

Abstract
Objective:
To evaluate and compare the retention, marginal discoloration, surface texture and anatomical form of pit and fissure sealants.
Materials and Methods:
Thirty children between the ages of 6 and 10 years, who were attending the school health program regularly, had participated in the study. A split-mouth design was used in which the two fissure sealants (Helioseal-F and Glass ionomer Fuji VII) were randomly placed in 60 matched contralateral pairs of permanent molar teeth. Sealants were rated by a single trained and calibrated examiner using mouth mirrors and probes following the US Public Health Service criteria. The sealants were evaluated at 3 months, 6 months and 1 year intervals.
Results:
The data obtained for retention, marginal discoloration, surface texture and anatomical form of pit and fissure sealants were tabulated and compared statistically using the Chi-square test of significance.
Conclusion:
The Helioseal-F sealant was better than the Glass ionomer Fuji VII sealant with respect to retention, anatomical form and surface texture. Both the materials showed similar results with respect to marginal discoloration.
Keywords: Anatomical form, fissure sealant, marginal adaptation, retention, surface texture
Introduction
Dental caries is a preventable disease of the mineralised tissues of the teeth with a multifactorial etiology related to the interactions over time between tooth substance and certain microorganisms and dietary carbohydrates producing plaque acids. Over the last few decades, several advancements have been made in caries prevention. Fluorides have been found to be extremely effective in preventing caries on the smooth surfaces of the teeth, but are less effective on the occlusal surfaces. Sealants protect the occlusal surfaces inhibiting bacterial growth and providing a smooth surface, increasing the probability that the surface will stay clean.
The complex morphology of the occlusal pits and fissures warrants an ideal site for the retention of bacteria and food remnants, rendering proper oral hygiene maintenance difficult. Another factor that is responsible for the high incidence of occlusal caries is the lack of salivary access into the fissures due to surface tension, preventing remineralization and thus lessening fluoride effectiveness at this spot as compared with the smooth surfaces. A precise diagnostic method of detection in case of occlusal incipient caries is still not available. The technique of pit and fissure sealants plays, undoubtedly, a fundamental role in preventing occlusal caries, both in primary and in permanent teeth.[1,2]
Glass ionomer sealants present a chemical bond to the dental tissue and have an anticariogenic effect by fluoride release. However, the deficiencies of Glass ionomer cements are lack of toughness, early water sensitivity, low abrasion resistance and different retention rates.[3] Glass ionomer sealants have poorer retention than composite resin materials, and their effect on caries reduction is equivocal. Therefore, Glass ionomer sealants are mainly used when it is not possible to use a resin material, for example due to poor patient compliance.[4]
Resin-based sealants are effective in caries control due to a physical barrier formation, which prevents the metabolic exchange between the fissure microorganisms and the oral environment. A fluoride-releasing pit and fissure resin sealant (Helioseal-F) is an effort to combine both the caries preventive effect via fluoride release and a good micromechanical bond with the tooth.[5]
Hence, a study was conducted to evaluate and compare the retention, anatomical form, marginal discoloration and surface texture of two pit and fissure sealants.
Study population and methods
Thirty children between the ages of 6 and 10 years, who were attending the school health program regularly, had participated in the study. Approval from the ethical committee and the parents was obtained prior to the onset of the study. A split-mouth design was used in which the two fissure sealants (Helioseal-F, Ivoclar Vivadent Somerset,NJ and GC Fuji VII,GC Corporation) were randomly placed in 60 matched contralateral pairs of permanent molar teeth. Fissurotomy was performed prior to the placement of the sealants.
Selection criteria
Age of the patient was between 6 and 10 years.
Presence of all four caries-free permanent first molars.
Evidence of an acceptable home dental cleaning regimen.
Patient cooperation and acceptance for the treatment.
Absence of class I clinical carious lesion.
No prior dental therapy.
Possibility to get proper isolation with cotton rolls.
No fluoride mouth rinse program practiced in the school.
No central fluoride water supply in the school/community where the students live.
Exclusion criteria
History of any medical disease that might interfere with the study.
Long-term regimen of medication that could affect the salivary flow and diet modification.
Current participation in other studies.
History of any adverse reaction to any of the restorative materials used.
History of abnormal parafunctional activity.
Heavy occlusal contacts on the teeth to be restored.
Patients undergoing fluoride application regimen.
Highly uncooperative child.
Helioseal-F sealant
A standard fissurotomy bur (SSW FG-330) was used to widen the occlusal pits and fissures of the permanent first molars. The enamel was conditioned by etching with 35–37% phosphoric acid and then washed and dried carefully to obtain a chalky-white enamel surface. Manufacturer's instructions were consulted for recommended etch and rinse times. A minimum amount of sealant that was required to adequately cover the pit and fissure network was applied. Any air bubbles or voids were removed before curing. The entire procedure was performed under cotton roll isolation. The restoration was checked for high points using articulating paper.
Fuji VII Glass Ionomer Sealant
A standard fissurotomy bur (SSW FG-330) was used to widen the occlusal pits and fissures of the permanent first molars. Fuji VII was mixed according to the manufacturer's instructions and placed into the prepared tooth and left untouched for 4 min after applying a protective coat of Fuji varnish with the help of a microbrush to provide protection against moisture. The entire procedure was performed under cotton roll isolation. The restoration was checked for high points using articulating paper.
Clinical evaluation
Sealants were rated by a single trained and calibrated examiner using the mouth mirrors and probes following the US public health service criteria.[6] The reason for opting for this criterion was due to its simplicity, easy to record the data in a presentable form and easy communication. It covers most of the parameters that account for a restorations clinical success. Evaluation parameters included retention, anatomical form, surface texture and marginal discoloration. Scoring was done either by denoting alphabets (like A, B, C… etc.) or numerical values (0, 1, 2…etc.). Because numerical value was easier for statistical analysis, we have adopted the same in our study. For criteria like anatomical form and marginal discoloration, we have given a score of 0 to indicate acceptability and scores of 1 and 2 to indicate progressively lessening degrees of clinical acceptance. For criteria like surface texture, we have given a score of 0 to indicate acceptability and scores of 1 to indicate progressively lessening degrees of clinical acceptance.
The retention was evaluated by visual inspection with the help of a probe and mouth mirror by a single operator as advocated by Horowtiz, Heifetz and Poulsen.[7] A score of 0 was given for complete retention, 1 was given for partial retention and 2 was given for no retention.
Results
The data was obtained at 3 months, 6 months and 1 year intervals. The results were tabulated for retention, marginal discoloration, surface texture and anatomical form of pit and fissure sealants and statistically compared using the Chi-square test of significance [Tables 1–4] [Figures 1–4].
Table 1.
Comparison of retention between Helioseal-F and Glass ionomer Fuji VII
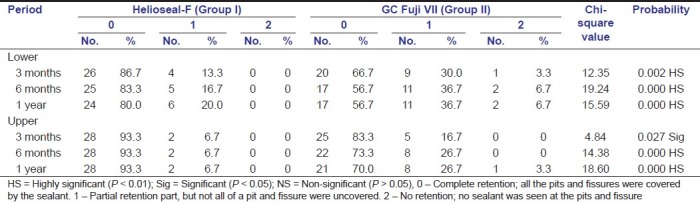
Table 4.
Comparison of surface texture between Helioseal-F and Glass ionomer Fuji VII
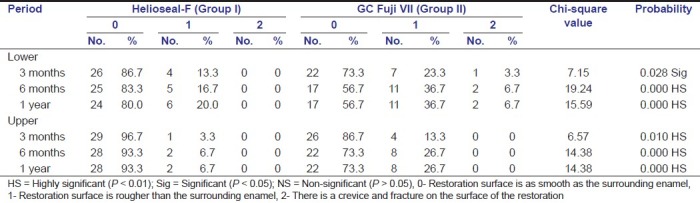
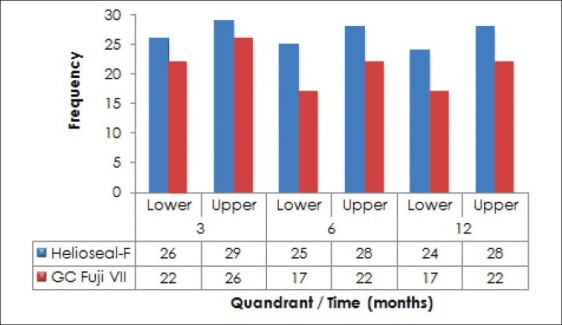
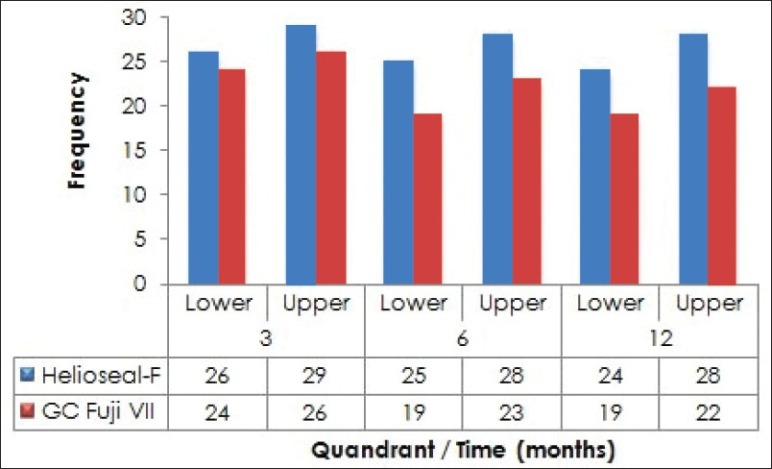
Figure 1.

Distribution of cases of Helioseal-F and Fuji VII with respect to their retention rates
Figure 4.
Distribution of cases of Helioseal-F and Fuji VII with smooth surface texture
Table 2.
Comparison of marginal discoloration between Helioseal-F and Glass ionomer Fuji VII
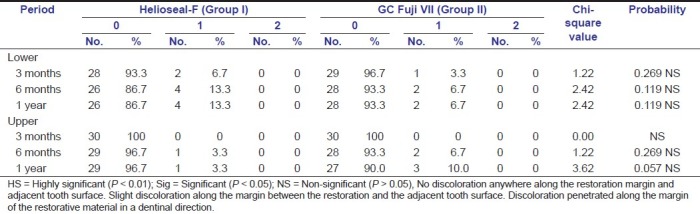
Table 3.
Comparison of anatomical form between Helioseal-F and Glass ionomer Fuji VII
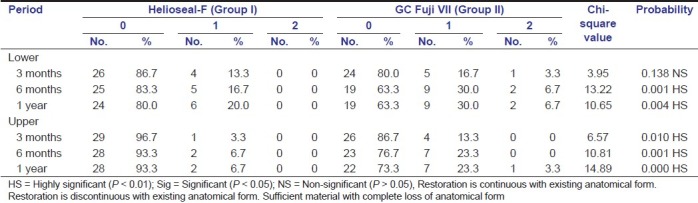
Figure 2.
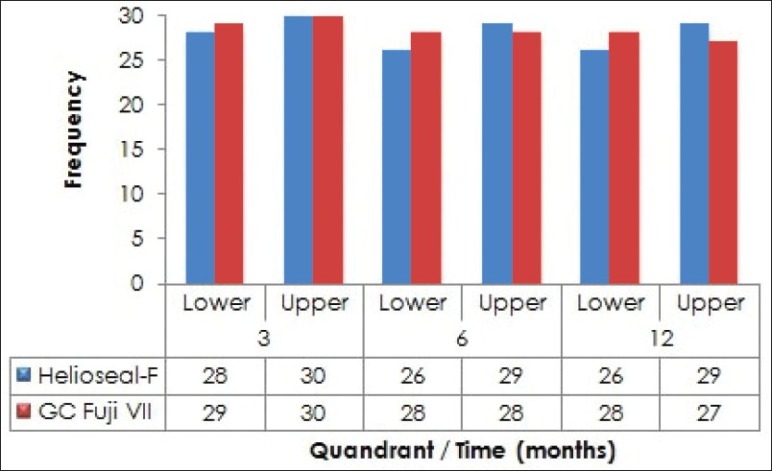
Distribution of cases of Helioseal-F and Fuji VII with no marginal discoloration
Figure 3.
Distribution of cases of Helioseal-F and Fuji VII with good anatomical form
Discussion
Taking into consideration a developing country like India, the preventive measures toward oral health are imperative. Even if the initial cost of preventive measures like sealants may be higher than the cost of restorative materials, in the long term, sealants or any other preventive measure would be more cost-effective as the tooth would be maintained in a state of health.
Helioseal-F is shaded white and comprises 40% inorganic filler, including a fluorosilicate glass that slowly releases fluoride ions over time. Helioseal-F combines mechanical block plus depot fluoride action for double protection. Clinically, Helioseal-F forms a smooth surface after polymerization that is easy to clean and does not allow bacteria to settle. Other advantages are lack of air bubbles, easy application and simple post-polymerization finishing.
Fuji VII has a pink shade when set, and this is in contrast from the tooth structure thus enabling inspection for sealant retention. Another feature of Fuji VII is the “Command Set” property of the material. The unique feature of this material is the absence of any resin component in the material to hasten the setting reaction. It speeds up curing by absorbing the heat energy from the light. Another major advantage of using Glass ionomer VII over Glass ionomer materials is the fluoride release by the sealant, which is considered to be the highest among all Glass ionomers.
In case of partially erupted permanent molars that are prone to caries, their location and gingival covering present difficulties in cleaning and consequently might lead these teeth to become carious before they are fully erupted. Effectiveness of sealant may be jeopardized by the difficulty in obtaining ideal isolation and management of tissue during its application. Glass ionomer Fuji VII has a great advantage that can be applied in areas of minimal isolation, unlike resin-based sealants, where strict isolation and dry field is of utmost importance.
Effectiveness of sealant as a caries preventive agent is dependent upon its full retention. Several authors showed that the caries increment is low when there is full retention of the sealant.[8–10] In the present study, the 3-month evaluation for the lower arch showed 86.7% of retention for resin sealant and 66.7% retention for Glass ionomer sealant. However, the 6-month evaluation showed 83.3% retention for resin sealant and 56.7% retention for Glass ionomer sealant, which was in accordance with other studies.[11,12] The high retention rate reported in this study for resin sealant may be due to the fact that it is easy to apply, good flow, working time is unlimited, chance of air bubble incorporation is less and no mixing is required. White shaded sealants enhance detection by the dentists during the recall evaluation. The patient himself as well as the parents can also check the sealant retention.
The Glass ionomer sealant has been considered a good alternative to resin sealant. They exhibit low technique sensitivity and good adherence in addition to the fluoride releasing property. The Glass ionomer acts as a reservoir from which the added fluoride is gradually released into the oral cavity to inhibit enamel demineralization and enhance remineralization.[13] According to Wendt and Koch, if some part of the sealant is missing in the fissures, there is still enough material in the deeper part to prevent caries.[14] Because of the inherent properties of Glass ionomer sealants like fluoride release and adherence to dental structures, total or partial loss is not considered to be a problem, as a small amount of material remaining in the fissures results in cariostatic effect.[15–17] Considering that fluoride release by Glass ionomer Fuji VII is supposed to be six-times the release of fluoride than any other Glass ionomer, we can say that Glass ionomer Fuji VII does show a promising future in the usage as pit and fissure sealant.
Traditional conventional Glass ionomer when used as a pit and fissure sealant shows very poor retention rates when fully retained.[18–20] A study by Booksman et al., a comparison of 6 months complete retention rates of 92% for concise white light initiated sealant and 2% for the Fuji III Glass ionomer sealant, suggested that the routine use of Fuji III Glass ionomer as a fissure sealant is unreliable. In the present study, Fuji VII had a retention rate of 56.7% and 70% in the lower and upper arch, respectively, at the 1-year evaluation period.
Evaluation of the surface texture of the sealant is rare in the literature. The importance of this parameter lies on the fact that an increased surface texture provides a niche for accumulation of plaque and food debris. This can initiate secondary caries at the margins of the sealant.
In the present study, Glass ionomer sealant suffered a greater loss of surface texture than the resin sealant. This was significant from the 6-month evaluation itself, which can be attributed to the low wear strength of the Glass ionomer sealant to occlusal forces. This leads to a faster surface disintegration, thinning of the sealant and, eventually, fracturing it off from the enamel surface. The combination of these two factors seemed to be the main reason for the Glass ionomer sealant loss. Further improvements on the Glass ionomer sealants should be encouraged in order to produce a more wear-resistant product to withstand the occlusal forces.
Marginal discoloration of a restoration can be considered as an early indicator of its loss of marginal integrity with the adjacent tooth structure. A restoration discolors at its margins when there is marginal breakdown, which creates a rough and irregular surface. This can act as a niche for the accumulation of plaque and food debris and also promote the penetration of oral fluids and cause microleakage, which can lead to secondary caries formation. If there is marginal discoloration that penetrated the sealant margins deep in a pulpal direction, it should be checked thoroughly for any secondary caries, preferably with a radiograph.
In the present study, marginal discoloration was checked visually with the help of a mirror. At baseline, all the sealants were checked visually and scored no cavosurface marginal discoloration. The cavosurface marginal discoloration was not statistically significant in the 6 months and 1 year evaluation. The marginal discoloration of Helioseal-F was higher in the lower arch than in the upper arch. Thus, cavosurface margin discoloration is vital for the sealant as this could be the earliest indicator for the initiation of secondary caries.[21] The marginal discoloration of Fuji VII sealants was similar in the maxillary and mandibular teeth.
Once applied, sealants need to be maintained. When sealants are applied in high caries risk children, review of sealant retention should be part of the recall visit. An earlier guideline in this series has recommended that the recall interval for high caries risk children should not exceed 12 months.[22] If there is particular concern about sealant retention, e.g. if isolation has been difficult to achieve or the sealant has been applied over a suspicious lesion, recall within 6 months is appropriate. A 3-year sealant study involving children aged 5–14 years with partially or newly erupted first or second permanent molars found that the re-treatment rate was higher at the first 6-month recall than at any other recall during the study, irrespective of the method of tooth isolation used (rubber dam or cotton rolls).[23]
Conclusion
The present study suggested that Helioseal-F sealant was better than Glass ionomer Fuji VII sealant with respect to retention, anatomical form and surface texture. Both the materials showed similar results with respect to marginal discoloration. The Helioseal-F sealant performed better in the upper arch than in the lower arch with respect to all properties (except post-operative sensitivity). The Fuji VII sealant performed better in the upper arch than in the lower arch with respect to retention, anatomical form and surface texture. But, with respect to marginal discoloration and post-operative sensitivity, Fuji VII showed similar results both in the upper and in the lower arches. More long-term studies are necessary, nevertheless, to determine the potential benefits of both materials.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
References
- 1.Feldens EG, Feldens CA, de Araujo FB, Maria AL. Invasive technique of pit and fissure sealants in primary molars: A SEM study. J Clin Pediatr Dent. 1994;18:187–90. [PubMed] [Google Scholar]
- 2.Lussi A. Validity of diagnostic and treatment decisions of fissure caries. Caries Res. 1991;25:296–303. doi: 10.1159/000261380. [DOI] [PubMed] [Google Scholar]
- 3.Chestnutt IG, Schafer F, Jacobson AP, Stephen KW. The prevalence and effectiveness of fissure sealants in Scottish adolescents. Br Dent J. 1994;177:125–9. doi: 10.1038/sj.bdj.4808525. [DOI] [PubMed] [Google Scholar]
- 4.Boucheau GF, Jerge CR. The efficacy of sealant treatment in the prevention of pit and fissure dental caries: Review and interpretation of the literature. J Am Dent Assoc. 1976;72:383–7. [Google Scholar]
- 5.Godoy F Garcia, Gwinnett AJ. Penetration of acid solution and gel in occlusal fissures. J Am Dent Assoc. 1987;114:809–10. doi: 10.14219/jada.archive.1987.0164. [DOI] [PubMed] [Google Scholar]
- 6.Ryge G, Snyder M. Evaluating the clinical quality of restorations. J Am Dent Assoc. 1973;87:369–77. doi: 10.14219/jada.archive.1973.0421. [DOI] [PubMed] [Google Scholar]
- 7.Horowitz HS, Heifetz SB, Poulsen S. Adhesive sealant clinical trial: An overview of results after four years in Kalispell, Montana. (44, 46-7).J Prev Dent. 1976;3:38–9. [PubMed] [Google Scholar]
- 8.Poulsen S, Breiruti N, Sadat N. A comparison of retention and the effect on caries of fissure sealing with glass-ionomer and resin-based sealant. Community Dent Oral Epidemiol. 2001;2:298–301. doi: 10.1034/j.1600-0528.2001.290409.x. [DOI] [PubMed] [Google Scholar]
- 9.Fuks Anna B, Grajower Rafael, Shapira Joseph. In vitro assessment of marginal leakage of sealant placed in permanent molars with different etching times. ASDCJ Dent Child. 1984;51(6):425–427. [PubMed] [Google Scholar]
- 10.Jensen OE, Handelmann SL, Diez F Perez. Occlusal wear of four pit and fissure sealant over two years. Pediatr Dent. 1985;7:23–9. [PubMed] [Google Scholar]
- 11.Sol E, Espasa E, Boj JR, Canalda C. Effect of different prophylaxis methods on sealant adhesion. J Clin Pediatr Dent. 2000;24:211–4. [PubMed] [Google Scholar]
- 12.Ibsen RL. use of a filled resin as fissure sealant, one-year clinical study. J Prev Dent. 1973;3:60–5. [PubMed] [Google Scholar]
- 13.Loveren C Van. The antimicrobial action of fluoride and its role in caries inhibition. J Dent Res. 1990;69:676–81. doi: 10.1177/00220345900690S131. [DOI] [PubMed] [Google Scholar]
- 14.Wendt LK, Koch G. Fissure sealant in permanent first molars after 10 years. Swed Dent J. 1988;12:181–5. [PubMed] [Google Scholar]
- 15.Pardi V, Pereira AC, Mialhe FL, Meneghim MC, Ambrosano GM. A 5 year evaluation of two glass ionomer cements used as fissure sealants. Community Dent Oral Epidemiol. 2003;3:386–91. doi: 10.1034/j.1600-0528.2003.00113.x. [DOI] [PubMed] [Google Scholar]
- 16.Ganesh M, Shobha T. Comparative evaluation of marginal sealing ability of Fuji VII and concise pit and fissure sealants. Contemp Dent Pract. 2007;8:10–8. [PubMed] [Google Scholar]
- 17.Herle GP, Joseph T, Varma B, Jayanthi M. Comparative evaluation of glass ionomer and resin fissure sealant using non-invasive and invasive techniques-A SEM and Microleakage study. J Indian Soc Pedod Prev Dent. 2004;2:56–62. [PubMed] [Google Scholar]
- 18.Booksman L, Gratton DR, McCutcheon E, Plotzke OB. Clinical evaluation of glass ionomer cement as a fissure sealant. Quintessence Int. 1987;18:707–9. [PubMed] [Google Scholar]
- 19.Forss H, Saarni UM, Seppa L. Comparison of glass ionomer and resin based fissure sealants: A 2 year clinical trial. Community Dent Oral Epidemiol. 1994;22:21–4. doi: 10.1111/j.1600-0528.1994.tb01563.x. [DOI] [PubMed] [Google Scholar]
- 20.Karlzen-Reuterving G, van Dijken JW. A three year follow-up of glass ionomer cement and resin fissure sealants. ASDC J Dent Child. 1995;62:108–10. [PubMed] [Google Scholar]
- 21.Beauchamp J, Caufield PW, Crall JJ, Donly K, Feigal R, Gooch B, et al. Evidence-based clinical recommendationsfor the use of pit-and-fissure sealants: A report of the American Dental Association Council on ScientificAffairs. J Am Dent Assoc. 2008;139:257–68. doi: 10.14219/jada.archive.2008.0155. [DOI] [PubMed] [Google Scholar]
- 22.Irish Oral Health Services Guideline Initiative. Strategies to prevent dental caries in children and adolescents: Guidance on identifying high caries risk children and developing preventive strategies for high caries riskchildren in Ireland. 2009. [Last accessed on 2010 Aug 12]. [Available from: http://ohsrc.ucc.ie/html/guidelines.html. ]
- 23.Straffon LH, Dennison JB, More FG. Three-year evaluation of sealant: Effect of isolation on efficacy. J Am Dent Assoc. 1985;110:714–7. doi: 10.14219/jada.archive.1985.0425. [DOI] [PubMed] [Google Scholar]