inorganic–organic copolymer is synthesized. In addition, it is possible to use organically modified Si alkoxides, which do not enter into any organic polymerization reaction and thereby contribute to an organic functionalization of the inorganic network.
It consists of ceramic polysiloxane, which has low shrinkage as against the organic dimethacrylate monomer matrix seen in composites (the resin matrix of Spectrum TPH consists of a BIS-GMA adduct, ethoxylated bisphenol – A- dimethacrylate, BIS – EMA, and triethylene glycol dimethacrylate). To the polysiloxane chains in ormocer, polymerisable side chains are added to react during curing and forming the setting matrix. These inorganic molecules are longer than Bis-GMA, which could explain the material's lower volumetric shrinkage. Incorporation of filler particles decreases volumetric shrinkage from 2–8% when it has no fillers to 1–3% when fillers are incorporated. The filler particles are 1–1.5 μm in size. This material presents 77–78 wt% of filler loading, 61% filler volume, and a modulus of elasticity of 10.700MPA (manufacturer's information). Because of this reduction in the number of monomers and the presence of polysiloxane, the polymerization shrinkage should be lesser in ormocer than in composite.
The temperature fluctuation is of consequence because the coefficient of thermal expansion of hybrid composites (35 ×10-6 ppm/0C)) is approximately three times that of the tooth (dentin=11 ×10-6 ppm/0C; enamel=17 ×10-6 ppm/0C), while that of ormocer is claimed to be between the two. So ormocer is expected to expand and contract much more like natural tooth structure than composite, thus significantly reducing the marginal gap formation.
The positive role of bonding agents in reducing microleakage has been proved.
Admira Bond is also a dentin–enamel bond whose key components are specially developed ormocers, which complex three dimensionally curing inorganic co-polymers. It has calcium complexing functionality, which is supposed to enhance the bond strength on tooth structure. Due to its chemical affinity, Admira Bond is supposed to bond firmly to both, the tooth and the filling material. According to a study carried out by Frankenberger, comparing the bond strength on dentin, using conical ejection test for six filling materials, Admira with Admira Bond showed the highest bond strength and it is a proven fact that a successful bonding agent must be able to resist the polymerization contraction shrinkage and subsequent microgap formation at the dentinal surface as the resin material is cured.
This study concluded that restorations done with Admira and Admira Bond gave better marginal seal than restorations done with TPH and Prime and Bond NT.
Conclusion
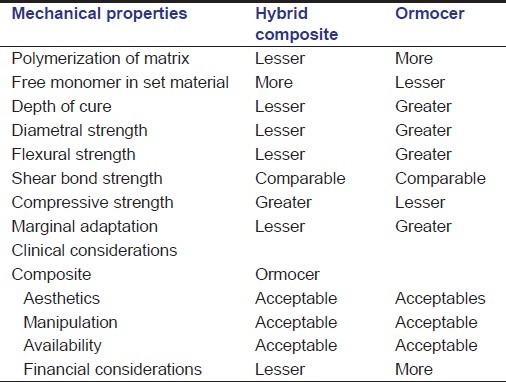
In restorative dentistry, choosing the correct restorative material is one of the primary variables that determine its success. Particularly in recent years, a lot of research has been done on adhesive dentistry. This has resulted in a number of positive developments and has provided dentists with assistance in selecting the correct materials and methods. In order to lessen a material's negative effects, we must know its physical, biological and clinical properties well [Table 7].
Table 7.
Comparative properties of composite versus ormocer
This study was carried out to compare the marginal sealing ability of an ormocer-based material (Admira) and a hybrid composite (Spectrum TPH) when used with an ormocer-based bonding agent (Admira Bond) and a conventional fifth-generation bonding agent (Prime and Bond NT). We found that Admira used with Admira Bond exhibited lesser microleakage than Spectrum TPH used with Prime and Bond NT, the difference being statistically insignificant.
So taking into consideration the present study and having reviewed the available comparative studies on the properties of ormocer-based restorative materials, they seem to be an acceptable choice for direct aesthetic restorations or should we say ormocers have arrived?
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
References
- 1.Bowen RL. Adhesive Bonding of various materials to hard tissues ad bonding to dentin improved by pretreatment and the use of surface active agents. J Dent Res. 1965;44:903–21. doi: 10.1177/00220345650440052501. [DOI] [PubMed] [Google Scholar]
- 2.Cunha LG, Alonso RC, Santos PH, Sinhoreti MA. Comparative study of the surface roughness of ormocer-based and conventional composites. J Appl Oral Sci. 2003;11:1–11. doi: 10.1590/s1678-77572003000400014. [DOI] [PubMed] [Google Scholar]
- 3. info@isc.fhg.de> – Fraunhofer Institute for Silicate Research, ISC.
- 4.Manhart J, Kunzelmann KH, Chen HY, Hickel R. Mechanical properties and wear behavior of light-cured packable composite resins. Dent Mater. 2000;16:33–40. doi: 10.1016/s0109-5641(99)00082-2. [DOI] [PubMed] [Google Scholar]
- 5.Kielbassa AM, Müller U, García-Godoy F. In situ study on the caries-preventive effects of fluoride releasing materials. Am J Dent. 1999;12:S13–4. [PubMed] [Google Scholar]
- 6.Hickel R, Dasch W, Janda R, Tyas M, Anusavice K. New direct restorative materials. Int Dent J. 1998;48:3–15. doi: 10.1111/j.1875-595x.1998.tb00688.x. [DOI] [PubMed] [Google Scholar]
- 7.Mahmoud SH, El-Embaby AE, AbdAllah AM, Hamama HH. Two-year clinical evaluation of ormocer, nanohybrid and nanofill composite restorative systems in posterior teeth. J Adhes Dent. 2008;4:315–22. [PubMed] [Google Scholar]
- 8.Civelek A, Ersoy M, L’Hotelier E, Soyman M, Say EC. Polymerization shrinkage and microleakage in Class II cavities of various resin composites. Oper Dent. 2003;28:635–41. [PubMed] [Google Scholar]
- 9.Ayad NM, Bedewi A, Hanafy S, Saka S. Effect of bleaching on microleakage, surface hardness, surface roughness, and color change of an ormocer and a conventional hybrid resin composite. Internet J Dent Sci. 2009;6:2. [Google Scholar]
- 10.Ajlouni R, Bishara SE, Soliman MM, Oonsombat C, Laffoon JF, Warren J. The use of Ormocer as an alternative material for bonding orthodontic brackets. Angle Orthod. 2005;75:106–8. doi: 10.1043/0003-3219(2005)075<0106:TUOOAA>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 11.Hennig AC, Helbig EB, Haufe E, Richter G, Klimm HW. Restoration of Class V cavities with the Ormocerbased filling system Admira. Schweiz Monatsschr Zahnmed. 2004;114:104–14. [PubMed] [Google Scholar]
- 12.Siso SH, Hürmüzlü F. Physical properties of three different types of LC composite resins. Acta Stomatol Croat. 2008;42:147–54. [Google Scholar]
- 13.Bausch JR, de Lange K, Davidson CL, Peters A, de Gee AJ. Clinical significance of polymerization shrinkage of composites resins. J Prosth Dent. 1982;48:59–62. doi: 10.1016/0022-3913(82)90048-8. [DOI] [PubMed] [Google Scholar]