

Abstract
This Classic Article is a reprint of the original work by G. Bennett, Shoulder and Elbow Lesions Distinctive of Baseball Players. An accompanying biographical sketch of G. Bennett is available at DOI 10.1007/s11999-012-2334-3. The Classic Article is ©1947 and is reprinted with permission from Wolters Kluwer Health from Bennett G. Shoulder and elbow lesions distinctive of baseball players. Ann Surg. 1947;126:107–110.
In a former publication [1] I stressed the point that the professional baseball player was a human being, not a superman, and that he was susceptible to all of the common lesions of the shoulder which we see in the nonball player, namely, subacromion and subdeltoid bursitis, irritation of the supraspinatus and biceps tendons, traumatic synovitis and inflammatory disease. Fortunately, these conditions form the largest group and respond well to rest, heat and general orthodox treatment. Because a man is a ball player does not mean that he cannot have abscessed teeth, infected tonsils, or other foci of infection; therefore, his general health should be thoroughly investigated, just as one does when in search of some obscure etiologic factor in joint lesions.
His occupation is such, however, that aside from these common joint complaints he develops distinctive lesions. One which has been definitely identified and, to my knowledge, is nonexistent in other occupations, is a deposit on the posterior and inferior margin of the glenoid fossa, on or about the attachment of the triceps tendon. This is the result of the abnormal strain which is placed on the shoulder in throwing a baseball. As the arm swings forward in a flail-like movement with complete relaxation of the muscles of the shoulder, which is so essential for a pitcher to be effective, a tremendous strain is thrown upon the posterior shoulder and, as a result, deposits or exostoses develop in close proximity to the circumflex nerve and this nerve becomes irritated and causes marked referred pain to the shoulder joint, particularly in the region of the deltoid muscle. This is one of the distinctive lesions which very often ends the career of a professional pitcher as, in my opinion, it does not respond well to surgery. The cause is abnormal use of the shoulder and the deposits cause no discomfort or inconvenience except when throwing a baseball hard (Figs. 1, 2).
Fig. 1A–B.
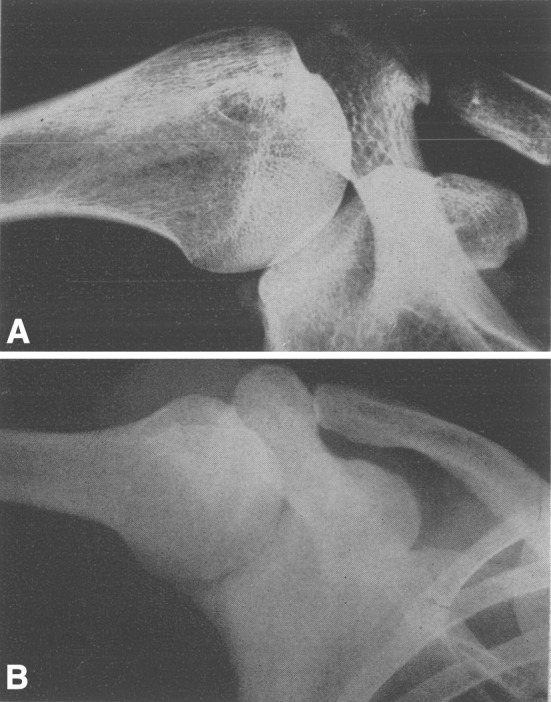
Characteristic deposits on the posterior-inferior border of the glenoid.
Fig. 2A–B.
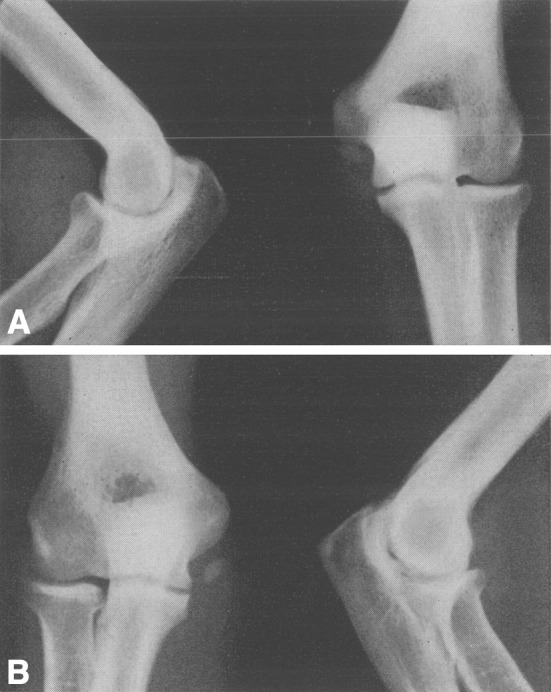
Typical small osseous growth in the ligamentous tissue posterior and inferior to the internal epicondyle.
The second lesion is a fraying of the supraspinatus tendon, which I do not think we can class as distinctive, because one sees it in individuals engaged in other occupations. The constant snubbing of the supraspinatus tendon over the head of the humerus and the greater tuberosity results in a gradual fraying of the deeper structures of the supraspinatus tendon. This is usually a lesion of a veteran pitcher after many years of professional baseball. On exploring these shoulders the outer surface of the supraspinatus tendon looks perfectly normal but a linear incision in the fibers of the tendon will show fraying of that portion which is in contact with the humerus. Again, I do not think this is a remedial lesion. It is the result of prolonged use and abnormal irritation and does not respond to surgery. It also is a condition which causes no discomfort except when throwing a baseball hard (Fig. 3).
Fig. 3.

The exostosis or deposit in the posterior inferior region of the glenoid cannot be identified by the ordinary anterior posterior or posterior anterior view of the shoulder. Our x-ray technician, Mr. W. Ross Mitchell, developed the technic shown here. External rotation of the humerus with tilting of the x-ray tube about 5 degrees is the position which rotates the head of the humerus and the glenoid to a position which throws the thickened area in relief (J. A. M. A., 117: 510–514, 1941).
The common pathologic processes of the elbow joint in the professional ball player are strikingly similar to those seen in non-ball players—loose bodies, single or multiple, either in the olecranon fossa, about the head of the radius or about the coronoid process. Generalized osteo-arthritis is also seen in non-ball players. There are, however, two lesions of the elbow which I think are distinctive. A pitcher in throwing a curve ball is compelled to supinate his wrist with a snap at the end of his delivery. This movement plus extension leads to the development of an irritation in front of the internal condyle of the humerus which is extremely disabling and very often ends his career. On examination one will note distinct fullness over the pronator radii teres, beneath which are the tendinous attachments of the brachialis and the flexor sublimis digitorum. These are covered by a very strong fascial band, a portion of which is the attachment of the biceps, which runs obliquely across the pronator muscle. A pitcher may be able to pitch for two or three innings when the pain and swelling becomes so great that he has to retire. Roentgenograms in the majority of cases are entirely negative, and on exploration the joint reveals very little. The muscle tissue generally is normal in appearance. The simple division of the fascia covering the muscles has, on occasions, rehabilitated these men so that they were able to return to the game. I am at a loss to explain it except that tension develops from some unidentified irritation to the muscle tissue which at times has an ischemic appearance. It is quite possible that this may be a secondary irritation which is the result of lipping of the ulna at its articulation with the internal condyle, because on rare occasions we see osteophytic processes here which are linked with the condition which I am endeavoring to describe. I am not clear in my own mind as to its exact pathology. I trust that further study and observation will clear up this point because I feel that it should be a remediable lesion.
The most distinctive lesion, and one which is not seen in other occupations, is the development of single or multiple deposits of bone or ossicles in the ligamentous tissue and tendinous attachments beneath the ulnar nerve and not within the joint. I am quite sure that these deposits are purely the result of chronic strain and probably take years to develop, and in many instances give no symptoms. When they begin to cause irritation of the ulnar nerve they can be removed with success. Identifying these small masses of bone in the ligamentous tissue and dissecting them free will relieve symptoms in most cases.
Footnotes
Read before the 58th Annual Session of the Southern Surgical Association, Hot Springs, Va., December 11, 1946.
Richard A. Brand MD (✉) Clinical Orthopaedics and Related Research, 1600 Spruce Street, Philadelphia, PA 19103, USA e-mail: dick.brand@clinorthop.org
Reference
- 1.Bennett, George E.: Shoulder and Elbow Lesions of the Professional Baseball Pitcher. J. A. M. A., 117, 510, August 1, 1941.