

Abstract
Vaccines designed to prevent or to treat hepatitis C viral infection must achieve maximum cross reactivity against widely divergent circulating strains. Rational approaches for sequence selection to maximize immunogenicity and minimize genetic distance across circulating strains may enhance vaccine induction of optimal cytotoxic T cell responses. We assessed T cell recognition of potential hepatitis C virus vaccine sequences generated using three rational approaches: 1) combining epitopes with predicted tight binding to the major histocompatibility complex (MHC), 2) consensus sequence (most common amino acid at each position), and 3) representative ancestral sequence that had been derived using Bayesian phylogenetic tools. No correlation was seen between peptide MHC binding affinity and frequency of recognition as measured by an interferon-gamma T cell response in human leukocyte antigen-matched HCV infected individuals. Peptides encoding representative, consensus, and natural variant sequences were then tested for the capacity to expand CD8 T cell populations and to elicit cross-reactive CD8 T cell responses. CD8+ T cells expanded with representative sequence HCV generally more broadly and robustly recognized highly diverse circulating HCV strains than T cell expanded with either consensus sequence or naturally occurring sequence variants. These data support the use of representative sequence in HCV vaccine design.
Keywords: Animals-human, T cells, Infections-viral, Processes-vaccination
Introduction
Approximately 170 million people are infected with hepatitis C virus (HCV) worldwide, with the majority of infected individuals progressing to chronic infection(1). Within the United States, hepatitis C virus infects 4 million individuals and remains the leading cause of liver transplantation and hepatocellular carcinoma (2,3). The estimated morbidity associated with infection is anticipated to rise over the coming decade and treatment is neither universally available nor completely effective. Thus, development of an HCV vaccine to prevent HCV infection remains a critical public health need despite the fact that no vaccine is currently available.
Due in part to its highly error-prone NS5B polymerase, HCV circulates within and between individuals as a quasispecies (4). This swarm of viruses presents an immense challenge for vaccine development. Vaccine strategies meant to overcome this viral diversity must generate a broad immune response, capable of responding to a host of variations. Initial efforts at vaccine development focused on development of sterilizing immunity using an E1/E2 heterodimer (5). Although neutralizing antibodies against envelope can play a role in clearance of infection and re-infection (6-8), specific envelope sequences that drive broadly neutralizing antibody production and sterilizing immunity remain unknown. Generation of robust CD4+ and CD8+ T cell responses is considered critical for long-term immunity (9-11). Development of a cytotoxic T lymphocyte (CTL) response usually occurs early in infection and has a kinetic association with clearance of viremia (12). Failure of a CTL response to control viremia may be due to evasion of the T cell response through a number of mechanisms, including lack of CD4+ T cell help(13,14), T cell exhaustion(15-18), or the emergence of viral escape mutations (19-25). Although the cellular immune response to HCV declines in chronic infection, progressive broadening of the T cell response to HCV is associated with enhanced control of HCV upon repeated reinfection (6). The generation of cellular immunity capable of controlling HCV infection analogous to that observed in people who successfully control repeated HCV infections has become a goal of HCV vaccine development (26).
The T cell responses generated by a vaccine must provide cross-reactivity against highly diverse circulating strains, making selection of HCV vaccine antigens a challenge. Sequence strain selection to induce a T cell response, either for peptide or DNA-based vaccines, has borrowed heavily from HIV vaccine design (27,28). Strategies that deliver only a handful of epitopes or provide cross-coverage of multiple epitopes of a single HCV-protein may maximize recognition of that protein, but at the expense of other regions that may be important in protective immunity. Another strategy that has been shown to be effective for generating cellular immune responses using hepatitis B, lymphocytic choriomeningitis, and lassa virus vaccines in mice is selection of peptides with known high affinity for the major histocompatibility complex (MHC) (29-31). High affinity binders may serve as a stronger immunogenic agent and peptides with high MHC affinity have been shown to be recognized by HBV and HIV infected humans and SIV infected macaques (32-34). However, the frequency of recognition of epitopes selected on the basis of MHC affinity for HCV is unknown.
An alternative to the inclusion of specific epitopes that is commonly employed in vaccine strain selection is the use of a single circulating strain. The choice of which viral strain to use is arbitrary given that no circulating strain resembles the majority of other circulating strains of HCV. The extent to which any individual strain might have mutations that impair immune recognition and allow persistence is also unknown. Strain selection for HCV has focused on existing, well-characterized strains, such as the genotype 1a strain H77 (35). HCV strains between subtypes can differ in nucleotide composition by 20-25% (36). By comparison, a less than 2% amino acid difference can cause a failure in cross-reactivity of the polyclonal response to influenza vaccine (27).
An alternative to selection of specific epitopes or use of a single circulating variant is to use computational methods to minimize the degree of sequence dissimilarity between a vaccine strain and contemporary circulating viruses. One method is to create a consensus strain, whereby the most commonly predicted amino acid at each position is used at each position (27). A limitation of the consensus approach is that escape mutations can become the dominant sequence in regions where the restricting HLA allele is common, as recently demonstrated for HCV (37). This can happen because circulating viral sequences adapt to immune pressure. When an adaptive mutation at a viral residue escapes similar immune responses shared by multiple subjects (e.g. a T cell response restricted by a common allele), that mutation may arise many times in a population such that a consensus of sequences obtained from those individuals may contain the common escape variant. Phylogenetic reconstruction places recent, host-specific changes near the tips of the tree, such that sequences found deeper in the tree may reflect an earlier, shared ancestor (38). While not naturally occurring, ancestral strain sequences are similar to currently circulating HCV strains but may lack the divergent escape mutations carried by circulating strains.
We recently generated both a consensus sequence (cons1a) and a phylogenetic, reconstructed HCV sequence (bole1a) (39). However, the enhanced potential of any computer generated sequence to elicit cross reactive T cell responses has not been demonstrated for HCV. In this paper, we assess the recognition frequency and cross reactivity of HCV sequence peptides generated using the three vaccine development methods described: peptide selection based on high MHC binding capacity, consensus, or the phylogenetically representative bole1a sequence. We provide the first data in HCV to support the use of a synthetically generated sequence (bole1a) to elicit robust CD8+ T cell responses.
Methods
Subjects
The Baltimore Before and After Acute Study of Hepatitis (BBAASH) cohort is a prospective study of injection drug users (IDU) at risk for hepatitis C infection. Eligible participants have a history of or ongoing intravenous drug use and are seronegative for anti-HCV antibodies at enrollment. Written consent was obtained from each participant. Once enrolled, participants receive counseling to reduce intravenous drug use and its complications. Blood is drawn for isolation of serum, plasma, and peripheral blood mononuclear cells (PBMC) in a protocol designed for monthly follow-up as previously described. (40) HCV RNA measurements are used to identify the time of infection and to determine the outcome of infection. Participants with acute HCV infection were referred for evaluation of treatment. The study was approved by the Institutional Review Board at the Johns Hopkins School of Medicine.
Hemigenomic HCV sequencing
A 5.2kb region spanning the 5-untranslated region to the NS3/NS4A junction was reverse transcribed, amplified by nested PCR, and cloned as described previously(41). Briefly, total RNA was extracted from serum using the QIAamp viral RNA mini kit (Qiagen) according to manufacturer's instructions. The 5.2 kb PCR product was generated by a reverse transcription nested PCR strategy. Purified PCR products were cloned into a pCR-XL TOPO vector and transformed into One Shot TOP10 chemically competent cells. Forty clones were picked and amplified with Templiphi to screen for the presence of the insert. Positive clones were sequenced and aligned using CodonCode Aligner (Codon Code Corporation, Dedham, MA).
Human Leukocyte (HLA) binding assay
Quantitative assays to measure the binding of peptides to purified class I molecules were based on the inhibition of binding of a radiolabeled standard peptide (42). Briefly, 1-10 nM of radiolabeled peptide was co-incubated at room temperature with 1 μM to 1 nM of purified MHC in the presence of 1 μM human β2-microglubulin (Scripps Laboratories, San Diego, CA) and a cocktail of protease inhibitors. After a two-day incubation, binding of the radiolabeled peptide to the corresponding MHC class I molecule was determined by capturing MHC/peptide complexes on Greiner Lumitrac 600 microplates (Greiner Bio-one, Longwood, FL) coated with the W6/32 antibody, and measuring bound cpm using the TopCount microscintillation counter (Packard Instrument Co.). Alternatively, following the two-day incubation, the percent of MHC bound radioactivity was determined by size exclusion gel filtration chromatography using a TSK 2000 column.
Generation of HCV genotype 1a consensus sequence (cons1a)
Full-length genotype 1a polypeptide sequences (n=390) were downloaded from GenBank that were circulating in humans and were non-artificial sequences. Sequences were aligned to H77 and the consensus residues calculated with MargFreq program.
Generation of HCV genotype 1a sequence (bole1a)
Construction of the bole1a sequence has been described elsewhere (39). Briefly, the bole1a sequence was constructed using Bayesian phylogenetic and ancestral sequence reconstruction methods along with covariation analysis on the same set of 390 full-length sequences from which the consensus was derived.
Cell culture to generate T cell lines
PMBCs were thawed and stimulated with 10ug/ml of synthetic peptide and 0.5ug/ml of anti-CD28 and anti-CD49d antibodies. Cells were maintained at a density of 2 × 10^6 cells/ml in RPMI 1640 [Sigma-Aldrich], 20% Human serum [Sigma-Aldrich], and 10mM HEPES buffer [Sigma-Aldrich] with 2 mM glutamine and 50 U/ml penicillin-streptomycin. Cells were incubated at 37°C and 5% CO2 with addition of rIL-2 on days 3, 4, 7, and 10 and again following a second round of peptide stimulation on day 10.
Selection of epitope variant peptides and peptide synthesis
In subjects with detectable CD8+ T cell ELISpot responses against HCV, we examined the sequences of the epitope regions over time. When changes away from the consensus sequence occurred in the region of a CD8 T cell epitope, a synthetic peptides corresponding to that sequence as well as the consensus sequence were synthesized commercially by Genemed Synthesis (San Antonio, TX).
Interferon-gamma ELISpot Assay
Ex vivo HCV CD8+ T cell responses were quantified by Human IFN gamma ELISPOT Ready-SET-Go!® assays (eBiosciences) according to manufacturer's instructions. Briefly, PBMC were screened for recognition of HCV-specific antigens using pools of overlapping peptides covering the entire HCV polyprotein and previously defined optimal epitopes. Once responses were determined, additional analyses were performed using decreasing concentrations of synthesized peptides to determine the effects of amino acid substitutions on recognition and the degree to which there was cross-reactivity with circulating variants of the epitope and the bole1a or consensus sequence peptides
To compare the magnitude of T cell responses generated in response to optimal and variant peptides, the same ELISpot assay was performed, using decreasing concentrations of synthesized peptides as antigen. Briefly, PVDF plates were coated with 2.5ug/ml recombinant human anti-IFN-gamma antibody (Endogen M-700A) in 100ul PBS/well at 37°C at 4°C overnight. Plates were washed with sterile PBS eight times before blocking with RPMI +10% FCS for 30 minutes. Either 20,000 or 30,000 cells in R10 media were added to the wells. Decreasing peptide concentrations (10ul/well, 10ug/ml-0.001ug/ml) were added to the well in duplicate. PHA served as a positive control. Plates were incubated for 20 hours at 37°C with 5%CO2. Following incubation, plates were washed with 200ul sterile PBS eight times and blotted dry. Biotin-labeled anti-IFN-gamma (Endogen, M-701B, 0.25ug/ml, 100ul) was added to each well and incubated for 90 min at room temperature. Plates were washed and incubated with streptavidin-alkaline phosphatase (Bio-Rad 170-3554, 100ul) for 45 minutes at room temperature. Following additional washes, the plates were developed with BCIP/NBT Tris-buffer (pH 9.5) solution (Bio-Rad, 170-6532 and 170-6539) according to manual instructions. Plates were dried overnight and read on a Ziess ELISpot plate reader.
Statistical Analysis
Statistical analysis was done using SigmaPlot software version 12.0 (Systat Software, Inc.). Log odds of frequency of recognition based on HLA matched subjects was calculated. Linear regression was performed on the log odds versus log of the IC50 from the in vitro binding assay for HLA-matched sequences for positive responses in all subjects and among those that cleared acute infection.
Results
HLA binding affinity does not predict frequency of recognition
Peptides that bind strongly to the MHC can induce strong pathogen -specific immune responses in other chronic viral infections (32-34). As a result, selection of pathogen peptides with high MHC binding capacity has been used as a strategy in vaccine strain selection. In order to test the hypothesis that high affinity binding to Class I MHC is associated with increased frequency of HCV peptide recognition, the likelihood of recognition of previously identified class I restricted epitopes was correlated with the IC50 binding to its corresponding HLA allele and subtype. Our cohort is routinely screened during acute infection for responses against overlapping genotype 1a peptides, including both long regions of the HCV-H77 polypeptide and known class I epitopes (19). These epitopes have been confirmed as class I restricted epitopes in the literature using cytolytic assays, IFN-gamma ELISpot, intracellular cytokine staining, and/or tetramer staining (43). Assessment during the acute phase of HCV infection is critical since the breadth of HCV epitope recognition declines with progression to chronic infection (10,44).
A total of 60 acutely HCV infected subjects had HLA genotype data available and were screened for HCV specific T cell responses to 36 epitopes with known HLA restriction and binding affinity (Table I). To avoid spuriously negative results, the calculated frequency of responses against each known HLA-restricted epitope in the ELISpot assay includes data for only those subjects with matching HLA genotype and subtype. A positive response for a subject to any epitope was defined as recognition of that epitope in ELISpot testing at any time during infection. The frequency of recognition varied widely between epitopes. For example, we found that nearly half of HLA-A*0201 individuals (14/33, 42%) recognized the HLA-A*02-restricted epitope NS3 1406-1415 (KLVALGINAV) (Table I). In contrast, 15/36 (42%) of the tested epitopes were never recognized. To determine if recognition frequency was correlated with HLA-binding affinity, affinity and recognition frequency were compared.
Table I.
HLA binding affinity and frequency of recognition of peptidesi
| Epitope sequence | AA Starting Position | MHC Allele | HLA binding (IC50, nM) | # of HLA-matched subjects that recognize sequence | Total number of HLA-matched subjects | Fraction recognition |
|---|---|---|---|---|---|---|
| YLLPRRGPRL | 35 | A*02:01 | 125 | 0 | 33 | 0 |
| GPRLGVRAT | 41 | B*07:02 | 15 | 5 | 15 | 0.33 |
| RLGVRATRK | 43 | A*03:01 | 12 | 0 | 16 | 0 |
| RLGVRATRK | 43 | A*11:01 | 6 | 0 | 5 | 0 |
| RLGVRATRK | 43 | A*31:01 | 429 | 0 | 3 | 0 |
| KTSERSQPR | 51 | A*03:01 | 69 | 0 | 16 | 0 |
| KTSERSQPR | 51 | A*11:01 | 38 | 0 | 5 | 0 |
| KTSERSQPR | 51 | A*31:01 | 67 | 0 | 3 | 0 |
| DLMGYIPLV | 132 | A*02:01 | 80 | 3 | 33 | 0.09 |
| LLALLSCLTV | 178 | A*02:01 | 357 | 1 | 33 | 0.03 |
| FLVGQLFTF | 285 | A*02:01 | 67 | 1 | 33 | 0.03 |
| SLLAPGAKQNV | 401 | A*02:01 | 513 | 1 | 33 | 0.03 |
| RLWHYPCTI | 614 | A*02:01 | 23 | 7 | 33 | 0.21 |
| RLWHYPCTV | 614 | A*02:01 | 12 | 11 | 33 | 0.33 |
| RMYVGGVEHR | 630 | A*03:01 | 15 | 1 | 16 | 0.06 |
| RMYVGGVEHR | 630 | A*11:01 | 8 | 0 | 5 | 0 |
| RMYVGGVEHR | 630 | A*31:01 | 95 | 0 | 3 | 0 |
| LEDRDRSEL | 654 | B*40:01 | 426 | 1 | 3 | 0.33 |
| LEDRDRSEL | 654 | B*40:02 | 4267 | 1 | 2 | 0.50 |
| HPALVFDIT | 881 | B*07:02 | 160 | 1 | 15 | 0.07 |
| RPALVFDIT | 881 | B*07:02 | 43 | 0 | 15 | 0 |
| CINGVCWTV | 1073 | A*02:01 | 55 | 13 | 33 | 0.39 |
| CTCGSSDLY | 1123 | A*01:01 | 108 | 0 | 12 | 0 |
| YLVTRHADV | 1131 | A*02:01 | 454 | 0 | 33 | 0 |
| TLGFGAYMSK | 1261 | A*03:01 | 124 | 0 | 16 | 0 |
| LGFGAYMSK | 1262 | A*03:01 | 136 | 0 | 16 | 0 |
| LGFGAYMSK | 1262 | A*11:01 | 21 | 0 | 5 | 0 |
| GIDPNIRTGV | 1273 | A*02:01 | 722 | 3 | 33 | 0.09 |
| GVDPNIRTGV | 1273 | A*02:01 | 351 | 1 | 33 | 0.03 |
| HPNIEEVAL | 1359 | B*35:01 | 99 | 1 | 5 | 0.20 |
| HPNIEEVAL | 1359 | B*35:03 | 6.8 | 1 | 3 | 0.33 |
| IPFYGKAI | 1377 | B*07:02 | 497 | 0 | 15 | 0 |
| HSKKKCDEL | 1395 | B*08:01 | 764 | 7 | 13 | 0.54 |
| KLVALGINAV | 1406 | A*02:01 | 5 | 14 | 33 | 0.42 |
| ATDALMTGY | 1436 | A*01:01 | 1.3 | 5 | 12 | 0.42 |
| SLMAFTAAV | 1789 | A*02:01 | 26 | 3 | 33 | 0.09 |
| LLFNILGGWV | 1807 | A*02:01 | 4 | 0 | 33 | 0 |
| ILAGYGAGV | 1851 | A*02:01 | 116 | 0 | 33 | 0 |
| GVAGALVAFK | 1858 | A*03:01 | 26 | 0 | 16 | 0 |
| GVAGALVAFK | 1858 | A*11:01 | 4 | 0 | 5 | 0 |
| VAGALVAFK | 1859 | A*03:01 | 46 | 0 | 16 | 0 |
| VAGALVAFK | 1859 | A*11:01 | 7 | 0 | 5 | 0 |
| VLSDFKTWL | 1992 | A*02:01 | 305 | 6 | 33 | 0.18 |
| DVVCCSMSY | 2415 | A*26:01 | 25 | 0 | 2 | 0 |
| RLIVFPDLGV | 2578 | A*02:01 | 56 | 4 | 33 | 0.12 |
| RVCEKMALY | 2587 | A*03:01 | 56 | 2 | 16 | 0.13 |
| GLQDCTMLV | 2727 | A*02:01 | 18 | 3 | 33 | 0.09 |
Synthesized peptides encoding known HCV epitope sequences were tested in an in vitro radiolabeled competitive binding assay for binding to the MHC, and the 50% inhibitory concentration (IC50, nM) was determined. BBAASH subjects (n=60) with known HLA typing were screened at acute and chronic time points for responses against overlapping HCV peptides in an IFN-gamma ELISpot. Frequency of recognition of HLA restricted peptide epitopes by subjects with the matched HLA allele and subtype was determined. Subjects lacking the HLA allele required for presentation were excluded. Fraction recognition was calculated as follows: fraction recognition = (number of subjects with matched HLA allele recognizing epitope)/(total number of subjects with restricting HLA allele).
An in vitro competitive binding assay of peptide to the restricting HLA allele was used to assess the strength of binding to the MHC (Table I), with some of these results reported previously (45,46). This assay measures HLA binding affinity of test peptides by determining the concentration of test peptide required to inhibit by 50% binding of radiolabeled peptides to purified HLA molecules of known subtypes. Requiring high concentrations of test peptide to compete with binding of the radiolabeled peptide to the restricting MHC (high IC50) suggests low affinity for that HLA molecule. We compared the frequency of epitope recognition among HLA-matched individuals to the inhibitory concentration in the in vitro HLA binding assay, and found no significant relationship (Figure 1a). For all subjects and responses, HCV peptides with higher HLA binding affinity were no more likely to be recognized than those with low binding affinity (y=-0.1254x-0.4992, r2=0.0492, OR=0.882, 95%CI 0.69-1.12). Moreover, 12/19 (63%) high affinity HCV peptides (IC50 <50nM) were never recognized at any time point examined in our large cohort of acutely HCV infected subjects. This lack of relationship between frequency of recognition and HLA binding affinity held even when we examined the subset of subjects who cleared acute infection and therefore had successful immune responses (Figure 1b, y=-0.1464x-0.2524, r2=-0.0925, OR=0.866, 95% CI=-13.0-12.7). Having found no association between HLA binding affinity and T cell recognition, we evaluated immunogenicity of vaccine strains generated in alternative ways.
Figure 1. Lack of correlation between HLA binding affinity and frequency of recognition.

The frequency of epitope recognition among 60 HCV infected subjects with matching HLA allele and subtype was assessed. HLA binding affinity was determined in an in vitro assay using purified HLA molecules with known allele and subtype. The percent of subjects recognizing HLA-matched epitopes as derived in Table I was graphed relative to the HLA binding affinity for (A) all subjects and (B) subjects that clear infection.
Bole1a sequence induces more robust responses than consensus sequence
The use of consensus or representative sequences has been proposed in vaccine design to minimize the genetic differences between vaccine strains and contemporary isolates. A consensus sequence includes the most common amino acid at each position. However, such a sequence is subject to the frequencies of common HLA alleles in the population and the forces by which these alleles shape circulating viral sequence. Evolutionary forces on the population level due to common HLA alleles play a contributory role on the frequency of circulating escape variants (37,38). The methods used to generate bole1a minimized the genetic distance from circulating sequences while maximizing the likelihood that selected residues represented universally-shared (i.e. rather than individual) evolutionary forces. For comparison, we used the same 390 full length genotype 1a HCV polypeptide sequences that were used to construct bole1a to generate a consensus sequence (cons1a). Bole1a sequence contains a larger number of known T cell epitopes than do the H77 and HCV-1 strains (39) despite H77 and HCV-1 having been used widely to identify HCV epitopes. Bole1a is less likely to contain escape mutations that would impair T cell recognition (27). The cons1a and bole1a sequences were compared for homology across 15 epitopes located between Core and NS3. For 13/15 epitopes, the sequences were identical with the two exceptions noted in Table II. In general, the consensus amino acid residue was clearly defined, with 90% or higher frequency of a single residue. Where the consensus amino acid differed from bole1a, the frequency at the differing position was between 0.405 and 0.523.
Table II.
Bolela and consensus sequences1
| HLA A.A. Location | Sequence | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| C*07 E2 610-618 | D | Y | P | Y | R | L | W | H | Y |
| 0.331 | 0.997 | 0.897 | 1 | 1 | 0.995 | 1 | 1 | 0.992 | |
| H | |||||||||
| 0.405 | |||||||||
| A*01 NS3 1436-1444 | A | T | D | A | L | M | T | G | Y |
| 0.992 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0.477 | |
| F | |||||||||
| 0.523 | |||||||||
Bole1a and cons1a sequences were compared for identity for known MHC class I restricted epitopes. The two epitopes for which bole1a (top) and the consensus (bottom) sequence differ are shown with the frequency of each amino acid at each position.
T cell recognition of artificial HCV sequences has not yet been demonstrated. Therefore, we initially sought to determine if the rationally generated HCV vaccine sequences cons1a and bole1a could induce robust T cell responses and if the sequences differed in their capacity to do so. The cons1a and bole1a sequences were tested for their capacity to expand T cells already primed in vivo against circulating HCV. Lines were generated against peptides encoding the two cons1a and bole1a sequences that differed and then tested for recognition of both the cons1a and bole1a sequences by IFN-gamma ELISpot (Figure 2a and 2b). Supplemental Table II indicates the circulating virus present at the time that the T cells were obtained from the individuals tested. In both cases, the bole1a sequence peptides were able to expand T cell responses that recognized bole1a and consensus sequences for that epitope. In contrast, incubation with the consensus sequence expanded T cells well for only one of the two epitopes. Expansion with consensus NS31436-1444 (ATDALMTGF) resulted in minimal recognition of either variant of that epitope (Figure 2a). Expansion with consensus E2610-618 (HYPYRLWHY) recognition of both variants, but of much lower magnitude than that achieved with bole1a sequence expansion (Figure 2b). Overall, T cells expanded with the bole1a sequence-encoded peptides had greater magnitude responses against both bole1a and consensus sequences than those sequences expanded with cons1a (Figure 2c). Given the improved expansion using bole1a compared to cons1a, future comparisons of the immunogenicity of rationally-designed strains to circulating HCV strains were completed using bole1a sequence for these epitopes.
Figure 2. Relative to the bole1a peptides, consensus peptides fail to or poorly expand T cells specific for peptides from either sequence.

PBMC were stimulated for twenty days with peptides bearing either the bole1a or consensus cons1a sequences. Stimulating peptide sequence is indicated on each graph in the upper right corner. The resulting lines were tested against titrated concentrations of peptides encoding the (--•--) bole1a or cons1a sequence (--○--) in duplicate wells. (A) HLA A*01 HCV NS3 1436-1444, subject 65 (B) HLA C*07 HCV E2 610-618, subject 109 (C) Summation of the total magnitude of response (Total SFC/1e6 cells).
Bole1a sequence better expands CD8+ T cells of diverse HCV specificity
Mutation within CD8+ T cell epitopes occurs frequently, with 69% of epitopes undergoing mutation in the first six months of infection(19). We and others have previously demonstrated selection of and subsequent dominance of HCV variants that evade neutralizing antibody and CD8+ T cells responses (7,19). Thus, any given circulating HCV strain from an individual is likely to contain a large number of escape mutations that allow evasion of T cell recognition (21,47). The capacity of a vaccine strain to induce CD8+ T cell responses to naturally occurring sequence variants will likely be reduced if the vaccine strain used contains escape mutations.
Naturally occurring HCV variants within epitope regions were identified through longitudinal hemigenomic sequencing of HCV from subjects (Supplemental Table I) who recognized CD8+ T cell epitopes of known HLA-restriction. Identified amino acid substitutions within these epitopes and their frequency in the larger Genbank dataset are listed in Table III. Bole1a sequences were identified in circulating sequences for all epitopes investigated, confirming that sequences algorithmically chosen are also found in natural infection. However, circulating variant sequences identified in our cohort were not always present in the larger Genbank dataset, suggesting that the relative frequency of individual variant sequences will vary.
Table III.
Bole1a and identified variant sequences.i
| HCV protein | A.A. Location | Peptide | HLA restriction | Frequency of variants in database (%) |
|---|---|---|---|---|
| Core | 1–9 | MSTNPKPQRK | A*11 | |
| ---D------ | 0 | |||
| --------K- | 1.3 | |||
| ---------Q | 1.8 | |||
| Core | 41–49 | GPRLGVRAT | B*07 | |
| --K------ | 0.3 | |||
| --K---C-- | 0 | |||
| -------T- | 3.8 | |||
| E1 | 285–293 | FLVGQLFTF | A*02 | |
| ------L-- | 0.3 | |||
| ---S----- | 4.9 | |||
| E2 | 610–618 | DYPYRLWHY | C*07 | |
| H-------- | 30 | |||
| H-D------ | 0 | |||
| H-H------ | 0.5 | |||
| H-S------ | 5 | |||
| N-------- | 25 | |||
| E2 | 614–622 | RLWHYPCTI | A*02 | |
| --------A | 1.3 | |||
| --------T | 0 | |||
| --------V | 36 | |||
| E2 | 621–628 | TINYTIFK | A*11 | |
| -------R | 0.5 | |||
| E2 | 654–662 | LEDRDRSEL | B*60 | |
| -----K-K- | 0 | |||
| p7 | 790–799 | LYGMWPLLLL | A*29/C*07 | |
| F--------- | 24 | |||
| NS2 | 957–964 | RDWAHNGL | B*37 | |
| -N---S-L | 0 | |||
| -S---DS- | 0 | |||
| -S----S- | 12 | |||
| NS3 | 1073–1081 | CINGVCWTV | A*02 | |
| ----A---- | 1 | |||
| ----E---- | 0 | |||
| ----E---I | 0 | |||
| --------I | 0.5 | |||
| NS3 | 1111–1120 | WPAPQGARSL | A*26 | |
| -A----S--- | 0.5 | |||
| ------S--- | 25 | |||
| NS3 | 1359–1367 | HPNIEEVAL | B*35 | |
| -S------- | 3.3 | |||
| NS3 | 1395–1403 | HSKKKCDEL | B*08 | |
| -------D- | 0.3 | |||
| ----E---- | 0 | |||
| --------F | 1.8 | |||
| ---R----- | 4.4 | |||
| NS3 | 1406–1415 | KLVALGINAV | A*02 | |
| --G-M----- | 1 | |||
| ---G-V---- | 1.5 | |||
| ----M----- | 3.3 | |||
| --T------- | 1.8 | |||
| ---T------ | 1.5 | |||
| ------V--- | 29 | |||
| ---V--V--- | 0.5 | |||
| NS3 | 1436–1444 | ATDALMTGY | A*01 | |
| --------F | 52 | |||
Subjects who recognized known epitope peptide sequences in an overlapping peptide ELISpot screen were followed longitudinally. Amino acid sequences for bole1a-encoded sequences with their positions in the HCV polypeptide and HLA restriction are re-written in full and are in bold font. Naturally occurring variant sequence mutations identified in our cohort are identified underneath by their changes away from the bole1a sequence. The frequency of occurrence of these variant sequences in the 390 full-length sequences from Genbank is also shown.
Given that representative HCV strains should contain fewer escape mutations than do naturally circulating strains, we hypothesized that CD8+ T cells already primed in vivo against HCV would better recognize bole1a sequence than any individual circulating strain. Expansion capacity of the bole1a sequence relative to naturally occurring sequence variants was tested. Lines were generated against peptides encoding the bole1a sequences or naturally circulating sequence variants. These lines were tested for recognition of the bole1a sequence and the corresponding naturally occurring sequence variants using peptide dilutions in an IFN-gamma ELISpot assay (Figure 3a-g). Lines were successfully generated against 8/8 (100%) peptides encoding bole1a sequences and for 12/18 (67%) peptides derived from naturally occurring sequence variants that did not match bole1a (Figure 3a-g and Figure 2a, b). Incubation of T cells with every naturally occurring sequence variant of the Core41-49 epitope (Figure 3a) as well as three of the four NS31073-1081 (Figure 3f) epitopes failed to generate any ELISpot responses above background to bole1a or sequence variant antigen peptides. This suggests that the naturally occurring variants of these epitopes are less able than bole1a to expand cross reactive T cell responses. In addition, when expansion of T cells with naturally occurring sequence variants did occur, the responses were of diminished magnitude relative to those obtained using the bole1a sequence to expand. The single exception occurred for p7 790-790, where expansion with either the bole1a sequence or a naturally occurring sequence variant produced comparable (within 2-fold) recognition of both sequences across four of five peptide dilutions (Figure 3e). Figure 3h shows the summation of ELISpot responses against 10, 1, and 0.1uM of the bole1a and every variant peptide for each epitope when bole1a is used to expand (left column) or a naturally occurring variant is used to expand (right column). For 6/7 (86%) epitopes, expansion with bole1a sequence resulted in stronger summed responses against itself and sequence variants as measured by total SFC per million cells than did expansion with circulating variants (Figure 3h). The single exception, the p7 790-790 sequence, still resulted in an overall strong magnitude of response against both the bole1a sequence as well as the naturally occurring sequence variant. Thus, bole1a best or comparably expands T cells specific for HCV epitopes, again supporting the superiority of the bole1a sequence over circulating variants in expanding T cell responses broadly specific for HCV.
Figure 3. Relative to peptides encoding bole1a sequence, peptides encoding variant sequences fail to or poorly expand T cells specific for either bole1a or variant sequence.

PBMC were stimulated for twenty days with a peptide of either the bole1a or an identified circulating sequence of that same epitope. In the upper right corner of each graph, the sequence used to expand is shown with amino acid differences from bole1a underlined. The resulting lines were tested against titrated concentrations of peptides in duplicate wells encoding the bole1a sequence (--•--) and all identified circulating variants of that epitope (open shapes) in an IFN-gamma ELISpot assay. (A) HLA B*07 HCV Core 41-49, subject 109 (B) HLA C*07 HCV E2 610-618, subject 109 (C) HLA A*02 HCV E2 614-622, subject 18 (D) HLA A*11 HCV E2 621-628, subject 109 (E) HLA A*29 HCV 97 790-799, subject 109 (F) HLA A*02 HCV NS3 1073-1081, subject 160 (G) HLA A*26 HCV NS3 1111-1120, subject 109 (H) Sum of the magnitude of ELISpot response at peptide dilutions of 10, 1, and 0.1uM (y-axis) when peptides encoding bole1a or a naturally circulating variant was used to expand the T cells (x-axis). The lines connect the bole1a epitope to its corresponding variants.
Bole1a sequence expands T cells of diverse cross-reactivity
The level of cross-reactivity for seven epitopes was compared across individuals to determine if recognition patterns were consistent across subjects and if bole1a expanded T cells specific for variants not seen in that subject. We tested our CD8+ T cell lines against the indicated bole1a sequence for recognition of all the epitope variant peptides identified in our sequencing of circulating HCV strains as well as bole1a and consensus sequence epitopes (Figure 4a-g, Table III, Supplemental Table II). The bole1a sequence was recognized by all subjects and at the two highest concentrations of peptide for every epitope. However, the recognition patterns for specific variants did vary between subjects and by epitope. For example, expansion of T cells with either the peptide encoding bole1a sequence for the epitope NS31436-1444 or its variant resulted in similar recognition patterns of bole1a and the variant sequence (Figure 4a) between subjects. In other cases, expansion with bole1a-encoded sequence resulted in better recognition of the bole1a sequence than any variant, but with differing recognition profiles of variant sequences (4b-d). Finally, expansion with bole1a-encoded sequence resulted in equal recognition of sequence variants and itself for three epitopes (Figure 4e-g), although the extent of variant recognition differed across subjects. T cells expanded from both subjects recognized the D610H and D610N variants well with diminished recognition of the other three sequence variants (Figure 4e). These results suggest that expansion of T cells with bole1a is likely to generate T cell responses that recognize many different circulating HCV variants in different HCV exposed subjects. In contrast, expansion with any given circulating variant results in widely different levels of recognition depending on the subject and HCV exposure.
Figure 4. Bole1a reliably expands T cells with diverse cross-reactivity.

PBMC were stimulated for twenty days with peptides bearing either the bole1a identified variant sequences. The resulting lines were tested against titrated concentrations of peptides encoding an HCV consensus sequence and identified variants in duplicate wells in an IFN-gamma ELISpot. (A) HLA A*01 HCV NS3 1436-1444, subjects 113 and 65 (B) HLA A*11 HCV E2 621-628, subjects 18 and 109 (C) HLA B*08 HCV NS3 1395-1403, subjects 109 and 181 (D) HLA A*26 HCV NS3 1111-1120, subjects 109 and 18 (E) HLA C*07 HCV E2 610-618, subjects 109 and 148 (F) HLA A*02 HCV NS3 1406-1415, subjects 26 and 18 (G) HLA A*02 HCV NS3 1073-1081, subjects 160 and 18.
Bole1a sequence contains the greatest number of optimal epitopes
Following vaccination against any virus, individuals subsequently exposed to that virus will have to respond to a multitude of sequences similar but not identical to those they have already seen. Optimal sequences, or those sequences that stand the greatest likelihood of being cross-reactive in a vaccine, were defined as sequences that a) induce a response when used to generate a line and b) induce maximal responses. For a given epitope position, the optimal sequence was defined experimentally as the sequence that induced the greatest recognition on IFN-gamma ELISpot at a peptide concentration of 1uM. Lines generated that produced only responses less than 100 SFC/1E6 cells were excluded from consideration. Of the ten epitopes assessed, six had a single optimal sequence. For four epitopes, two sequences were equally well recognized with responses of a magnitude within two-fold of the strongest response. When two sequences produced comparable responses, both were deemed optimal. For example, the WPAPQGARSL and WPAPQGSRSL variants of the NS31111-1120 epitope were comparably recognized in multiple ELISpot assays across multiple individuals so both were accepted as optimal sequences.
The presence of the optimal sequence or sequences for the ten epitopes tested was assessed across the 390 full length genotype 1a sequence culled from GenBank as well as the bole1a and cons1a sequences. The tabulated data are presented in Figure 5. Bole1a was found in the group of sequences containing the highest number of optimal epitopes and contains optimal sequence for every of the ten epitopes. Twenty nine other viral strains also contained all of the optimal sequences. In comparison, the cons1a and the H77 sequence were found to contain only 9/10 optimal epitopes despite the H77 strain being used to define most of the known HCV epitopes.
Figure 5. Bole1a sequence contains the greatest number of optimal epitopes.
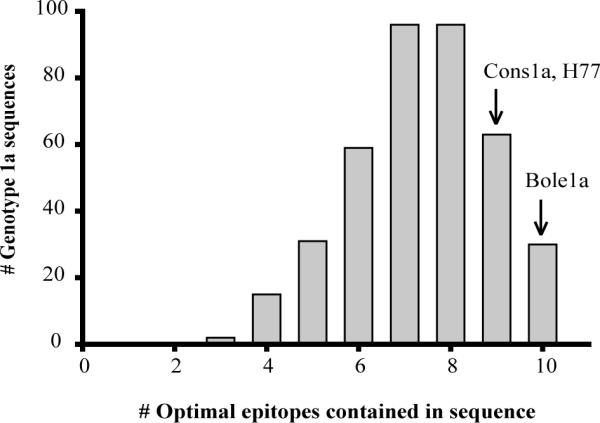
The optimal epitope sequence was defined as the sequence that induced the largest response or within 2-fold response of the largest response on IFN-gamma ELISpot at a peptide concentration of 1uM. Lines generated that produced only responses less than 100 SFC/1E6 cells were excluded from consideration. Full-length genotype 1a sequences culled from GenBank (n=390), cons1a, and bole1a sequences were then screened for the presence of the optimal epitopes and the total number of optimal epitopes per sequence was tallied.
Discussion
Successful vaccination strategies against extremely genetically diverse viruses like HCV will require generation of an immune response that is both broadly cross-reactive and robust against the antigens to which vaccine recipients are subsequently exposed. Significant controversy exists about the best method for selection of a vaccine strain capable of inducing strong, cross-reactive T cell responses against divergent circulating strains. Clinical trials in humans comparing the capacity of different vaccines to induce protective responses are not possible due to expense and limited access to those at risk for infection. Thus, surrogate measures for vaccine strain efficacy are needed. We elected to focus on HCV genotype 1a infectious strains as the most common infectious subtype in the US as well as one of the most difficult to eradicate by therapy. This study presents a comprehensive analysis of the efficacy of a computationally designed genotype 1a HCV sequence (bole1a) to expand HCV specific T cell responses relative to a consensus sequence or individual circulating strains as well as an assessment of the relationship between HLA binding affinity and recognition.
Beginning with the method of selecting peptides with high HLA binding affinity as vaccine antigens, we assessed the frequency of peptide recognition relative to HLA binding capacity. If peptides bound more strongly to the MHC induce recognition more frequently, those peptides might be better candidates for a vaccine sequence. For hepatitis B, lymphocytic choriomeningitis, and HIV, high affinity peptides have been proposed as vaccine antigens based on their enhanced immunogenicity (29,31,33). However, we found no association between HCV peptide binding to the MHC and frequency of recognition in an acutely infected HCV cohort. The lack of association also held among those who clear infection, suggesting that the strength of binding to the MHC does not predict likelihood of developing an effective HCV response. High HLA binding affinity as a method for producing antigen has been proposed in previous studies (45) (46). To evaluate this strategy, a previous study assessed the capacity of peptide with high HLA A*02 binding affinity to prime naïve T cell responses in vitro using human cells and in vivo in mice. While some peptides were capable of inducing responses in both models, it remained unclear from that study if in vivo priming of HCV specific T cells favors recognition of high affinity HLA binders (45). Our study compares in vivo human recognition of peptide epitopes restricted to multiple HLA alleles with widely diverse binding capacity. Another study proposed the use of high HLA binding affinity with ability to bind multiple alleles to select HCV vaccine antigen and found that peptides with comparable HLA binding capacity could have markedly different immunogenicity (46). This is supportive of our study's finding that HLA affinity beyond that needed to bind was not the major determinant of recognition. Once MHC binding beyond a relevant threshold is achieved, other factors such as location of the epitope in the polypeptide, its abundance, thymic education, and T cell precursor frequency appear to play a dominant role in selecting the actual epitope recognized(48,49).
The most commonly proposed method in vaccine design for HCV is selection of an individual circulating sequence. However, any individual circulating sequence is likely to contain escape mutations that result in diminished T cell recognition relative to those generated against the initial infecting sequence(19) or a prototype sequence (50,51). We compared two computationally-derived sequences, consensus (cons1a) and a phylogenetically representative sequence (bole1a). Bole1a is designed to decrease the genetic distance between vaccine and circulating strains and to minimize the inclusion of escape mutations. Although the consensus sequence had shared identity for 13/15 epitopes, our head-to-head comparison of cons1a versus bole1a sequence at the two epitopes that differed demonstrated improved capacity to expand cross reactive HCV specific T cells responses using bole1a. One of the differences present in the consensus sequence represented a known escape mutation in an HLA A*01 restricted epitope. The HCV NS31436-1444 ATDALMGY epitope has been shown to predominate in HLA A*01 populations, despite a known fitness cost (37).
Following vaccination against any virus, individuals subsequently exposed to that virus will have to respond to sequences similar but not identical to those they have already seen. Ability to expand T cell populations that recognize common circulating sequence variants will be critical if any individual sequence is used as a vaccine strain. Bole1a reliably expanded T cell responses against a broad array of circulating variants with greater magnitude of responses compared to naturally occurring sequence variants (Figure 3h). The bole 1a sequence can induce cross-reactive responses against many variants, including those not circulating in that host; an observation noted across subjects.
Although bole1a expanded T cells capable of recognizing many different circulating epitopes, some circulating variants were not recognized well by T cells expanded with any peptide sequence. For example, for the CINGVCWTV bole1a HCV NS31073-1081 peptide epitope, three of the four circulating variants of that sequence (CINGACWTV, CINGECWTI, and CINGECWTV) are very poorly recognized regardless of the peptide variant used to expand T cells(Figure 3f). Vaccination with any sequence is unlikely to induce a response to those sequences. Variant sequences have been shown to escape the T cell response through a number of mechanisms, including decreased binding to the MHC (21) or exploitation of a hole in the repertoire (52). How many T cell epitopes must be recognized to generate an effective T cell response is unknown. Thus, the impact of failure to generate a response to any one viral epitope is unclear. However, failure to generate a single T cell response is unlikely to render a vaccine ineffective.
Compared to T cells expanded with bole1a, T cell expansion with naturally occurring HCV variants generally resulted in diminished recognition of circulating sequence variants. While some variant sequences produced cross-reactive responses, others induced no cross-recognition. In addition, some variant sequences failed to induce any T cell response, making selection of a naturally circulating sequence problematic.
Bole1a contains a larger number of epitopes in the Immune Epitopes Database than did any circulating strain of HCV assessed (39). Experimentally, bole1a and 29 other sequences contain 10 of the 10 epitope sequences tested that were deemed most optimal for expansion and recognition, outperforming both cons1a and H77. The difference might have been greater had a larger number of epitopes been assessed. The H77 sequence contained nearly as many with 9 of the 10 optimal epitopes. This is not surprising given that H77 has been the most commonly used sequence for epitope discovery. Many of the tested epitopes were derived from this sequence in the generation of peptides to screen for T cell responses. Given the historical reliance on H77 for epitope identification, that bole1a contained even more optimal epitopes supports its use. In addition to the experimentally observed reliable expansion of cross-reactive, robust T cell responses, this theoretical assessment of immunogenicity also argues for the use of a representative sequence like bole1a.
The HIV literature debate over HIV strain selection has suggested use of multiple reference sequences, consensus sequences (27), most recent common ancestor sequence, or mosaic sequences. The STEP trial used gag, pol, and nef sequences from three reference strains in an Ad5-based vaccine and failed to reduce the incidence of infection, to lower HIV RNA set points (53), or to induce a difference in CD8+ T cell responses (54). Part of this failure has been attributed to the immunogenicity of the Ad5 vector in prime and boost, but selection of reference strains may also play a role. Vaccination of macaques has not found a consensus sequence to be particularly immunogenic compared to alternative methods (55). However, immune pressure on HIV is intense and consensus sequence contains escape mutations as a result. For example, the frequency of HIV variants in HLA B*57, HLA-B*27, and HLA-B*51 restricted sequences has been correlated with the prevalence of the restricting allele in populations, suggesting an evolving relationship between HIV sequence and HLA frequency (56). Finally, the use of computer generated sequences in vaccine design has been proposed for HCV (57) with coverage compared to reference strain H77, but direct testing of immunogenicity and cross-recognition had not been demonstrated previously. Our study provides the first evidence that a computer generated HCV sequence can both expand cross reactive T cell responses and be recognized as antigen.
There are some limitations to our study. Lines generated against a sequence offer insight into recognition of sequence variants but may artificially expand one subset of the polyclonal population in a way that would not occur in vivo. We measured only IFN-gamma production as a marker for T cell reactivity. Although poly-functional T cell responses are associated with control in some vaccine studies (58), there is an excellent correlation between IFN-gamma production and control of HCV (12,59). In addition, we did not examine sequence cross-reactivity in multiple genotypes due to a relative infrequency of non-genotype 1 infections in our cohort. However, certain epitopes and escape variants are conserved across genotypes. For example, the escape variant Y1444F is the same variant in genotypes 1a, 1b, and 3a infection (37). Thus, our results may be relevant in non-genotype 1 infections. We are also limited to assessing responses that appear in the peripheral blood. Other studies have implicated an increased breadth and frequency in the CD8+ T cell response in the intrahepatic compartment versus the peripheral response (50,60). Thus, we may have underestimated the frequency of responses detected. Furthermore, we were unable to assess HLA-binding affinity for all known epitopes, including those of HLA-C as well as the B*27 and B*57 alleles. The presence of either the B*27 or the B*57 allele in HCV infected subjects is associated with increased frequency of HCV clearance (61). Finally, we did not assess recognition or cross-reactivity of helper responses, which are known to play a role in controlling infection (13,62).
We also demonstrate capacity to expand from previously HCV-exposed individuals rather than immunogenicity in HCV uninfected subjects. Ideally, vaccination of naïve hosts with every variant and artificial sequence would be performed. The assessment of the subsequent immune response would allow a more accurate comparison of immunogenicity. Given the lack of feasibility of such experiments, we assessed capacity to expand and cross-reactivity as a surrogate.
In conclusion, generation of a successful T cell vaccine will require a strain that is immunogenic as well as cross-reactive within genotype, or with multiple genotypes. We have demonstrated for the first time the efficacy of a synthetic representative sequence, bole1a, to expand a robust and cross-reactive CD8+ T cell response and its superiority over other strategies. We anticipate that this strategy will help direct vaccine sequence selection for hepatitis C infection.
Supplementary Material
Acknowledgments
The authors have no conflicting financial interests. We thank Drew Pardoll for helpful comments on the manuscript. We also thank David Hudson for assistance with subject recruitment.
Footnotes
Grant support: Funding for this research was provided by NIH R01DA024565, The Damon Runyon Cancer Research Foundation, and NIH U19AI088791
Reference List
- 1.Schwartlander B. Global burden of disease. Lancet. 1997;350:141–142. doi: 10.1016/S0140-6736(05)61844-2. [DOI] [PubMed] [Google Scholar]
- 2.Alter MJ, Kruszon-Moran D, Nainan OV, McQuillan GM, Gao F, Moyer LA, Kaslow RA, Margolis HS. The prevalence of hepatitis C virus infection in the United States, 1988 through 1994. N. Engl. J. Med. 1999;341:556–562. doi: 10.1056/NEJM199908193410802. [DOI] [PubMed] [Google Scholar]
- 3.Wong JB, McQuillan GM, McHutchison JG, Poynard T. Estimating future hepatitis C morbidity, mortality, and costs in the United States. Am. J. Public Health. 2000;90:1562–1569. doi: 10.2105/ajph.90.10.1562. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Martell M, Esteban JI, Quer J, Genesca J, Weiner A, Esteban R, Guardia J, Gomez J. Hepatitis C virus (HCV) circulates as a population of different but closely related genomes: quasispecies nature of HCV genome distribution. J. Virol. 1992;66:3225–3229. doi: 10.1128/jvi.66.5.3225-3229.1992. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Choo QL, Kuo G, Ralston R, Weiner A, Chien D, van Nest G, Han J, Berger K, Thudium K, Kuo C. Vaccination of chimpanzees against infection by the hepatitis C virus. Proc. Natl. Acad. Sci. USA. 1994;91:1294–1298. doi: 10.1073/pnas.91.4.1294. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Osburn WO, Fisher BE, Dowd KA, Urban G, Liu L, Ray SC, Thomas DL, Cox AL. Spontaneous Control of Primary Hepatitis C Virus Infection and Immunity Against Persistent Reinfection. Gastroenterology. 2009 doi: 10.1053/j.gastro.2009.09.017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Dowd KA, Netski DM, Wang XH, Cox AL, Ray SC. Selection Pressure from Neutralizing Antibodies Drives Sequence Evolution during Acute Infection with Hepatitis C Virus. Gastroenterology. 2009;136:2377–2386. doi: 10.1053/j.gastro.2009.02.080. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Pestka JM, Zeisel MB, Blaser E, Schurmann P, Bartosch B, Cosset FL, Patel AH, Meisel H, Baumert J, Viazov S, Rispeter K, Blum HE, Roggendorf M, Baumert TF. Rapid induction of virus-neutralizing antibodies and viral clearance in a single-source outbreak of hepatitis C. Proc. Natl. Acad. Sci. U. S. A. 2007;104:6025–6030. doi: 10.1073/pnas.0607026104. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Cooper S, Erickson AL, Adams EJ, Kansopon J, Weiner AJ, Chien DY, Houghton M, Parham P, Walker CM. Analysis of a successful immune response against hepatitis C virus. Immunity. 1999;10:439–449. doi: 10.1016/s1074-7613(00)80044-8. [DOI] [PubMed] [Google Scholar]
- 10.Gruner NH, Gerlach TJ, Jung MC, Diepolder HM, Schirren CA, Schraut WW, Hoffmann R, Zachoval R, Santantonio T, Cucchiarini M, Cerny A, Pape GR. Association of hepatitis C virus-specific CD8+ T cells with viral clearance in acute hepatitis C. J. Infect. Dis. 2000;181:1528–1536. doi: 10.1086/315450. [DOI] [PubMed] [Google Scholar]
- 11.Lechner F, Wong DK, Dunbar PR, Chapman R, Chung RT, Dohrenwend P, Robbins G, Phillips R, Klenerman P, Walker BD. Analysis of successful immune responses in persons infected with hepatitis C virus. J. Exp. Med. 2000;191:1499–1512. doi: 10.1084/jem.191.9.1499. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Shoukry NH, Grakoui A, Houghton M, Chien DY, Ghrayeb J, Reimann KA, Walker CM. Memory CD8+ T cells are required for protection from persistent hepatitis C virus infection. J. Exp. Med. 2003;197:1645–1655. doi: 10.1084/jem.20030239. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Day CL, Lauer GM, Robbins GK, McGovern B, Wurcel AG, Gandhi RT, Chung RT, Walker BD. Broad specificity of virus-specific CD4+ T-helper-cell responses in resolved hepatitis C virus infection. J. Virol. 2002;76:12584–12595. doi: 10.1128/JVI.76.24.12584-12595.2002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Eckels DD, Wang H, Bian TH, Tabatabai N, Gill JC. Immunobiology of hepatitis C virus (HCV) infection: the role of CD4 T cells in HCV infection. Immunol. Rev. 2000;174:90–97. doi: 10.1034/j.1600-0528.2002.017403.x. [DOI] [PubMed] [Google Scholar]
- 15.Rutebemberwa A, Ray SC, Astemborski J, Levine J, Liu L, Dowd KA, Clute S, Wang C, Korman A, Sette A, Sidney J, Pardoll DM, Cox AL. High-programmed death-1 levels on hepatitis C virus-specific T cells during acute infection are associated with viral persistence and require preservation of cognate antigen during chronic infection. J. Immunol. 2008;181:8215–8225. doi: 10.4049/jimmunol.181.12.8215. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Kasprowicz V, Schulze zur WJ, Kuntzen T, Nolan BE, Longworth S, Berical A, Blum J, McMahon C, Reyor LL, Elias N, Kwok WW, McGovern BG, Freeman G, Chung RT, Klenerman P, Lewis-Ximenez L, Walker BD, Allen TM, Kim AY, Lauer GM. High level of PD-1 expression on hepatitis C virus (HCV)-specific CD8+ and CD4+ T cells during acute HCV infection, irrespective of clinical outcome. J. Virol. 2008;82:3154–3160. doi: 10.1128/JVI.02474-07. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Radziewicz H, Ibegbu CC, Fernandez ML, Workowski KA, Obideen K, Wehbi M, Hanson HL, Steinberg JP, Masopust D, Wherry EJ, Altman JD, Rouse BT, Freeman GJ, Ahmed R, Grakoui A. Liver-infiltrating lymphocytes in chronic human hepatitis C virus infection display an exhausted phenotype with high levels of PD-1 and low levels of CD127 expression. J. Virol. 2007;81:2545–2553. doi: 10.1128/JVI.02021-06. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Day CL, Kaufmann DE, Kiepiela P, Brown JA, Moodley ES, Reddy S, Mackey EW, Miller JD, Leslie AJ, Depierres C, Mncube Z, Duraiswamy J, Zhu B, Eichbaum Q, Altfeld M, Wherry EJ, Coovadia HM, Goulder PJ, Klenerman P, Ahmed R, Freeman GJ, Walker BD. PD-1 expression on HIV-specific T cells is associated with T-cell exhaustion and disease progression. Nature. 2006 doi: 10.1038/nature05115. [DOI] [PubMed] [Google Scholar]
- 19.Cox AL, Mosbruger T, Mao Q, Liu Z, Wang XH, Yang HC, Sidney J, Sette A, Pardoll D, Thomas DL, Ray SC. Cellular immune selection with hepatitis C virus persistence in humans. J Exp. Med. 2005;201:1741–1752. doi: 10.1084/jem.20050121. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Allen TM, Altfeld M, Yu XG, O'Sullivan KM, Lichterfeld M, Le Gall S, John M, Mothe BR, Lee PK, Kalife ET, Cohen DE, Freedberg KA, Strick DA, Johnston MN, Sette A, Rosenberg ES, Mallal SA, Goulder PJ, Brander C, Walker BD. Selection, transmission, and reversion of an antigen-processing cytotoxic T-lymphocyte escape mutation in human immunodeficiency virus type 1 infection. J. Virol. 2004;78:7069–7078. doi: 10.1128/JVI.78.13.7069-7078.2004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Timm J, Lauer GM, Kavanagh DG, Sheridan I, Kim AY, Lucas M, Pillay T, Ouchi K, Reyor LL, Zur Wiesch JS, Gandhi RT, Chung RT, Bhardwaj N, Klenerman P, Walker BD, Allen TM. CD8 epitope escape and reversion in acute HCV infection. J. Exp. Med. 2004;200:1593–1604. doi: 10.1084/jem.20041006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Allen TM, O'Connor DH, Jing P, Dzuris JL, Mothe BR, Vogel TU, Dunphy E, Liebl ME, Emerson C, Wilson N, Kunstman KJ, Wang X, Allison DB, Hughes AL, Desrosiers RC, Altman JD, Wolinsky SM, Sette A, Watkins DI. Tat-specific cytotoxic T lymphocytes select for SIV escape variants during resolution of primary viraemia. Nature. 2000;407:386–390. doi: 10.1038/35030124. [DOI] [PubMed] [Google Scholar]
- 23.Jones NA, Wei X, Flower DR, Wong M, Michor F, Saag MS, Hahn BH, Nowak MA, Shaw GM, Borrow P. Determinants of human immunodeficiency virus type 1 escape from the primary CD8+ cytotoxic T lymphocyte response. J. Exp. Med. 2004;200:1243–1256. doi: 10.1084/jem.20040511. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Yokomaku Y, Miura H, Tomiyama H, Kawana-Tachikawa A, Takiguchi M, Kojima A, Nagai Y, Iwamoto A, Matsuda Z, Ariyoshi K. Impaired processing and presentation of cytotoxic-T-lymphocyte (CTL) epitopes are major escape mechanisms from CTL immune pressure in human immunodeficiency virus type 1 infection. J Virol. 2004;78:1324–1332. doi: 10.1128/JVI.78.3.1324-1332.2004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Erickson AL, Kimura Y, Igarashi S, Eichelberger J, Houghton M, Sidney J, McKinney D, Sette A, Hughes AL, Walker CM. The outcome of hepatitis C virus infection is predicted by escape mutations in epitopes targeted by cytotoxic T lymphocytes. Immunity. 2001;15:883–895. doi: 10.1016/s1074-7613(01)00245-x. [DOI] [PubMed] [Google Scholar]
- 26.Houghton M, Abrignani S. Prospects for a vaccine against the hepatitis C virus. Nature. 2005;436:961–966. doi: 10.1038/nature04081. [DOI] [PubMed] [Google Scholar]
- 27.Gaschen B, Taylor J, Yusim K, Foley B, Gao F, Lang D, Novitsky V, Haynes B, Hahn BH, Bhattacharya T, Korber B. Diversity considerations in HIV-1 vaccine selection. Science. 2002;296:2354–2360. doi: 10.1126/science.1070441. [DOI] [PubMed] [Google Scholar]
- 28.McElrath MJ, Haynes BF. Induction of immunity to human immunodeficiency virus type-1 by vaccination. Immunity. 2010;33:542–544. doi: 10.1016/j.immuni.2010.09.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Sette A, Vitiello A, Reherman B, Fowler P, Nayersina R, Kast WM, Melief CJ, Oseroff C, Yuan L, Ruppert J, Sidney J, del Guercio MF, Southwood S, Kubo RT, Chesnut RW, Grey HM, Chisari FV. The relationship between class I binding affinity and immunogenicity of potential cytotoxic T cell epitopes. J. Immunol. 1994;153:5586–5592. [PubMed] [Google Scholar]
- 30.Botten J, Alexander J, Pasquetto V, Sidney J, Barrowman P, Ting J, Peters B, Southwood S, Stewart B, Rodriguez-Carreno MP, Mothe B, Whitton JL, Sette A, Buchmeier MJ. Identification of protective Lassa virus epitopes that are restricted by HLA-A2. J. Virol. 2006;80:8351–8361. doi: 10.1128/JVI.00896-06. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Kotturi MF, Scott I, Wolfe T, Peters B, Sidney J, Cheroutre H, von Herrath MG, Buchmeier MJ, Grey H, Sette A. Naive precursor frequencies and MHC binding rather than the degree of epitope diversity shape CD8+ T cell immunodominance. J. Immunol. 2008;181:2124–2133. doi: 10.4049/jimmunol.181.3.2124. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Loffredo JT, Sidney J, Wojewoda C, Dodds E, Reynolds MR, Napoe G, Mothe BR, O'Connor DH, Wilson NA, Watkins DI, Sette A. Identification of seventeen new simian immunodeficiency virus-derived CD8+ T cell epitopes restricted by the high frequency molecule, Mamu-A*02, and potential escape from CTL recognition. J. Immunol. 2004;173:5064–5076. doi: 10.4049/jimmunol.173.8.5064. [DOI] [PubMed] [Google Scholar]
- 33.Corbet S, Nielsen HV, Vinner L, Lauemoller S, Therrien D, Tang S, Kronborg G, Mathiesen L, Chaplin P, Brunak S, Buus S, Fomsgaard A. Optimization and immune recognition of multiple novel conserved HLA-A2, human immunodeficiency virus type 1-specific CTL epitopes. J. Gen. Virol. 2003;84:2409–2421. doi: 10.1099/vir.0.19152-0. [DOI] [PubMed] [Google Scholar]
- 34.Mizukoshi E, Sidney J, Livingston B, Ghany M, Hoofnagle JH, Sette A, Rehermann B. Cellular immune responses to the hepatitis B virus polymerase. J. Immunol. 2004;173:5863–5871. doi: 10.4049/jimmunol.173.9.5863. [DOI] [PubMed] [Google Scholar]
- 35.Folgori A, Capone S, Ruggeri L, Meola A, Sporeno E, Ercole BB, Pezzanera M, Tafi R, Arcuri M, Fattori E, Lahm A, Luzzago A, Vitelli A, Colloca S, Cortese R, Nicosia A. A T-cell HCV vaccine eliciting effective immunity against heterologous virus challenge in chimpanzees. Nat. Med. 2006;12:190–197. doi: 10.1038/nm1353. [DOI] [PubMed] [Google Scholar]
- 36.Simmonds P, Bukh J, Combet C, Deleage G, Enomoto N, Feinstone S, Halfon P, Inchauspe G, Kuiken C, Maertens G, Mizokami M, Murphy DG, Okamoto H, Pawlotsky JM, Penin FO, Sablon E, Tadasu SI, Stuyver L, Thiel HJ, Viazov S, Weiner A, Widell A. Consensus proposals for a unified system of nomenclature of hepatitis C virus genotypes. Hepatology. 2005;42:962–973. doi: 10.1002/hep.20819. [DOI] [PubMed] [Google Scholar]
- 37.Neumann-Haefelin C, Frick DN, Wang JJ, Pybus OG, Salloum S, Narula GS, Eckart A, Biezynski A, Eiermann T, Klenerman P, Viazov S, Roggendorf M, Thimme R, Reiser M, Timm J. Analysis of the evolutionary forces in an immunodominant CD8 epitope in hepatitis C virus at a population level. J. Virol. 2008;82:3438–3451. doi: 10.1128/JVI.01700-07. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Bhattacharya T, Daniels M, Heckerman D, Foley B, Frahm N, Kadie C, Carlson J, Yusim K, McMahon B, Gaschen B, Mallal S, Mullins JI, Nickle DC, Herbeck J, Rousseau C, Learn GH, Miura T, Brander C, Walker B, Korber B. Founder effects in the assessment of HIV polymorphisms and HLA allele associations. Science. 2007;315:1583–1586. doi: 10.1126/science.1131528. [DOI] [PubMed] [Google Scholar]
- 39.Munshaw S, Bailey JR, Liu L, Osburn W, Burke KP, Cox AL, Ray SC. Computational reconstruction of bole1a, a representative synthetic hepatitis C subtype 1a viral genome. J. Virol. doi: 10.1128/JVI.05959-11. in press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Cox AL, Netski DM, Mosbruger T, Sherman SG, Strathdee S, Ompad D, Vlahov D, Chien D, Shyamala V, Ray SC, Thomas DL. Prospective evaluation of community-acquired acute-phase hepatitis C virus infection. Clin. Infect. Dis. 2005;40:951–958. doi: 10.1086/428578. [DOI] [PubMed] [Google Scholar]
- 41.Liu Z, Netski DM, Mao Q, Laeyendecker O, Ticehurst JR, Wang XH, Thomas DL, Ray SC. Accurate representation of the hepatitis C virus quasispecies in 5.2-kilobase amplicons. J Clin. Microbiol. 2004;42:4223–4229. doi: 10.1128/JCM.42.9.4223-4229.2004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Sidney J, Southwood S, Oseroff C, Del Guercio JF, Sette A, Grey H. Measurement of MHC/Peptide Interactions by Gel Filtration. In: Bierer B, Coligan JE, Margulies DH, Shevach EM, Strober W, Kruisbeek A, editors. Current Protocols in Immunology. John Wiley & Sons, Inc.; 1998. pp. 18.3.1–18.3.19. [Google Scholar]
- 43.Ward S, Lauer G, Isba R, Walker B, Klenerman P. Cellular immune responses against hepatitis C virus: the evidence base 2002. Clin. Exp. Immunol. 2002;128:195–203. doi: 10.1046/j.1365-2249.2002.01840.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Cox AL, Mosbruger T, Lauer GM, Pardoll D, Thomas DL, Ray SC. Comprehensive analyses of CD8+ T cell responses during longitudinal study of acute human hepatitis C. Hepatology. 2005;42:104–112. doi: 10.1002/hep.20749. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Wentworth PA, Sette A, Celis E, Sidney J, Southwood S, Crimi C, Stitely S, Keogh E, Wong NC, Livingston B, Alazard D, Vitiello A, Grey HM, Chisari FV, Chesnut RW, Fikes J. Identification of A2-restricted hepatitis C virus-specific cytotoxic T lymphocyte epitopes from conserved regions of the viral genome. Int. Immunol. 1996;8:651–659. doi: 10.1093/intimm/8.5.651. [DOI] [PubMed] [Google Scholar]
- 46.Chang KM, Gruener NH, Southwood S, Sidney J, Pape GR, Chisari FV, Sette A. Identification of HLA-A3 and -B7-restricted CTL response to hepatitis C virus in patients with acute and chronic hepatitis C. J. Immunol. 1999;162:1156–1164. [PubMed] [Google Scholar]
- 47.Ray SC, Fanning L, Wang XH, Netski DM, Kenny-Walsh E, Thomas DL. Divergent and convergent evolution after a common-source outbreak of hepatitis C virus. J Exp. Med. 2005;201:1753–1759. doi: 10.1084/jem.20050122. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Yewdell JW, Bennink JR. Immunodominance in major histocompatibility complex class I-restricted T lymphocyte responses. Annu. Rev. Immunol. 1999;17:51–88. doi: 10.1146/annurev.immunol.17.1.51. 51-88. [DOI] [PubMed] [Google Scholar]
- 49.Assarsson E, Sidney J, Oseroff C, Pasquetto V, Bui HH, Frahm N, Brander C, Peters B, Grey H, Sette A. A quantitative analysis of the variables affecting the repertoire of T cell specificities recognized after vaccinia virus infection. J. Immunol. 2007;178:7890–7901. doi: 10.4049/jimmunol.178.12.7890. [DOI] [PubMed] [Google Scholar]
- 50.Neumann-Haefelin C, Timm J, Spangenberg HC, Wischniowski N, Nazarova N, Kersting N, Roggendorf M, Allen TM, Blum HE, Thimme R. Virological and immunological determinants of intrahepatic virus-specific CD8+ T-cell failure in chronic hepatitis C virus infection. Hepatology. 2008;47:1824–1836. doi: 10.1002/hep.22242. [DOI] [PubMed] [Google Scholar]
- 51.Salloum S, Oniangue-Ndza C, Neumann-Haefelin C, Hudson L, Giugliano S, aus dem SM, Nattermann J, Spengler U, Lauer GM, Wiese M, Klenerman P, Bright H, Scherbaum N, Thimme R, Roggendorf M, Viazov S, Timm J. Escape from HLA-B*08-restricted CD8 T cells by hepatitis C virus is associated with fitness costs. J. Virol. 2008;82:11803–11812. doi: 10.1128/JVI.00997-08. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Wolfl M, Rutebemberwa A, Mosbruger T, Mao Q, Li HM, Netski D, Ray SC, Pardoll D, Sidney J, Sette A, Allen T, Kuntzen T, Kavanagh DG, Kuball J, Greenberg PD, Cox AL. Hepatitis C virus immune escape via exploitation of a hole in the T cell repertoire. J. Immunol. 2008;181:6435–6446. doi: 10.4049/jimmunol.181.9.6435. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Buchbinder SP, Mehrotra DV, Duerr A, Fitzgerald DW, Mogg R, Li D, Gilbert PB, Lama JR, Marmor M, Del RC, McElrath MJ, Casimiro DR, Gottesdiener KM, Chodakewitz JA, Corey L, Robertson MN. Efficacy assessment of a cell-mediated immunity HIV-1 vaccine (the Step Study): a double-blind, randomised, placebo-controlled, test-of-concept trial. Lancet. 2008;372:1881–1893. doi: 10.1016/S0140-6736(08)61591-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.McElrath MJ, De Rosa SC, Moodie Z, Dubey S, Kierstead L, Janes H, Defawe OD, Carter DK, Hural J, Akondy R, Buchbinder SP, Robertson MN, Mehrotra DV, Self SG, Corey L, Shiver JW, Casimiro DR. HIV-1 vaccine-induced immunity in the test-of-concept Step Study: a case-cohort analysis. Lancet. 2008;372:1894–1905. doi: 10.1016/S0140-6736(08)61592-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Santra S, Liao HX, Zhang R, Muldoon M, Watson S, Fischer W, Theiler J, Szinger J, Balachandran H, Buzby A, Quinn D, Parks RJ, Tsao CY, Carville A, Mansfield KG, Pavlakis GN, Felber BK, Haynes BF, Korber BT, Letvin NL. Mosaic vaccines elicit CD8+ T lymphocyte responses that confer enhanced immune coverage of diverse HIV strains in monkeys. Nat. Med. 2010;16:324–328. doi: 10.1038/nm.2108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Kawashima Y, Pfafferott K, Frater J, Matthews P, Payne R, Addo M, Gatanaga H, Fujiwara M, Hachiya A, Koizumi H, Kuse N, Oka S, Duda A, Prendergast A, Crawford H, Leslie A, Brumme Z, Brumme C, Allen T, Brander C, Kaslow R, Tang J, Hunter E, Allen S, Mulenga J, Branch S, Roach T, John M, Mallal S, Ogwu A, Shapiro R, Prado JG, Fidler S, Weber J, Pybus OG, Klenerman P, Ndung'u T, Phillips R, Heckerman D, Harrigan PR, Walker BD, Takiguchi M, Goulder P. Adaptation of HIV-1 to human leukocyte antigen class I. Nature. 2009;458:641–645. doi: 10.1038/nature07746. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Yusim K, Fischer W, Yoon H, Thurmond J, Fenimore PW, Lauer G, Korber B, Kuiken C. Genotype 1 and global hepatitis C T-cell vaccines designed to optimize coverage of genetic diversity. J. Gen. Virol. 2010;91:1194–1206. doi: 10.1099/vir.0.017491-0. [DOI] [PubMed] [Google Scholar]
- 58.Seder RA, Darrah PA, Roederer M. T-cell quality in memory and protection: implications for vaccine design. Nat. Rev. Immunol. 2008;8:247–258. doi: 10.1038/nri2274. [DOI] [PubMed] [Google Scholar]
- 59.Thimme R, Bukh J, Spangenberg HC, Wieland S, Pemberton J, Steiger C, Govindarajan S, Purcell RH, Chisari FV. Viral and immunological determinants of hepatitis C virus clearance, persistence, and disease. Proc. Natl. Acad. Sci. U. S. A. 2002;99:15661–15668. doi: 10.1073/pnas.202608299. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.He XS, Rehermann B, Lopez-Labrador FX, Boisvert J, Cheung R, Mumm J, Wedemeyer H, Berenguer M, Wright TL, Davis MM, Greenberg HB. Quantitative analysis of hepatitis C virus-specific CD8(+) T cells in peripheral blood and liver using peptide-MHC tetramers. Proc. Natl. Acad. Sci. USA. 1999;96:5692–5697. doi: 10.1073/pnas.96.10.5692. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Neumann-Haefelin C, McKiernan S, Ward S, Viazov S, Spangenberg HC, Killinger T, Baumert TF, Nazarova N, Sheridan I, Pybus O, von Weizsacker F, Roggendorf M, Kelleher D, Klenerman P, Blum HE, Thimme R. Dominant influence of an HLA-B27 restricted CD8+ T cell response in mediating HCV clearance and evolution. Hepatology. 2006;43:563–572. doi: 10.1002/hep.21049. [DOI] [PubMed] [Google Scholar]
- 62.Schulze zur WJ, Ciuffreda D, Lewis-Ximenez L, Kasprowicz V, Nolan BE, Streeck H, Aneja J, Reyor LL, Allen TM, Lohse AW, McGovern B, Chung RT, Kwok WW, Kim AY, Lauer GM. Broadly directed virus-specific CD4+ T cell responses are primed during acute hepatitis C infection, but rapidly disappear from human blood with viral persistence. J. Exp. Med. 2012 doi: 10.1084/jem.20100388. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.