

Abstract
Purpose
Non-invasive ventilation is largely used to treat acute and chronic respiratory failure. This ventilation encounters a non negligible rate of failure related to the used interface/mask, but the reasons for this failure remain unclear. In order to shed light into this issue and to better understand the effects of the geometrical design of interfaces, we aimed to quantify flow, pressure and gas composition in terms of CO2 and O2 at the passage through different types of interface (oronasal mask, integral mask and helmet). Especially, we postulated that due to specific gas flow passing throughout interface, the effective dead space added by the interface is not always related to the whole gas volume included in the interface.
Methods
Numerical simulations, using computational fluid dynamics, were used to describe pressure, flow and gas composition during ventilation with the different interfaces.
Results
Between the different interfaces the effective dead spaces differed only modestly (110 to 370ml) while their internal volumes were markedly different (110 to 10000ml). It was limited to half the tidal volume for the most voluminous interface, while it was close to the interface gas volume for the less voluminous interfaces. Pressure variations induced by the flow ventilation throughout the interface were negligible.
Conclusions
Effective dead space is not related to the internal gas volume included in the interface, suggesting that this internal volume should not be considered as a limiting factor for their efficacy during non-invasive ventilation. Patient’s comfort and synchrony have also to be taken into account.
Keywords: Computer Simulation, Equipment Design, Face, anatomy & histology, Humans, Positive-Pressure Respiration, instrumentation, Respiratory Dead Space
Keywords: interfaces/masks, non-invasive ventilation, dead space
INTRODUCTION
Non-invasive ventilation (NIV) defines a method of mechanical ventilation that does not require endotracheal intubation. Using this technique, pressurized gas is delivered to the airways through one of a variety of interfaces, such as a mouthpiece or a nasal or facial mask. Over the last two decades, the use of NIV has increased markedly in the treatment of both acute and chronic respiratory failure [1, 2]. In an acute setting, NIV reduces the risk of endotracheal intubation [3] and facilitates the weaning process from mechanical ventilation [4]. Nevertheless for various reasons, NIV is not always successful. The rate of failure for this procedure in acute patients ranges from 7% to 49% [2, 5–7]. One of the reasons reported in the literature to explain this failure rate is the poor patient tolerance to the NIV interface [8, 9]. Mask discomfort, sensation of excessive air pressure, intolerance, skin lesions, leakage and rebreathing have been cited as the most relevant parameters to explain the interface-related failure of NIV. A large variety of interfaces are presently available ranging from the simple nasal or oronasal mask to the helmet recently proposed [17, 18]. To our knowledge, the efficacy of these different interfaces has essentially been tested in clinical trials or in bench studies based upon the comparison of clinical indexes such as breathing pattern, airway pressure, neuromuscular drive, inspiratory muscle effort, work of breathing (WOB), arterial blood gases and dyspnea [1, 9–16]. All these interfaces allow successful non-invasive ventilation. Especially, clinical efficacy was not found different during NIV conducted with interfaces whose volumes very much differed [1, 9, 10, 16]. Only WOB and inspiratory muscle effort were slightly less decreased with the helmet, by comparison to the other interfaces [10, 16] but these differences were abolished by a specific ventilator setting [16]. In first view, this fact is surprising since some of these interfaces have a large internal volume associated with dead space that should not permit successful ventilation. In theory, the dead space should remain as small as possible because any increase of it, induces a raise in patient’s WOB [19].
We presently postulate that due to the streaming effects of the gas passing throughout the interface, the effective dead space of the interface could be quite different from the volume delimited by the interface and the part of the body embedded in this interface (called interface gas region). To test this assumption, we used numerical simulations with computational fluid dynamic (CFD) software to describe pressure, flow and gas composition in four types of interfaces regularly used to deliver NIV in the intensive care unit (ICU). In contrast with clinical trials, CFD presents the advantage to test this set of interfaces in strictly identical conditions. In a previous in vitro bench study, Saatci and al.[20] estimated the interface dead space without flow or pressure measurements. However, these authors tested several face masks but not the helmet interface.
MATERIAL AND METHOD
We studied four interfaces commonly used in ICU (see Table 1 for interface characteristics): two oronasal face masks (masks #1 and #2), an integral mask (mask # 3) and a helmet-type interface which covers the entire head and neck (mask # 4). Each interface was successively positioned upon the same adult mannequin head made of polystyrene. Each setup, i.e., the mannequin-interface, was numerically reconstructed in three dimensions by using computed tomography (CT) images. In each three dimensional (3D) geometry, breathing flow was simulated for successive cycles (i.e. inspiratory + expiratory phases) by using CFD software (FLUENT® Fluent Inc., Lebanon, TN, USA) until an “equilibrium state” was reached. The equilibrium state is defined as the moment where the parameters (i.e., pressure, flow and gas composition) become identical from one breathing cycle to the next breathing cycle. Details about 3D reconstruction and CFD procedure are described in the online electronic supplementary material (ESM). The inspiratory phase consisted of blowing a constant 600 ml/sec flow rate during 1.25 sec through the inlet of the interface. The expiratory phase consisted of blowing a constant 300 ml/sec flow rate during 2.5 sec through the mouth of the mannequin. This setting corresponds to a breathing pattern of 750 ml tidal volume (VT), 16 beats/min frequency and a ratio of 2 between inspiratory and expiratory times. During the inspiratory phase, the insufflated gas called “fresh air” was normal air, fully humidified and heated at 37°C (Figure 1). During the expiratory phase, the gas blown in the interface, called in Figure 1 “exhaled air”, was air enriched with CO2 (see Table 2 for the exact compositions of fresh air and exhaled air). At the initial time of the first breathing cycle, the interface gas region was totally filled with fresh air. The CFD procedure allows estimating gas composition, flow and pressure at any locus of the interface gas region and at any time of the breathing cycle. Gas composition was described as the mass fraction of each gas species, especially for oxygen (MFO2) and carbon dioxide (MFCO2). Then, we determined the effective dead space (VD) of the interface gas region defined as the rebreathed gas volume resulting from the exhaled gas trapped in this interface gas region as well as the volume of fresh air (Vfresh) that are inhaled by the mannequin during each inspiratory cycle
Table 1.
Non invasive ventilation interfaces
| Mask | Name/Compagny | Mask type | Interface volume (ml) |
|---|---|---|---|
| # 1 | Airvie/Peters | oronasal | 111 |
| # 2 | Full Face/Koo | oronasal | 205 |
| # 3 | Inspir’aid/Fernez-Bacou | integral mask | 978 |
| # 4 | Castor-R/Starmed | helmet | 10220 |
Non invasive ventilation interfaces. The interface volume is the internal volume of each interface estimated in presence of the mannequin head.
Figure 1.
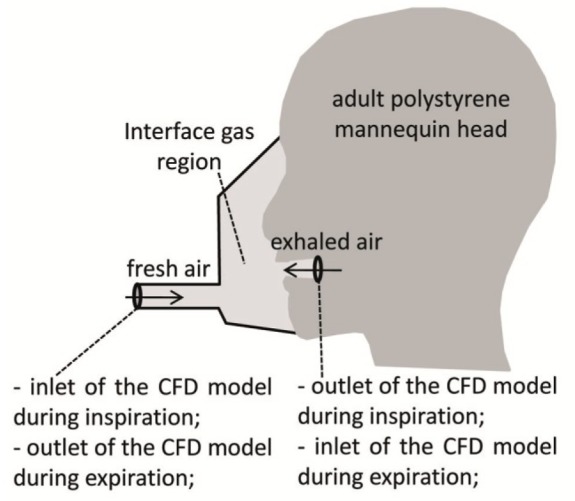
Schematic of the set-up showing the interface positioned on the polystyrene mannequin head.
CFD: Computational fluid dynamics
Table 2.
Gas compositions
| N2 | O2 | Ar | CO2 | H2O | ||
|---|---|---|---|---|---|---|
| Inspiratory flow (fresh air) | Mass Fraction (%) | 72.5 | 22.2 | 1.2 | 0.0 | 3.9 |
| Volume Fraction (%) | 73.3 | 19.7 | 0.9 | 0.0 | 6.2 | |
| Expiratory flow (exhaled air) | Mass Fraction (%) | 71.1 | 16.6 | 1.2 | 7.2 | 3.9 |
| Volume Fraction (%) | 73.3 | 15.0 | 0.9 | 4.7 | 6.2 |
The pressure in the interface is composed by a mean pressure (e.g. atmospheric pressure, pressure support, positive end-expiratory pressure) and by the variation of pressure induced by the flow. This variation of pressure, which is computed by the CFD procedure, does not depend on the mean pressure as long as the thermodynamical properties of gas are not affected by the mean pressure. Therefore, our results theoretically apply to the different pressure regimes or ventilator settings, constant or intermittent, used in clinical practice during NIV.
RESULTS
The equilibrium state was estimated from the time course of MFO2 at the mouth from one cycle to the following cycle. For the first 3 interfaces shown in Table 1, the equilibrium state was quickly reached: the MFO2 curves become identical after less than 6 breathing cycles. To reach the equilibrium state with the helmet took a little more time: approximately 2 minutes (i.e., after 32 breathing cycles).
During the inspiratory phase, MFO2 at the mouth of the mannequin globally increases with time, while MFCO2 decreases (see Figure 2). MFO2 represents the quantity of oxygen available for the lung at the equilibrium state while MFCO2 quantifies the amount of CO2 rebreathing. With the two oronasal masks (#1 and #2), that are the smaller, the MFO2 tended to reach the maximum theoretical value (22.2%, i.e., the oxygen concentration of the total fresh air) by the end of the inspiration time. By contrast, with the two other interfaces (#3 integral and #4 helmet), MFO2 at the mouth of the mannequin was never above 20% during the inspiratory cycle. The MFCO2 behaviour was to decrease throughout the inspiratory phase from its maximum value (7.2%) to zero (0%) for the two oronasal masks, and to remain always positive for the two other masks: 2.4% for integral mask and 3.2% for helmet, (see Figure 2).
Figure 2.

Evolution of the Mean Mass Fraction of Oxygen (MFO2 on left vertical axis) and Carbon dioxide (MFCO2 on right vertical axis) at the mouth of the mannequin during the inspiratory period once the equilibrium state is reached between two successive cycles (see text). The inspiration begins at time (t= 0) and stops at time (t = 1.25 sec). Dashed lines indicate the mass fractions of fresh and exhaled air.
The effective dead space characterizing the four interfaces varied from 110 ml to 370 ml (see Figure 3). The larger VD corresponds to the helmet, and represents only 4% of the volume of the interface gas region. In this case, the effective dead space increases linearly with time and inspired volume (see Figure 4). The smallest VD was obtained with the oronasal mask #1 which has the smallest interface gas volume, and the VD was about 100% of the interface gas volume (see Figure 3). For this oronasal mask #1, VD was attained within the first 0.35 sec of the inspiratory cycle, before following a plateau during the remaining of the cycle (see Figure 4). The two others masks i.e., oronasal mask #2 and integral mask, behaved intermediately. The VD profile (see Figure 3) of oronasal mask # 2 during the inspiration was close to that of oronasal mask # 1, with a VD reaching 93% of the interface gas volume. The integral mask behaviour was not far from that of helmet, with a VD equal to only 35% of the interface gas volume (see Figure 3).
Figure 3.
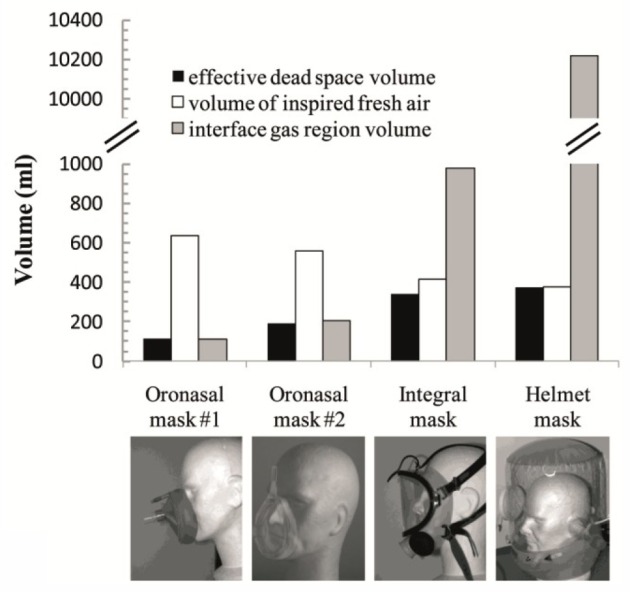
Effective dead space volume, volume of inspired fresh air and interface gas volume for the four masks presented in Table 1. These data are given once the equilibrium state is reached between two successive cycles.
Figure 4.
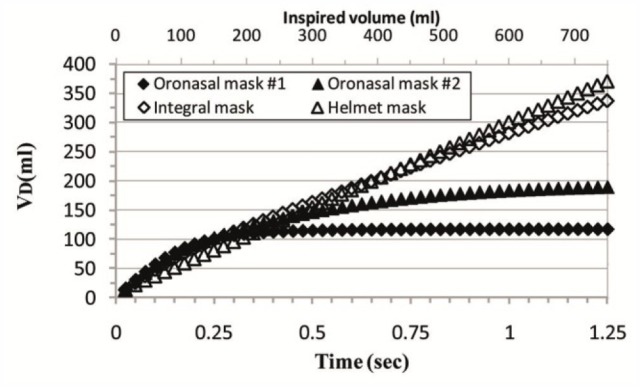
Evolution of the effective dead space volume during the inspiratory period once the equilibrium state is reached between two successive cycles. The inspiratory flow begins at time (t= 0) and stops at time (t= 1.25 sec).
For all tested interfaces, the pressure field was found relatively homogeneous with a maximum pressure variation not exceeding 0.3 cm H2O.
DISCUSSION
The main finding of this study is that the effective dead space, which is never higher than the interface gas volume, can be much smaller due to the streaming effect presently calculated by CFD. For all the interfaces the effective dead space was under 370 ml for a tidal volume of 750 ml. This is of clinical interest because it suggests that even interfaces with extremely high internal volumes (10 liters) might yet be used in patients. This holds true to the extent that patients are capable to inhale an inspired gas slightly enriched with CO2 (a maximum 2.1% of CO2 in volume for the helmet). The finding that effective interface dead space is not linked to the interface gas volume is consistent with several clinical studies. These studies have reported a lack of differences, in terms of patient’s respiratory effort, breathing pattern and gas exchange, among interfaces with disparate internal volumes [1, 9, 14, 16, 21, 22].
Importantly, our results also show that with a tidal volume of 750 ml, the less voluminous mask (oronasal mask #1) clearly remains the most favorable in terms of re-breathing, since the VD is reduced by a factor of 3.4 when compared to the VD of the most voluminous masks (helmet) (Figure 3). Nevertheless, this beneficial effect decreases quasi linearly as tidal volume decreases (Figure 4). For example, with a tidal volume of 400 ml, the previous factor is as low as 1.8. This means that the choice of an interface based only on the effective VD, is probably questionable. Factors such as comfort, tolerance and leaks should also be taken into account during the decision-making process.
In the extreme case of tidal volumes below 200 ml, the most efficient interface in terms of re-breathing becomes the most voluminous (the helmet). Of course, such a small tidal volume does not fit standard adult ventilation. However, if we consider the non-invasive high-frequency oscillatory ventilation at low tidal volume, as recently proposed in neonatalogy [23], our results suggest that a helmet interface could be potentially more effective than a nasal or oronasal interface due to the lower CO2 rebreathing. It is not in disagreement with the fact that the helmet is not the interface of choice for NIV in COPD patients with acute exacerbation. Indeed, a 200 ml tidal volume is too low in breathing adult COPD patients to results in adequate alveolar ventilation. With these patients the required tidal volume is higher, i.e., in range where the helmet is the less efficient interface in terms of re-breathing.
The streaming effect behind effective dead space can be physically understood on the basis of the ratio between tidal volume and interface gas volume. When the interface gas volume is much larger than the tidal volume, the convective flows are reduced and the gas composition in the interface, i.e., the mass fraction of each gas species, is poorly affected by a single breathing cycle. The quasi-constancy of MFO2 and MFCO2 at the mouth in the helmet mask throughout the entire inspiratory phase illustrates this phenomenon (Figure 2). This assumption was already implicitly developed by Taccone et al. [15] who described the helmet functions as a semi-closed environment. Accordingly, the corresponding mass fraction becomes, at the equilibrium point, the mean between the mass fractions of fresh air and exhaled air and the VD is half the tidal volume, (e.g., VD = 49% of VT in the helmet). On the basis of a negligible convective flow it suggests that this result (VD ≅ 50% of VT) may be generalized to the other helmets.
By contrast, when the interface volume is small as compared to the tidal volume (oronasal mask #1 and #2), the convective flows are important. In this scenario, the recirculation velocities are relatively high and are also present in the quasi-totality of the interface gas region. In this case, the interface gas volume is washed out by the breathing flow (i.e., both the inhaled and the exhaled gas) and the dead space gets closer to the interface internal volume, (e.g., 100 % of the interface gas volume for the oronasal mask # 1 and 93 % for the oronasal mask #2). On this basis, we can predict that the “small” masks (oronasal) have a VD close to their internal volume.
With the integral mask, where the gas entry is at the level of the chin, the role of convection is intermediate and the tidal volume is close to the interface gas volume. In the first part of an inspiration, (i.e., for the first 0.35 sec, corresponding to about 200 ml of inspired gas), the inferior part of the mask (from the chin to the mouth) is rapidly washed out. During this time, MFO2 and VD are close to the values observed with the 2 smallest masks (see oronasal masks #1 and #2 in Figure 2 and 4). After this short period of time, MFO2 at the mouth reaches a plateau resulting from gas mixture made of the gas flow coming directly from the ventilator (fresh air) and partial entrainment of the gas residing between the mouth and forehead (see the video showing the time course of the MFO2 during the inspiration and expiration in the online ESM). The fact, that VD is impacted by both convective and diffusive phenomena, suggests that the results of our simulation cannot be generalized to the other integral mask to predict the VD. Changing geometry may change the balance between convective and diffusion phenomena that will result in a different VD.
Noteworthy, the physical streaming effects do not require important pressure variations in the interface gas region. It confirms that these interfaces are slightly resistive and are not responsible for a significant amount of resistive work. Chiumello et al. [10] found that helmet induced an increase of WOB associated with an increase of the time to reach the pressure support without any increase of the tidal volume while Vargas et al. [16] found that using a specific settings (increase of the pressure support and PEEP with the highest pressurization rate) allowed to abolish this greater inspiratory muscle effort. It suggests that this increased WOB observed with the helmet is explained in part by trigger and pressurization difficulties and not only to a large dead space problem. Such assumption is in agreement with the relative low value of VD that we obtained.
The present findings can be partially extended to clinically-relevant changes in oxygen and carbon dioxide concentrations. In this study we used normal air, heated and humidified, as inspiratory gas and we used air enriched with 5% of CO2 as the expired gas. Oxygen-therapy as well as O2 - CO2 exchange within the lung modify gas composition. As long as physical and thermodynamic properties of the gas are not affected by gas composition and/or temperature, the effective dead space inferred in this study remains unchanged. This means that if convective and diffusive phenomena are unchanged, the effective dead space is also unchanged. Considering the slight modification in thermodynamic properties of the gas (less than 10% for gas density and less than 4% for gas kinematic viscosity) induced by either a variation of O2 concentration (from 15% to 100%) or a variation of CO2 concentration (from 0 to 5%), we can postulate that our results remain valid whatever the oxygen-therapy level administered. Note that, a change in O2 concentration in the fresh air only requires changing the maximal and minimal values corresponding to fresh and exhaled air, in the scales of Figure 2.
One of the limitations of this study was that the numerical tool did not allow us to simulate non-intentional leak. Nevertheless, it is clear that a bias-flow leak tends to decrease the rebreathing problem, but it also tends to induce auto-triggering and to decrease the effective tidal volume inspired by the patient [24, 25]. However, the importance of these phenomena is extremely contingent upon a set of conditions as ventilator mode, trigger algorithms or maximum flow deliverable by the ventilator. Another limitation of this study is that we implicitly assumed the rigidity of the wall interface. This assumption is particularly questionable with the helmet. However, a recent study [16] concluded that increasing both pressure-support level and positive end-expiratory pressure may be clinically advisable when providing NIV via a helmet. Such a higher pressurization, that reduces the compliance of the helmet, tends to justify our rigidity assumption.
In summary, we have shown that mathematical modelling and computational fluid dynamics can estimate the effective dead space of NIV interfaces by analysing the pressure field/flow pattern and variations in gas composition inside these interfaces. New research efforts will be dedicated in the future to the translation of these mathematical modelling to clinical environments so as to increase efficiency while decreasing the side-effects of the clinical treatments. The effective dead space of the interfaces used for NIV was not directly related to the internal volume of the interface. For the most voluminous interfaces, effective dead space is limited to half the tidal volume while the effective dead space is close to the interface gas volume only for the less voluminous interfaces. These findings allow physicians to choose among a large number of masks which may be suitable for an individual patient and also allow physicians to take into consideration other parameters such as comfort and synchrony when choosing an interface.
Supplementary Material
References
- 1.Tarabini Fraticelli A, Lellouche F, L’Her E, Taille S, Mancebo J, Brochard L. Physiological effects of different interfaces during noninvasive ventilation for acute respiratory failure. Crit Care Med. 2009;37:939–945. doi: 10.1097/CCM.0b013e31819b575f. [DOI] [PubMed] [Google Scholar]
- 2.Mehta S, Hill NS. Noninvasive ventilation. Am J Respir Crit Care Med. 2001;163:540–577. doi: 10.1164/ajrccm.163.2.9906116. [DOI] [PubMed] [Google Scholar]
- 3.Brochard L, Mancebo J, Wysocki M, Lofaso F, Conti G, Rauss A, Simonneau G, Benito S, Gasparetto A, Lemaire F, et al. Noninvasive ventilation for acute exacerbations of chronic obstructive pulmonary disease. N Engl J Med. 1995;333:817–822. doi: 10.1056/NEJM199509283331301. [DOI] [PubMed] [Google Scholar]
- 4.Nava S, Ambrosino N, Clini E, Prato M, Orlando G, Vitacca M, Brigada P, Fracchia C, Rubini F. Noninvasive mechanical ventilation in the weaning of patients with respiratory failure due to chronic obstructive pulmonary disease. A randomized, controlled trial. Ann Intern Med. 1998;128:721–728. doi: 10.7326/0003-4819-128-9-199805010-00004. [DOI] [PubMed] [Google Scholar]
- 5.Carlucci A, Richard JC, Wysocki M, Lepage E, Brochard L. Noninvasive versus conventional mechanical ventilation. An epidemiologic survey. Am J Respir Crit Care Med. 2001;163:874–880. doi: 10.1164/ajrccm.163.4.2006027. [DOI] [PubMed] [Google Scholar]
- 6.Girault C, Briel A, Hellot MF, Tamion F, Woinet D, Leroy J, Bonmarchand G. Noninvasive mechanical ventilation in clinical practice: a 2-year experience in a medical intensive care unit. Crit Care Med. 2003;31:552–559. doi: 10.1097/01.CCM.0000050288.49328.F0. [DOI] [PubMed] [Google Scholar]
- 7.Robino C, Faisy C, Diehl JL, Rezgui N, Labrousse J, Guerot E. Effectiveness of non-invasive positive pressure ventilation differs between decompensated chronic restrictive and obstructive pulmonary disease patients. Intensive Care Med. 2003;29:603–610. doi: 10.1007/s00134-003-1654-x. [DOI] [PubMed] [Google Scholar]
- 8.Chiumello D. Is the helmet different than the face mask in delivering noninvasive ventilation? Chest. 2006;129:1402–1403. doi: 10.1378/chest.129.6.1402. [DOI] [PubMed] [Google Scholar]
- 9.Cuvelier A, Pujol W, Pramil S, Molano LC, Viacroze C, Muir JF. Cephalic versus oronasal mask for noninvasive ventilation in acute hypercapnic respiratory failure. Intensive Care Med. 2009;35:519–526. doi: 10.1007/s00134-008-1327-x. [DOI] [PubMed] [Google Scholar]
- 10.Chiumello D, Pelosi P, Carlesso E, Severgnini P, Aspesi M, Gamberoni C, Antonelli M, Conti G, Chiaranda M, Gattinoni L. Noninvasive positive pressure ventilation delivered by helmet vs. standard face mask. Intensive Care Med. 2003;29:1671–1679. doi: 10.1007/s00134-003-1825-9. [DOI] [PubMed] [Google Scholar]
- 11.Mortimore IL, Whittle AT, Douglas NJ. Comparison of nose and face mask CPAP therapy for sleep apnoea. Thorax. 1998;53:290–292. doi: 10.1136/thx.53.4.290. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Navalesi P, Fanfulla F, Frigerio P, Gregoretti C, Nava S. Physiologic evaluation of noninvasive mechanical ventilation delivered with three types of masks in patients with chronic hypercapnic respiratory failure. Crit Care Med. 2000;28:1785–1790. doi: 10.1097/00003246-200006000-00015. [DOI] [PubMed] [Google Scholar]
- 13.Pelosi P, Severgnini P, Aspesi M, Gamberoni C, Chiumello D, Fachinetti C, Introzzi L, Antonelli M, Chiaranda M. Non-invasive ventilation delivered by conventional interfaces and helmet in the emergency department. Eur J Emerg Med. 2003;10:79–86. doi: 10.1097/00063110-200306000-00002. [DOI] [PubMed] [Google Scholar]
- 14.Racca F, Appendini L, Gregoretti C, Stra E, Patessio A, Donner CF, Ranieri VM. Effectiveness of Mask and Helmet Interfaces to Deliver Noninvasive Ventilation in a Human Model of Resistive Breathing. J Appl Physiol. 2005 doi: 10.1152/japplphysiol.01363.2004. [DOI] [PubMed] [Google Scholar]
- 15.Taccone P, Hess D, Caironi P, Bigatello LM. Continuous positive airway pressure delivered with a “helmet”: effects on carbon dioxide rebreathing. Crit Care Med. 2004;32:2090–2096. doi: 10.1097/01.ccm.0000142577.63316.c0. [DOI] [PubMed] [Google Scholar]
- 16.Vargas F, Thille A, Lyazidi A, Campo FR, Brochard L. Helmet with specific settings versus facemask for noninvasive ventilation. Crit Care Med. 2009;37:1921–1928. doi: 10.1097/CCM.0b013e31819fff93. [DOI] [PubMed] [Google Scholar]
- 17.Antonelli M, Conti G, Pelosi P, Gregoretti C, Pennisi MA, Costa R, Severgnini P, Chiaranda M, Proietti R. New treatment of acute hypoxemic respiratory failure: noninvasive pressure support ventilation delivered by helmet--a pilot controlled trial. Crit Care Med. 2002;30:602–608. doi: 10.1097/00003246-200203000-00019. [DOI] [PubMed] [Google Scholar]
- 18.Bellani G, Patroniti N, Greco M, Foti G, Pesenti A. The use of helmets to deliver non-invasive continuous positive airway pressure in hypoxemic acute respiratory failure. Minerva Anestesiol. 2008;74:651–656. [PubMed] [Google Scholar]
- 19.Lellouche F, Maggiore SM, Deye N, Taille S, Pigeot J, Harf A, Brochard L. Effect of the humidification device on the work of breathing during noninvasive ventilation. Intensive Care Med. 2002;28:1582–1589. doi: 10.1007/s00134-002-1518-9. [DOI] [PubMed] [Google Scholar]
- 20.Saatci E, Miller DM, Stell IM, Lee KC, Moxham J. Dynamic dead space in face masks used with noninvasive ventilators: a lung model study. Eur Respir J. 2004;23:129–135. doi: 10.1183/09031936.03.00039503. [DOI] [PubMed] [Google Scholar]
- 21.Anton A, Tarrega J, Giner J, Guell R, Sanchis J. Acute physiologic effects of nasal and full-face masks during noninvasive positive-pressure ventilation in patients with acute exacerbations of chronic obstructive pulmonary disease. Respir Care. 2003;48:922–925. [PubMed] [Google Scholar]
- 22.Gregoretti C, Confalonieri M, Navalesi P, Squadrone V, Frigerio P, Beltrame F, Carbone G, Conti G, Gamna F, Nava S, Calderini E, Skrobik Y, Antonelli M. Evaluation of patient skin breakdown and comfort with a new face mask for non-invasive ventilation: a multi-center study. Intensive Care Med. 2002;28:278–284. doi: 10.1007/s00134-002-1208-7. [DOI] [PubMed] [Google Scholar]
- 23.Colaizy TT, Younis UM, Bell EF, Klein JM. Nasal high-frequency ventilation for premature infants. Acta Paediatr. 2008;97:1518–1522. doi: 10.1111/j.1651-2227.2008.00900.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Fauroux B, Leroux K, Desmarais G, Isabey D, Clement A, Lofaso F, Louis B. Performance of ventilators for noninvasive positive-pressure ventilation in children. Eur Respir J. 2008;31:1300–1307. doi: 10.1183/09031936.00144807. [DOI] [PubMed] [Google Scholar]
- 25.Louis B, Leroux K, Isabey D, Fauroux B, Lofaso F. Effect of manufacturers inserted mask leaks on ventilator performance. Eur Respir J. 2009;35:627–636. doi: 10.1183/09031936.00188708. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.