

Abstract
Background:
Musculoskeletal tumors are rare, but their descriptive data in any region are important to reduce mortality rate and improve their management.
Materials and Methods:
Retrospectively, 426 pathologic reports from 1997 to 2008 were reviewed in Shiraz University Orthopedic Hospitals which are the main referral centers for musculoskeletal tumors in south of Iran. We collected and analyzed data on age, gender, anatomical site, and histopathologic types of musculoskeletal tumors.
Results:
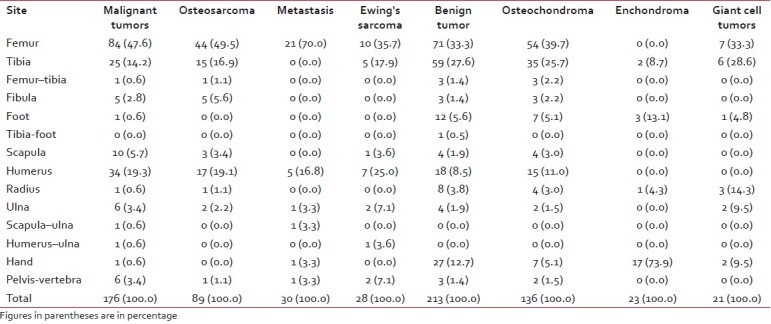
Of the 426 cases, 60.1% were men and 39.9% were women. The commonest malignant bone tumors were osteosarcoma (89; 50.6%), metastasis (30; 17.0%), Ewing's sarcoma (28; 15.9%), and chondrosarcoma (14; 8.0%). The most frequent benign bone tumors were osteochondroma (136; 63.9%), enchondroma (23; 10.8%), giant cell tumor (21; 9.9%), and osteoid osteoma (14; 6.6%). The femur was the most commonly involved site in musculoskeletal tumors. It was followed by the tibia in benign tumors and the humerus in malignant ones. Metastasis (28; 32.6%), soft tissue tumors (18; 20.9%), osteochondroma (10; 11.6%), and osteosarcoma (9; 10.5%) were the most diagnosed bone lesions in patients older than 40.
Conclusion:
There are no significant changes in epidemiology of musculoskeletal tumors in Shiraz, south of Iran, in comparison with other parts of the world.
Keywords: Benign, bone, Iran, malignancy, musculoskeletal, Shiraz, tumor
INTRODUCTION
Malignant neoplasms are one of the main causes of mortality in the world. Skeletal system involvement as metastasis is common. The primary source comes usually from breast, prostate, kidney, lung, and thyroid.[1,2] Diagnosis of these lesions often changes the treatment plan.
Primary bone tumors are rare. They account for 0.2–0.5% of all malignancies in all ages[3] and comprise 3–5% of tumors diagnosed in European children below 15 years and 7–8% in adolescents between 15 and 19 years of age.[4] Incidence of primary malignant bone tumors is about 9 in 1 million people in a year. It is slightly higher in males than females (10/million/year vs. 8/million/year).[5] It is usual for these tumors to be diagnosed late because these neoplasms are uncommon; moreover, their presentations are vague with unspecific signs and symptoms. Sometimes they are recognized and treated like osteomyelitis or simple fracture before exact diagnosis. Therefore, basic epidemiology in each region can help doctors to diagnose and manage them earlier. Also, these studies can guide researchers to find particular risk factors in that area.
According to previous researches, distribution of primary bone tumors is variable in different parts of the world. Highest rates are seen in Europe and the USA, but Asian countries have lower incidence and prevalence.[4,6,7] Although there are several epidemiologic studies of musculoskeletal tumors in the neighboring countries of Iran,[8–11] to the best of our knowledge, this report is the first documented one in Iran.
MATERIALS AND METHODS
We reviewed retrospectively charts and pathologic reports of patients who had undergone musculoskeletal open or excisional biopsies from January 1997 to December 2008. Biopsies had been taken in Chamran and Namazi Hospitals of Shiraz University of Medical Sciences, two main referral centers in the south of Iran. Pathologic slides had been reported by three expert pathologists in musculoskeletal diseases. Also, final diagnosis had been correlated with clinical presentation and radiograph findings by an orthopedic tumor surgeon (senior author). It should be mentioned that although diagnosis of several bone tumors like osteoid osteoma, osteochondroma, and nonossifying fibroma was made clinically and radiographically, open biopsies had been taken due to equivocal diagnosis. Moreover, some reports were the result of excisional biopsies (like osteochondroma and osteoid osteoma). We collected data on age, sex, anatomical site, and histopathologic type of 426 patients.
On the basis of pathologic reports, the tumors were classified as benign bone tumors, malignant bone tumors, and soft tissue tumors. The latter comprised malignant ones like rhabdomyosarcoma, fibrosarcoma, etc. Benign soft tissue tumors were excluded. There were some nonspecific sarcomas like small cell malignant sarcoma and high-grade malignant sarcoma in pathologic reports. We classified them as others in the results.
Description statistics were performed using SPSS software version 18.0 for windows (SPSS Inc., Chicago, IL, USA). Frequency and percentage of the mentioned variables were calculated.
RESULTS
Totally, 426 cases were analyzed. Male to female ratio was 1.5. There were 170 women (39.9%) and 256 men (60.1%). The oldest patient was an 84-year-old man with metastasis. There were two 4-year-old children as the youngest patients, with pathologic reports of osteofibrous dysplasia and soft tissue tumor. As shown in Table 1, 176 patients had malignant bone tumors with the peak frequency seen in patients of age between 5 and 25 years. Also, large proportion of benign bone tumors (161; 75.5%) was seen in patients younger than 25 years of age. Soft tissue tumors occurred more (10; 27.1%) in the age group of 45–54 years.
Table 1.
Distribution of musculoskeletal tumors by age

Overall, the most common pathologic types of bone tumors were osteochondroma (136; 35.0%) and osteosarcoma (89; 22.9%). The femur (159; 40.9%) was the most common anatomical site of bone tumors, followed by the tibia (84; 21.6%), and the humerus (52; 13.4%).
Benign bone tumors
As illustrated in Table 2, osteochondroma (136; 63.9%), enchondroma (23; 10.8%), and giant cell tumors (21; 9.9%) were the most frequent. Men outnumbered women with respect to osteochondroma and enchondroma [Table 3]. This is in contrast to giant cell tumor, wherein 76.2% cases were women. Also, about half of the cases of osteochondroma and enchondroma belonged to 15–24 years (48.5% for osteochondroma and 56.3% for enchondroma). Giant cell tumors were seen mostly in adult patients (third and fourth decades of life).
Table 2.
Frequency and percentage of each bone tumor
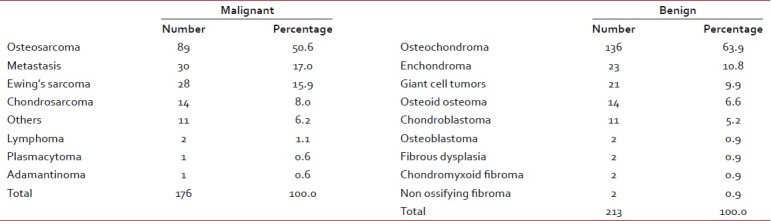
Table 3.
Distribution of the commonest tumors by gender and age

Malignant bone tumors
Of a total of 176 malignant neoplasms, osteosarcoma was the commonest (84; 50.6%), followed by metastasis (30; 17.0%), Ewing's sarcoma (28; 15.9%), and chondrosarcoma (14; 8.0%) [Table 2]. Osteosarcoma and Ewing's sarcoma occurred in males more than females. Male to female ratios were about 1.3 and 6 for osteosarcoma and Ewing's sarcoma, respectively. Both were more frequent in the 15-to 24-year age group. There was no case of Ewing's sarcoma in patients older than 34 years of age [Table 3].
Soft tissue tumors
There were 37 cases with malignancy of soft tissues, with a male predilection (22; 59.5%). The commonest anatomical locations were the thigh (11; 29.7), leg (7; 18.4%), wrist-hand (7; 18.9%), and foot (5; 13.5%).
Musculoskeletal tumors in patients over 40 years
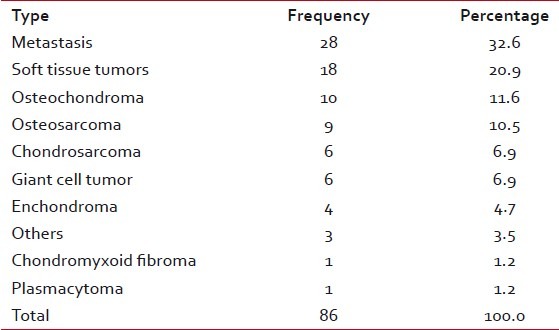
Of 86 patients, 44 (51.2%) were men and 42 (48.8%) were women. Metastasis was the leading pathologic report (28; 32.6%), followed by soft tissue tumors (18; 20.9%). The most diagnosed benign and malignant bone tumors were osteochondroma (10; 11.6%) and osteosarcoma (9; 10.5%) [Table 4].
Table 4.
Frequency and percentage of musculoskeletal tumors in patients older than 40
Anatomical site distribution
Overall, the femur was the most commonly involved long bone. It was followed by the humerus (34; 19.3%) and the tibia (25; 14.2%) in malignant bone tumors, and by the tibia (59, 27.6%) and the wrist-hand (27; 12.7%) in benign neoplasms. Anatomical site distribution of specific tumors is illustrated in Table 5. Of 35 patients with musculoskeletal tumors in wrist and hand, 4 occurred in carpus bones, 8 in metacarpal bones, and 23 in phalanges. The commonest involved finger was the second one (8; 34.7%).
Table 5.
Distribution of musculoskeletal tumors by anatomical site
There are some cases with involvement of more than one bone:
Three cases with osteochondroma of femur and tibia
A case of osteosarcoma of tibia with skip lesion in femur
A 19-year-old man with diagnosis of Ewing's sarcoma involved humerus and ulna
An adolescent girl with osteoid osteoma involved tibia and first metatarsal
A case of metastatic carcinoma to scapula and ulna
DISCUSSION
Primary bone tumors, comprising less than 1% of all malignancies,[3,11] have a high mortality rate. The relative 5-year survival rate is 53.9% for osteosarcoma, 75.2% for chondrosarcoma, and 50.6% for Ewing's sarcoma.[12] Description data and regional distribution of musculoskeletal tumors, as a cause of significant number of deaths, are important for improvement in diagnosis and treatment strategies.
Osteosarcoma is the most common primary malignancy according to several studies.[5,13–17] It is reported to constitute about 35–68% of all primary malignant bone tumors.[8,9,15–17] In our study, osteosarcoma accounted for 50.6% of patients. Male to female ratio was about 1.3, which is the same as that reported in other studies.[4,18] It commonly affects individuals in their first three decades of life. According to this study, none of the patients were less than 5 years of age and the highest number of patients (73; 82.1%) was below 25 years of age. Ewing's sarcoma accounted for 15.9% of all malignant tumors, making it the second most common primary malignancy in bone. Chondrosarcoma was the third (14; 8.0%). Our results are similar to those reported in a study by Rao et al.[10] in India and by Shah et al.[8] in Pakistan. Most reports from developed countries explain chondrosarcoma as the second most frequent.[15,16] Ewing's sarcomas are tumors of the young, with 80% occurring in patients under 20 years. They rarely occur above the age of 30.[5] We did not have any Ewing's sarcoma patient older than 35 years.
In our study, the most frequent benign bone tumor was osteochondroma, followed by enchondroma and giant cell tumor. Osteochondroma accounted for 63.9% of benign bone tumors and 35% of all bone neoplasms. The femur and the tibia were the most affected anatomical sites. The highest percentage of osteochondroma has been reported in our series among all the reviewed papers.[10,15,19] The real frequency of this tumor may be more in our population because of its clinical diagnosis by radiographs. Only excisional biopsies were included in study. The second most frequent benign neoplasm, enchondroma, accounted for about 11% of cases, wherein 73.9% cases were diagnosed in hand. Foot was the next most common site. Giant cell tumors, as the second most common benign tumors in several studies,[15,19] represent about 5% of all bone tumors.[20] In our study, it was seen in 21 patients (9.9%) with involvement of the femur (33.3%), the tibia (28.6%), and the radius (14.3%) in order of frequency.
Metastasis from other sites[1,2] and multiple myeloma are the most likely diagnosed bone lesions in patients older than 40.[21] We had only one case of plasmacytoma. This may be due to its clinical diagnosis by internists and oncologists without biopsy taking. Metastatic carcinoma and soft tissue tumors were the most prevalent diagnosed bone tumors in older patients. Osteochondroma (10; 11.6%) and osteosarcoma (9; 10.5%) were the common primary benign and malignant bone tumors, respectively. Interestingly, bone fibrous tumors were very rare in our study.
There are reasons to explain late diagnosis with poor prognosis of musculoskeletal tumors. Besides the rarity of musculoskeletal tumors and unfamiliarity of general medical staff, they present with nonspecific clinical symptoms. Swelling and pain are seen in other musculoskeletal diseases which are more common than tumors. Epidemiologic studies help in rapid diagnosis and management. Overall, there is not any significant difference between our study and others in literature.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Coleman RE. Clinical features of metastatic bone disease and risk of skeletal morbidity. Clin Cancer Res. 2006;12:6243s–9s. doi: 10.1158/1078-0432.CCR-06-0931. [DOI] [PubMed] [Google Scholar]
- 2.Lewis VO. What's new in musculoskeletal oncology. J Bone Joint Surg Am. 2007;89:1399–407. doi: 10.2106/JBJS.G.00075. [DOI] [PubMed] [Google Scholar]
- 3.Fletcher CD, Unni KK, Mertens F, editors. of World Health Organization classification of tumours. Vol. 5. Lyon, France: IARC Press; 2002. Pathology and genetics of tumours of soft tissue and bone. [Google Scholar]
- 4.Stiller CA, Bielack SS, Jundt G, Steliarova-Foucher E. Bone tumours in European children and adolescents, 1978-1997.Report from the Automated Childhood Cancer Information System project. Eur J Cancer. 2006;42:2124–35. doi: 10.1016/j.ejca.2006.05.015. [DOI] [PubMed] [Google Scholar]
- 5.Bramer JA, Somford MP. The epidemiology of primary skeletal malignancy. Orthop Trauma. 2010;24:247–51. [Google Scholar]
- 6.Parkin DM, Stiller CA, Nectoux J. International variations in the incidence of childhood bone tumours. Int J Cancer. 1993;53:371–6. doi: 10.1002/ijc.2910530305. [DOI] [PubMed] [Google Scholar]
- 7.Eyre R, Feltbower RG, Mubwandarikwa E, Eden TO, McNally RJ. Epidemiology of bone tumours in children and young adults. Pediatr Blood Cancer. 2009;53:941–52. doi: 10.1002/pbc.22194. [DOI] [PubMed] [Google Scholar]
- 8.Shah SH, Muzaffar S, Soomro IN, Pervez S, Hasan SH. Clinico-morphological pattern and frequency of bone cancer. J Pak Med Assoc. 1999;49:110–2. [PubMed] [Google Scholar]
- 9.Omololu AB, Ogunbiyi JO, Ogunlade SO, Alonge TO, Adebisi A, Akang EE. Primary malignant bone tumour in a tropical African University teaching hospital. West Afr J Med. 2002;21:291–3. doi: 10.4314/wajm.v21i4.28001. [DOI] [PubMed] [Google Scholar]
- 10.Rao VS, Pai MR, Rao RC, Adhikary MM. Incidence of primary bone tumours and tumour like lesions in and around Dakshina Kannada district of Karnataka. J Indian Med Assoc. 1996;94:103–4. [PubMed] [Google Scholar]
- 11.Yeole BB, Jussawalla DJ. Descriptive epidemiology of bone cancer in greater Bombay. Indian J Cancer. 1998;35:101–6. [PubMed] [Google Scholar]
- 12.Damron TA, Ward WG, Stewart A. Osteosarcoma, chondrosarcoma, and Ewing's sarcoma: National Cancer Data Base Report. Clin Orthop Relat Res. 2007;459:40–7. doi: 10.1097/BLO.0b013e318059b8c9. [DOI] [PubMed] [Google Scholar]
- 13.Ritter J, Bielack SS. Osteosarcoma. Ann Oncol. 2010;21(Suppl 7):vii320–5. doi: 10.1093/annonc/mdq276. [DOI] [PubMed] [Google Scholar]
- 14.Buckley JD, Pendergrass TW, Buckley CM, Pritchard DJ, Nesbit ME, Provisor AJ, et al. Epidemiology of osteosarcoma and Ewing's sarcoma in childhood: A study of 305 cases by the Children's Cancer Group. Cancer. 1998;83:1440–8. doi: 10.1002/(sici)1097-0142(19981001)83:7<1440::aid-cncr23>3.0.co;2-3. [DOI] [PubMed] [Google Scholar]
- 15.Baena-Ocampo Ldel C, Ramirez-Perez E, Linares-Gonzalez LM, Delgado-Chavez R. Epidemiology of bone tumors in Mexico City: Retrospective clinicopathologic study of 566 patients at a referral institution. Ann Diagn Pathol. 2009;13:16–21. doi: 10.1016/j.anndiagpath.2008.07.005. [DOI] [PubMed] [Google Scholar]
- 16.Blackwell JB, Threlfall TJ, McCaul KA. Primary malignant bone tumours in Western Australia, 1972-1996. Pathology. 2005;37:278–83. doi: 10.1080/00313020500168737. [DOI] [PubMed] [Google Scholar]
- 17.Settakorn J, Lekawanvijit S, Arpornchayanon O, Rangdaeng S, Vanitanakom P, Kongkarnka S, et al. Spectrum of bone tumors in Chiang Mai University Hospital, Thailand according to WHO classification 2002: A study of 1,001 cases. J Med Assoc Thai. 2006;89:780–7. [PubMed] [Google Scholar]
- 18.Stiller CA, Craft AW, Corazziari I. Survival of children with bone sarcoma in Europe since 1978: Results from the EUROCARE study. Eur J Cancer. 2001;37:760–6. doi: 10.1016/s0959-8049(01)00004-1. [DOI] [PubMed] [Google Scholar]
- 19.Odetayo OO. Pattern of bone tumours at the National Orthopaedic Hospital, Lagos, Nigeria. West Afr J Med. 2001;20:161–4. [PubMed] [Google Scholar]
- 20.Turcotte RE. Giant cell tumor of bone. Orthop Clin North Am. 2006;37:35–51. doi: 10.1016/j.ocl.2005.08.005. [DOI] [PubMed] [Google Scholar]
- 21.Heck RK. General principles of tumors. In: Canale ST, Beaty JH, editors. Campbell's Operative Orthopaedics. 11th ed. Philadelphia: Mosby, Elsevier; 2008. pp. 775–854. [Google Scholar]