

Abstract
The aim of the present roentgenographic in vitro study was to determine the initial straight length from the cemento-enamel junction (CEJ) to the appearance of a root canal curvature in human mandibular premolars. A total number of 282 mandibular premolars were examined. Exclusion criteria comprised root caries, extensive restorations and endodontically treated teeth. The teeth were fixed and digitally radiographed by means of a specially developed fixation device with standardized and reproducible distances with the parallel technique (Heliodent MD; Merlin 2.1). The distances from the CEJ to the first curvature (> 5°) (distance I), from the first curvature to a second curvature (distance II), and from the first or second curvature to the radiological apex (distance III) were recorded. The lengths of the initial straight distance and the appearance of a curvature were statistically analyzed and related to each other. In first mandibular premolars, the mean value for distance I was 10.9 mm, for distance II 3.7 mm and for distance III 3.04 mm. The mean values for the second mandibular premolars were 1.1 mm in distance I, 4.3 mm in distance II and 3.1 mm in distance III. No statistically significant differences between left and right mandibular premolars could be observed regarding the canal curvature location and the angle values. The results of this investigation show that curvatures are increasingly observed 9 to 12 mm from the original path in mandibular premolars.
Keywords: Mandibular premolars, root canal curvature, in vitro study
Introduction
Conventional endodontic treatment has experienced an impressive progression over the last decades basically through a more efficient desinfection of the root canal system supported by new irrigation and instrumentation methods combined with increasing information about morphological complexities [6,10,15]. The success of root canal therapy is dependent on a thorough knowledge of the root and root canal morphology in order to locate the root canals and properly clean, shape, and obturate the canal space in three dimensions, thus the study of root and canal anatomy has endodontic and anthropologic significance [7,8].
In fact it is important to be familiar with variations in tooth anatomy because such knowledge can aid in locating canals and their subsequent management. Techniques and recommendations for the restoration of endodontically treated teeth have developed from the use of rigid prefabricated metal posts to composite resins and fiber reinforced composite posts [17]. The use of fiber posts in combination with adhesive materials for definite restorations has also experienced a progressive development. Fiber posts together with composite cores as foundation materials for the restoration of endodontically treated teeth are widely accepted as a viable alternative to cast posts of 2/3 of the determined root canal length. When considering the anatomy of human teeth, the number of roots and root canal incidence varies greatly in the literature. Their morphology is quite variable and can be extremely complex [1,2,9,12,13]. However, studies that determine the frequency and localization of root canal curvatures in relation to the initial straight distance are extremely rare. When a post insertion becomes necessary the precise knowledge of the root canal morphology is fundamental in order to avoid root canal perforations. Hence, the aim of this clinical study was to develop a standardised radiographic investigation technique in order to determine the root canal morphology of mandibular premolars regarding length and curvatures of the canals to provide information for subsequent post insertion.
Material and methods
In this study recently extracted human mandibular premolars (n = 282) were used. The teeth were collected from the department of oral surgery and private dental center practices. There was no information about the patients age, gender and general health condition. Exclusion criteria for further detailed analysis were the following: teeth with a non-definable cemento-enamel-junction (CEJ) or apex, endodontically treated teeth, a non-definable clinical crown and/or root, teeth with root caries, crowns or extensive fillings and type II and type IV root canal configurations [20]. Mandibular premolars with two root canals were also excluded. A specially developed fixation device was employed in order to be able to reproduce the radiographic parameters [21]. The teeth were digitally radiographed (Heliodent MD, Sirona Benzheim, Germany/Merlin 2.1) in a bucco-lingual plane, with an exposure time of 0.2 sec (60 kV) and with the parallel technique. The reliability of the x-ray beam was controlled throughout the entire investigation by means of an aluminium key (Hounsfield-scale). Radiographs were taken horizontally and in 20° from the mesial and distal tooth axis aspects. A horizontal line between the mesial and distal CEJ served as the coronal reference level. The intersection point in the middle of the root canal was used as a reference for the straight lines and tangents. To achieve objective results and guarantee accuracy, the investigators were calibrated by experienced operators of the endodontic and radiological departments. All relevant distances, angles, tangents and reference level (CEJ) were determined by an experienced endodontist. The length of the straight distance between the CEJ to the first curvature was recorded. The corresponding angles (angle values more than 5 degree) were determined as the angle between distance I (CEJ to the first curvature) and distance II (first curvature to the possible second curvature or to the radiological apex) as well as between distance III (second curvature to the radiological apex).
The mean values of the measurements of ten pilot radiographs that were made with the parallel technique and horizontal projection were used as a reference when importing the images (JEPG-format) into Adobe Photoshop 7.0 (36 pixels = 1 mm and 1 pixel = 0.027 mm). The data were collected with Microsoft Excel 2003® and after transformation of data statistical analysis was performed with statistical package SPSS® (Version 14.0). For categorical characteristics frequency and relative frequency and for metrical characteristics mean, standard deviation and also median were calculated. The statistical significance between categorical item position (first vs. second; and separately also left vs. right side) and the number of curvatures was determined. Statistically significant differences between position and (separately also side) concerning total root canal length and median angle for the first curvature were determined with the Wilcoxon-Mann-Whitney test. The analyses of data was done in an explorative manner and the outcome of a statistic test with p-value < 0.05 is called significant.
Results
In the present investigation a total of 282 human mandibular premolars were examined. After considering exclusion criteria all first left premolars (n = 107) and first right premolars (n = 100) as well as all second left premolars (n = 32) and all second right premolars (n = 43) showed only one root canal. The values for the total root canal length of the first and second premolars (left and right side) are demonstrated in Figure 1. The mean value of distance I (CEJ to the first curvature) was for the first left premolar 10.9 mm and for the first right premolar 10.8 mm; for the second left premolar there was a mean value of 12.0 mm and for the second right premolar of 10.9 mm (Figure 2). The difference in mean length of distance I was significant for the first and second premolars (p < 0.001) but not for left and right side (p < 0.9). For the second straight distance (first curvature to the second curvature) following mean values could be found: first left premolar: 3.15 mm; first right premolar: 4.19 mm; second left premolar: 4.34 mm and second right premolar: 4.24 mm (Figure 3). The third distance (second curvature to the radiological apex) demonstrated mean values for the first left premolar of 3.22 mm, for the first right premolar mean value of 2.69 mm, for the second left premolar mean value of 4.32 mm and for the second right premolar mean value of 3.41 mm (Figure 4). The mean angle for the first curvature was for the first left premolar 18° and for the first right premolar 14°. For the second left premolar mean values of 19° and in the second right premolar values of 13° were recorded (Figure 5). The difference in mean angle for the first curvature was significant for first and second premolar (p < 0.001) but not for left and right side (p < 0.7). The corresponding angle II between the second and third straight distance showed mean values of 24.5° for the first left premolar, for the first right premolar a value of 20°, for the second left premolar a mean value of 12° and for the second right premolar of 21°. Second root canal curvatures could be found in a high percentage. The first left premolars showed two root canal curvatures in 24.2% of all cases, the first right premolars in 37.2%, the second left premolars in 4.5% and the second right premolars in 34.3%. When comparing the left and the right premolars (first and second premolars), no significant differences could be found with regard to all determined parameters; therefore the first premolars (left and right side) as well as the second premolars (left and right side) were added together. This resulted in a linear graph of the cumulative frequencies of root canal curvatures. The first as well as the second premolars showed sigmoid graphs. In both cases slight plateaus in the initial and final course could be observed. This evaluation demonstrates that root canal curvatures could be found in a high frequency from 9 to 12 mm of the initial root length (Figure 6 and 7).
Figure 1.
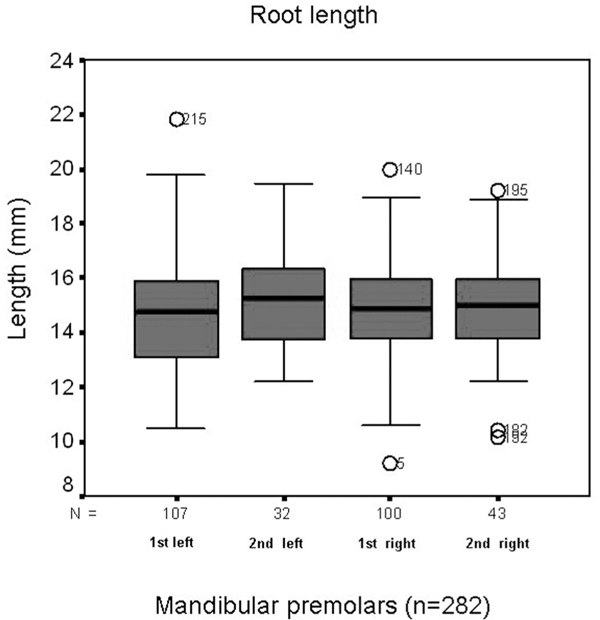
Total root canal length for the first and right mandibular premolars. The distances were recorded between the cemento-enamel junction and the radiological apex.
Figure 2.
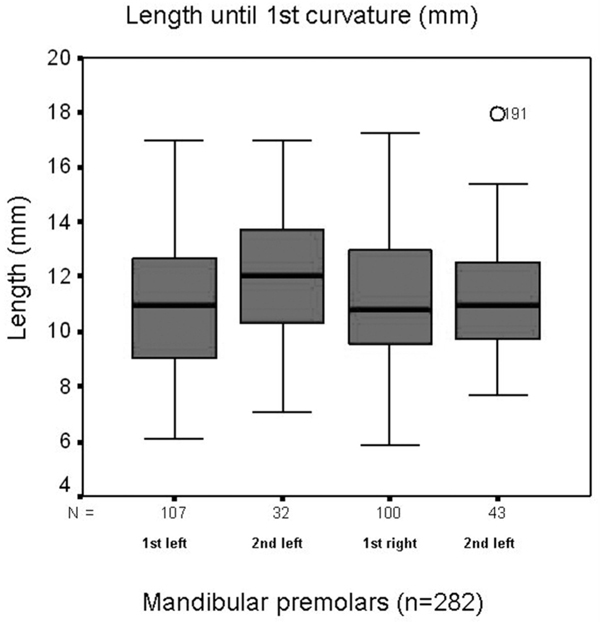
Measured length of the distance I (distance from the CEJ to the first curvature with values > 5°) for all mandibular premolars.
Figure 3.
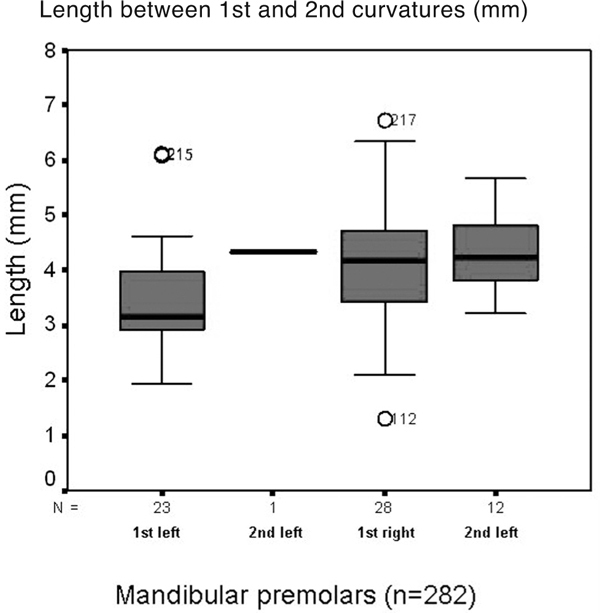
Measured length of the distance II between the first and a second curvature, if present in mandibular premolars.
Figure 4.
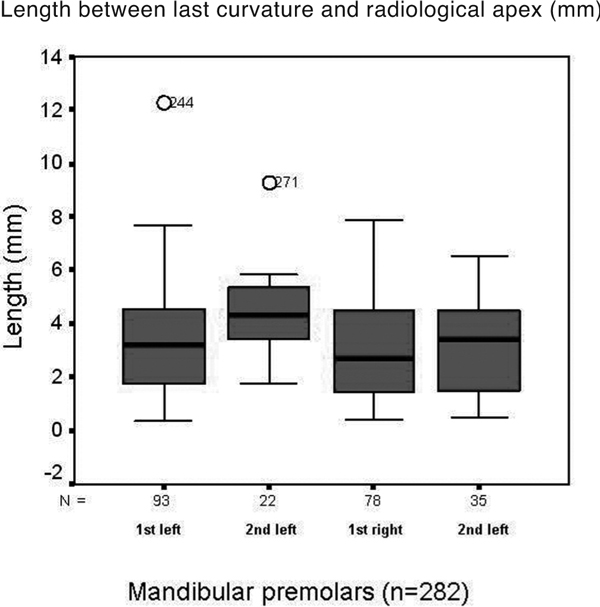
Measured length (distance III) between the last curvature and the radiological apex.
Figure 5.

Measured angles of the first curvature of all investigated mandibular premolars.
Figure 6.
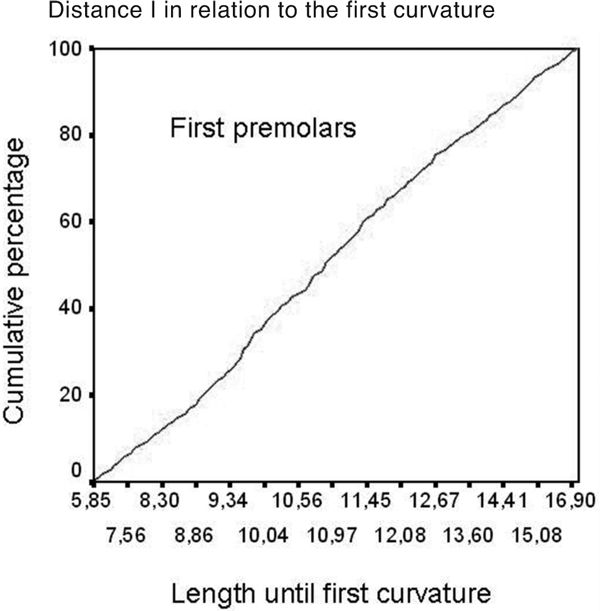
Cumulative frequency and relationship between the length of the distance I and the appearance of a first curvature for the fist mandibular premolars (left and right side together).
Figure 7.
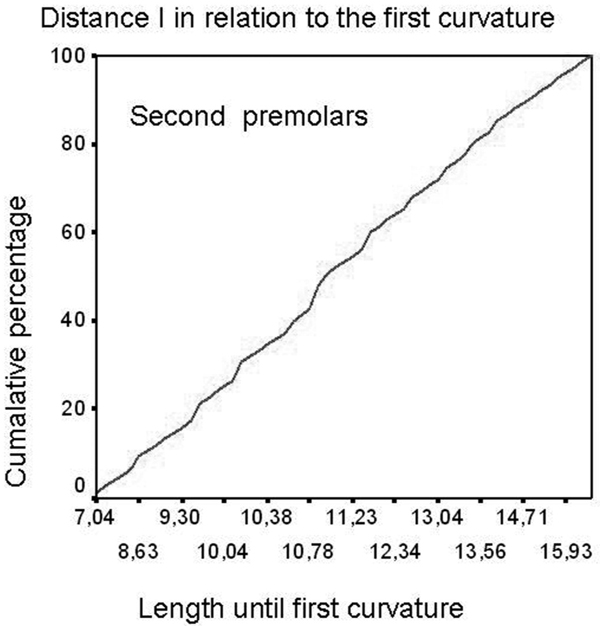
Cumulative frequency and relationship between the length of the distance I and the appearance of a first curvature for the second mandibular premolars (left and right side together).
Discussion
In the present study the localisation and frequency of root canal curvatures in mandibular premolars were determined. According to our exclusion criteria only premolars with one root canal were recorded. Most commonly the mandibular premolars showed only one root canal. In the study of Sert et al. [18] a total of 1400 extracted mandibular permanent teeth from an indigenous Turkish population were evaluated. The authors demonstrated that 62% of mandibular first premolars and 71% of second premolars had a single canal and these morphological characteristics of teeth in this Turkish population were consistent with those of other studies performed on different populations. Numerous authors have dealt with the question of the anatomy and morphology of root canals paying special attention to the curvatures and their corresponding angles [8,19,20,22]. Dobo et al. [4] examined a mathematical description of root canal forms using a differential geometrical pattern analysis and computer graphics. The measurements of 433 extracted human roots were carried out on isometric radiographs taken from a clinical view.
Several studies evaluated the configuration of root canal systems [3,5], the root canal path [10] morphological variations [18] as well as the angles of root canal curvatures [6,15,16]. In most of these studies including our own the method according to Schneider [16] has been applied in order to determine root canal curvatures. In our study the initial straight distance (cemento-enamel-junction to the first curvature) showed mean values from 10.8 mm to 12.2 mm for the first and second mandibular premolars, respectively. The corresponding angles ranged from 13° to 19°, respectively. Saletta et al. [14] measured the root canal curvatures taking into account the differences between dental morphotypes and their modifications after mechanical instrumentation. Despite different techniques and diverse methods of investigation the information gained is still insufficient regarding the relevant length and straight distances that are necessary for the successful placement of cores for definite restorations after endodontic treatments. It is essential that the core is placed in a central position within the root canal access. Any deviation from the original canal path will increase the possibility of a permanent stress in the root; which may lead to endodontic treatment failure, root canal fracture up to the loss of teeth. The initial straight length and the corresponding first angles are the landmarks of which an operator should be aware when placing a core. It is recommended to not only consider the total length of the root canal but also the first straight distance up to the appearance of a first curvature. The present data provide evidence that the first root canal curvature appears after 9 mm of the initial straight length. This means that first curvatures will occur in the first half of the total canal length. In conclusion we could demonstrate that the probability of the appearance of a root canal curvature in human mandibular premolars has a sigmoid line. The determined line graphs prove that there is an increasing tendency of curvatures in root canal length ranging from 9 to 12 mm and that in mandibular premolars great deviation from the original canal path can be expected 9 mm from the cemento-enamel-junction.
References
- Bjorndal L, Carlsen O, Thuesen G, Darvann T, Kreiborg S. External and internal macromorphology in 3D-reconstructed maxillary molars using computerized X-ray microtomography. Int Endod J. 1999;32:3–9. doi: 10.1046/j.1365-2591.1999.00172.x. [DOI] [PubMed] [Google Scholar]
- Blaskovic-Subat V, Smojver B, Maricic B, Sutalo J. A computerized method for the evaluation of root canal morphology. Int Endod J. 1995;28:290–296. doi: 10.1111/j.1365-2591.1995.tb00318.x. [DOI] [PubMed] [Google Scholar]
- Cunningham CJ, Senia ES. A three-dimensional study of canal curvatures in the mesial roots of mandibular molars. J Endod. 1992;18:294–300. doi: 10.1016/S0099-2399(06)80957-X. [DOI] [PubMed] [Google Scholar]
- Dobo NC, Keszthelyi G, Sulyok P, Ledecyky G, Szabo J. Mathematical description of the three-dimensional axis of the root canal of human teeth. Fogorz Sz. 2002;95:155–157. [PubMed] [Google Scholar]
- Dobo-Nagy C, Keszthelyi G, Szabo J, Sulyok P, Ledeczky G, Szabo J. A computerized method for mathematical description of three-dimensional root canal axis. J Endod. 2000;26:639–643. doi: 10.1097/00004770-200011000-00002. [DOI] [PubMed] [Google Scholar]
- Günday M, Sazak H, Garip Y. A comparative study of three different root canal curvature measurement techniques and measuring the canal access angle in curved canals. J Endod. 2005;31:796–798. doi: 10.1097/01.don.0000158232.77240.01. [DOI] [PubMed] [Google Scholar]
- Jafarzadeh H, Wu Y-N. The c-shaped root canal configuration: a review. J Endod. 2007;33:517–523. doi: 10.1016/j.joen.2007.01.005. [DOI] [PubMed] [Google Scholar]
- Jerome CE. C-shaped root canal systems: diagnosis, treatment, and restoration. Gen Dent. 1994;42:424–427. [PubMed] [Google Scholar]
- Kartal N, Ozcelik B, Cimilli H. Root canal morphology of maxillary premolars. J Endod. 1998;24:417–419. doi: 10.1016/S0099-2399(98)80024-1. [DOI] [PubMed] [Google Scholar]
- Lee JK, Ha BH, Choi JH. Quantitative three-dimensional analysis of root canal curvature in maxillary first molars using micro-computed tomography. J Endod. 2006;32:941–945. doi: 10.1016/j.joen.2006.04.012. [DOI] [PubMed] [Google Scholar]
- Mayo CV, Montgomery S, del Rio C. A computerized method for evaluating root canal morphology. J Endod. 1986;12:2–7. doi: 10.1016/S0099-2399(86)80274-6. [DOI] [PubMed] [Google Scholar]
- Naoum HJ, Love RM, Chandler NP, Herbison P. Effect of X-ray beam angulation and intraradicular contrast medium on radiographic interpretation of lower first molar root canal anatomy. Int Endod J. 2003;36:12–19. doi: 10.1046/j.0143-2885.2003.00604.x. [DOI] [PubMed] [Google Scholar]
- Nattress BR, Martin DM. Predictability of radiographic diagnosis of variations in root canal anatomy in mandibular incisor and premolar teeth. Int Endod J. 1991;24:58–62. doi: 10.1111/j.1365-2591.1991.tb00808.x. [DOI] [PubMed] [Google Scholar]
- Saletta D, Baldi C, Nieri M, Ceppatelli P, Franceschi D, Rotundo R, Cairo F, Pini Prato GP. Root curvature: differences among dental morphotypes and modifications after mechanical instrumentation. J Periodontol. 2005;76:723–730. doi: 10.1902/jop.2005.76.5.723. [DOI] [PubMed] [Google Scholar]
- Schäfer E, Diez C, Hoppe W, Tepel J. Roentgenographic investigation of frequency and degree of canal curvatures in human permanent teeth. J Endod. 2002;28:211–216. doi: 10.1097/00004770-200203000-00017. [DOI] [PubMed] [Google Scholar]
- Schneider SW. A comparison of canal preparations in straight and curved canals. Oral Surg Oral Med Oral Pathol. 1971;32:271–275. doi: 10.1016/0030-4220(71)90230-1. [DOI] [PubMed] [Google Scholar]
- Schwartz RS, Robbins JW. Post placement and restoration of endodontically treated teeth: a literature review. J Endod. 2004;30:289–301. doi: 10.1097/00004770-200405000-00001. [DOI] [PubMed] [Google Scholar]
- Sert S, Aslanalp V, Tanalp J. Investigation of the root canal configurations of mandibular permanent teeth in the Turkish population. Int Endod J. 2004;37:494–499. doi: 10.1111/j.1365-2591.2004.00837.x. [DOI] [PubMed] [Google Scholar]
- Sonntag D, Stachniss-Carp S, Stachniss C, Stachniss V. Determination of root canal curvatures before and after canal preparation (part II): a method based on numeric calculus. Aust Endod J. 2006;32:16–25. doi: 10.1111/j.1747-4477.2006.00003.x. [DOI] [PubMed] [Google Scholar]
- Vertucci FJ. Root canal anatomy of the human permanent teeth. Oral Surg Oral Med Oral Pathol. 1984;58:589–599. doi: 10.1016/0030-4220(84)90085-9. [DOI] [PubMed] [Google Scholar]
- Willershausen B, Tekyatan H, Kasaj A, Briseno B. Roentgenographic in vitro investigation of frequency and location of curvatures in human maxillary premolars. J Endod. 2006;32:307–311. doi: 10.1016/j.joen.2005.09.011. [DOI] [PubMed] [Google Scholar]
- Yoshioka T, Villegas JC, Kobayashi C, Suda H. Radiographic evaluation of root canal multiplicity in mandibular first premolars. J Endod. 2004;30:73–74. doi: 10.1097/00004770-200402000-00002. [DOI] [PubMed] [Google Scholar]