

Abstract
Objectives
Chronic kidney disease is frequent in patients after orthotopic liver transplantation (OLT) and has impact on survival. Patients receiving calcineurin inhibitors (CNI) are at increased risk to develop impaired renal function. Early CNI reduction and concomitant use of mycophenolat mofetil (MMF) has been shown to improve renal function.
Methods
The aim of this trial was to compare dose-reduced CNI/MMF versus CNI-free MMF/prednisone-based treatment in stable patients after OLT with respect to glomerular filtration rate (GFR). 21 patients [GFR 44.9 ± 9.9 mL/min/1.73 m2 measured by 99m-Tc-DTPA-clearance, serum creatinine (SCr) 1.5 ± 0.42 mg/dL] were randomized either to exchange CNI for 10 mg prednisone (group 1; n = 8) or to receive CNI at 25% of the initial dose (group 2; n = 13) each in combination with 1000 mg MMF b.i.d.
Results
At month 12 mean SCr (-0.3 ± 0.4 mg/dL, p = 0.031) and GFR improved (8.6 ± 13.1 mL/min/1.73 m2, p = 0.015) in group 2 but remained unchanged in group 1. Main side effects were gastroinstestinal symptoms (14.3%) and infections (4.8%). Two biopsy proven, steroid-responsive rejections occurred. In group 1 mean diastolic blood pressure (BP) increased by 11 ± 22 mmHg (p = 0.03).
Conclusions
Reduced dose CNI in combination with MMF but not CNI-free-immunosuppression leads to improvement of GFR in patients with moderately elevated SCr levels after OLT. Addition of steroids resulted in increased diastolic blood pressure presumably counterbalancing the benefits of CNI withdrawal on renal function.
Keywords: calcineurin inhibitor, GFR, impaired renal function, liver transplantation, mycophenolate mofetil
Introduction
Liver transplant recipients are the second most frequent group of patients, who develop chronic renal failure among all recipients of solid organ transplantation [1]. Up to 18% of patients after OLT have been shown to suffer from end stage renal disease (ESRD) within 10 years after engraftment [2]. Apart from preoperative GFR, diabetes and chronic hepatitis C infection [1,3], the use of calcineurin inhibitor (CNI) based immunosuppression has been shown to put the patient at particular risk to develop chronic kidney disease [4].
Therefore, both CNI-sparing and CNI free regimens should offer an opportunity to treat liver transplant recipients with impaired renal function. Whereas CNI reduction with concomitant use of mycophenolate mofetil (MMF) has been demonstrated as an successful and safe option [6-13], MMF monotherapy was complicated by a high frequency of rejection episodes [5,14]. Alternatively CNI withdrawal has been studied in combination with conversion to mTor inhibitors. However, results in such studies are controversial [15,16]. Finally it remains unclear, whether the high rate of rejection episodes can be prevented when MMF monotherapy is combined with steroids.
We performed a single center prospective randomized pilot trial to compare a dose reduced CNI/MMF-versus a MMF/prednisone treatment in patients after liver transplantation with moderately impaired renal function.
Patients and methods
Patient recruitment
Patients were screened for renal impairment by 99m-Tc-DTPA-clearance following the method of Russell et al. [17] and included if GFR was below 70 mL/min/1.73 m2. Additional inclusion criteria consisted of age greater than 18 years and CNI-toxicity as main cause of impaired renal function by excluding other factors such as relevant proteinuria (> 1 g/24 h), hematuria or diabetes mellitus. Exclusion criteria comprised patients with severely increased serum creatinine (SCr) > 5 mg/dL, (re-) infection with hepatitis B (HBs-antigen positive), rejection episodes during the previous 12 months, CMV-infection during the previous 6 months, contraindications for the use of corticosteroids or MMF, pregnancy or breast-feeding, unwillingness in pre-menopausal women to take contraceptives for the duration of the study, active gastric ulcer disease, malignancy, hemoglobin < 10 g/dL, total leucocyte counts < 3.5 G/L and platelet counts < 70 G/L.
The study protocol was approved by the local ethics committee in accordance with the principles of the declaration of Helsinki.
Study protocol
Patients were randomized either to completely discontinue CNI and to add 10 mg prednisone instead (group 1) or to reduce the CNI to 25% of the initial dosage without any additional corticosteroids (group 2). Each patient received 1000 mg MMF b.i.d. CNI was tapered stepwise over 8 weeks after target MMF dose was achieved. To ensure equal renal function starting levels patients were first stratified with respect to serum creatinine above and below 1.4 mg/dL and than randomly allocated to the study groups at a 1:1 ratio using randomization blocks of five subjects.
For every suspected rejection, histological confirmation was obtained. Patients with biopsy proven rejection (BPR) were judged as treatment failure and withdrawn from the study.
Follow up
After study inclusion, patients were monitored in weekly intervals for the first 14 weeks. At each visit blood counts, liver functions tests and ciclosporine-or tacrolimus 12-h serum concentrations were measured and any side effects were recorded. At inclusion as well as after months 6 and 12 serum creatinine (Scr) and 99m-Tc-DTPA-clearance were measured.
Analysis of the data
The study was evaluated on an intent-to treat (ITT-) basis. Results are expressed as arithmetic means ± SD. Statistical analysis was performed using the StatView 5.0™Software (Version for Windows; SAS Institute Inc., Cary, NC, USA). Differences between the groups were analyzed by Mann-Whitney-Test and differences of paired values by Wilcoxon-Rank-Test. p-values < 0.05 were considered significant.
Results
Baseline characteristics
Between May 2003 and May 2005 twenty-one patients with a GFR < 70 mL/min/1.73 m2 were randomized into the treatment groups (group 1: n = 8; group 2: n = 13). Patient characteristics and immunosuppressive medication at the time of study inclusion are given in Table 1. There were no statistical significant differences noted between both groups regarding age, time since engraftment and renal function as determined by SCr and 99Tc-DTPA-clearance.
Table 1.
Patients baseline characteristics at study inclusion
| All(n = 21) | Group 1(n = 8) | Group2(n = 13) | P = | |
|---|---|---|---|---|
| Age (years) | 47.9 ± 11.3 | 47.3 ± 11.8 | 48.4 ± 11.5 | 0.71 |
| Male/female | 12/9 | 4/4 | 8/5 | |
| Time after engraftment (months) | 6 ± 3.1 | 6.3 ± 3.4 | 5.5 ± 2.8 | 0.71 |
| Baseline creatinine (mg/dL) | 1.5 ± 0.42 | 1.57 ± 0.46 | 1.45 ± 0.41 | 0.64 |
| Baseline GFR (mL/min) | 44.9 ± 9.9 | 42.2 ± 10.2 | 46.5 ± 9.8 | 0.33 |
| Immunosuppression at the time of inclusion | ||||
| Ciclosporin/through level (ng/ml) | N = 10 (83.9 ± 14.5) |
N = 5 (85.6 ± 17.6) |
N = 5 (81.7 ± 12.4) |
0.72 |
| Tacrolimus/through level (ng/ml) | N = 11 (9.1 ± 1.7) |
N = 3 (9.2 ± 2.4) |
N = 8 (9.1 ± 1.4) |
0.73 |
| Prednisone frequency/dose (mg/day) | N = 7 (4.4 ± 1.5) | N = 5 (5 ± 0) | N = 2 (3 ± 2.8) | |
Values are given as mean ± SD.
CNI through levels at baseline were 9.1 ± 1.4 ng/ml (tacrolimus) and 83.9 ± 14.5 ng/mL (ciclosporin) in group 1 and 9.1 ± 1.7 ng/mL and 81.7 ± 12.4 ng/mL in group 2, respectively. In group 2 CNI levels were reduced to 3.4 ± 1.9 ng/mL (tacrolimus) and 26.7 ± 3.5 (ciclosporin) at month 6 and 3.7 ± 1.9 ng/mL and 32 ± 5.7 ng/mL at month 12, respectively.
Effect on renal function
SCr levels and GFRs are summarized in Figures 1 and 2, respectively. At month 6, none of the groups revealed a significant change of SCr and GFR as compared to baseline. After 12 months, however, a statistically significant decrease of mean SCr (-0.3 ± 0.4 mg/dL, p = 0.031) and a corresponding rise in mean GFR (8.6 ± 13.1 mL/min/1.73 m2, p = 0.015) could be recorded in patients randomized into group 2, whereas no significant improvement of GFR was noted in patients on CNI-free treatment (-0.1 ± 0.4 mg/dL and 1.5 ± 17.7 mL/min/1.73 m2, respectively).
Figure 1.
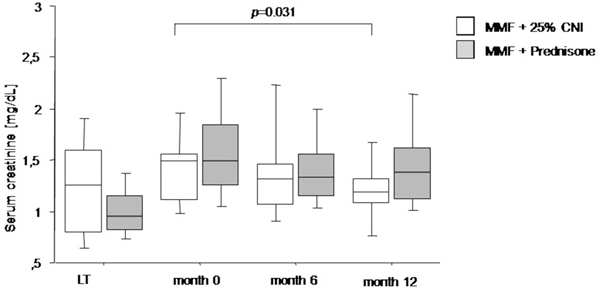
SCr levels measured after engraftment, at study inclusion and months 6 and 12 after conversion to MMF therapy. Data are given as box plots, where the limits of the boxes indicate the 25th and 75th percentiles and the lines inside the boxes indicate the 50th (median) percentile. The whiskers indicate the 10th and 90th percentiles.
Figure 2.
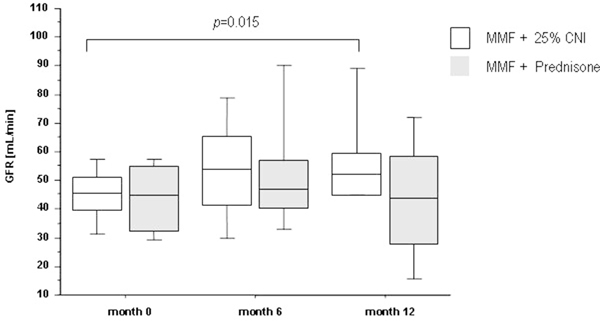
GFR measured by 99m-Tc-DTPA-Clearance at study inclusion and months 6 and 12 after conversion to MMF therapy. Data are given as box plots, where the limits of the boxes indicate the 25th and 75th percentiles and the lines inside the boxes indicate the 50th (median) percentile. The whiskers indicate the 10th and 90th percentiles.
Course of blood pressure and blood lipid levels
In the CNI-free steroid containing treatment arm a significant rise in mean diastolic blood pressure was recorded from 73.2 ± 15.1 mmHg at study inclusion to 83.6 ± 10.3 mmHg at month 12 (11 ± 22 mmHg; p = 0.03), whereas diastolic and systolic blood pressure remained unchanged in patients receiving CNI at a reduced dosage (Figure 3). At baseline, 7 patients received antihypertensive medication, which was intensified in 2 patients during the course of the study (one in each group). One additional patient from group 1 had to be started on antihypertensive treatment. In contrast to blood pressure, mean levels of cholesterin and triglycerides remained unchanged after conversion to the study medication and during follow up. At baseline a single patient in group 2 received a statin owing to the need for highly active antiretroviral therapy to treat coexisting HIV infection. In this individual, a dramatic decrease of triglycerides was noted after conversion to the CNI-free regimen. One more patient (group 2) had to be started on a lipid-lowering medication during the course of the study.
Figure 3.
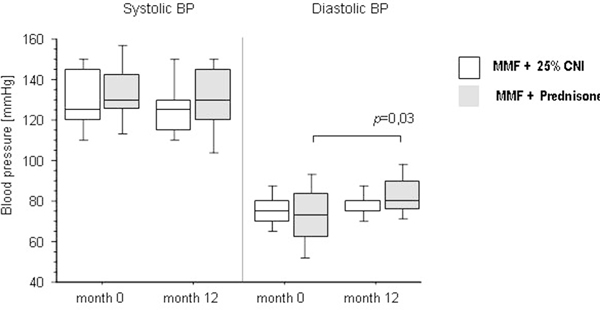
Systolic and diastolic BP at baseline and 12 months after inclusion into the study. Data are given as box plots, where the limits of the boxes indicate the 25th and 75th percentiles and the lines inside the boxes indicate the 50th (median) percentile. The whiskers indicate the 10th and 90th percentiles.
Side effects and rejection episode
Observed side effects (SE) consisted of gastrointestinal problems (abdominal discomfort and diarrhea) (14.3%), genital herpes simplex infection (4.8%), observation of pleural effusion and ascites of unknown etiology (polyserositis) (4.8%) and myoclonia (4.8%). One patient experienced acute renal failure with the onset of heavy diarrhea and was discontinued from the study. Under treatment with intravenous fluids renal function could be restored to the previous level. Allocation of the side effects to both treatment groups and SE-related discontinuation of MMF therapy are depicted in Table 2. In the patient with polyserositis, symptoms re-occurred 17 months after dis-continuation of MMF application. There was no significant change in serum ALT levels during the study period (Figure 4). BPR occurred in 2 patients. The first patient, allocated to treatment group 1, underwent liver biopsy because of an increase of liver function tests at week 32. She was re-placed on tacrolimus based immunosuppression after receipt of the pathology report. The second patient underwent liver biopsy because of the appearance of unclear polyserositis in the absence of increased liver function tests. Both rejections were considered as mild by the pathologist and responded well to steroid pulse therapy.
Table 2.
Observed side effects after conversion to MMF
| All (n =) | Group 1 (n =) | Group 2 (n =) | Discontinuation | |
|---|---|---|---|---|
| Gastroinestinal symptoms (abdominal discomfort, diarrhea) | 3 | 2 | 1 | 2 |
| Herpes simplex infection | 1 | 0 | 1 | 0 |
| Ascites/pleural effusion | 1 | 0 | 1 | 0 |
| Myoclonia | 1 | 0 | 1 | 1 |
| Rejection (BPR) | 2 | 1 | 1 | 2 |
Figure 4.
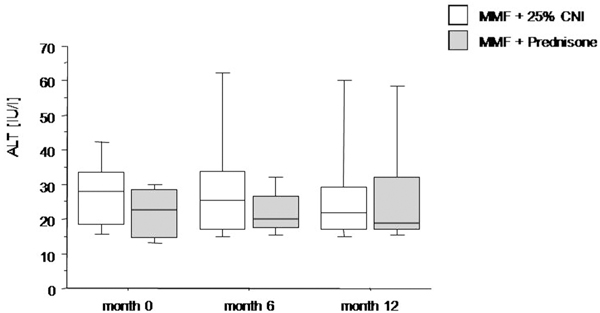
ALT levels measured at study entry and at months 6 and 12 after conversion to MMF therapy. Data are given as box plots, where the limits of the boxes indicate the 25th and 75th percentiles and the lines inside the boxes indicate the 50th (median) percentile. The whiskers indicate the 10th and 90th percentiles.
Altogether study medication had to be terminated in 5 patients (23.8%). Discontinuation of the study medication occurred due to side effects or rejection (GI-side effects n = 2, myoclonia n = 1, BPR n = 2). One additional patient withdrew consent shortly after study inclusion due to the discontinuation of contraceptive medication.
None of the patients required dose adjustments for low leukocyte, platelet counts or anemia and none developed diabetes.
Discussion
Here, we report the results of a pilot trial on CNI-free versus a CNI reduced immunosuppression under the concomitant use of MMF in liver transplant recipients with impaired renal function, applying 99m-Tc-DTPA clearance - the gold standard method - to measure GFR. We found, that conversion to MMF in combination with CNI-dose reduction was able to significantly improve GFR, whereas the CNI-free regimen in combination with steroids did not ameliorate renal function.
Previous studies have already demonstrated a positive effect of CNI-dose reduction on renal function in liver transplant recipients with chronic kidney disease. The following various approaches have been studied: de novo immunosuppression with MMF combined with delayed introduction of CNI's [7-9], reduced dose CNIs either de novo [10] or reduction after more than one year after engraftment [11-14]. However, in these studies assessment of renal function had been based on indirect methods such as serum creatinine [5], creatinine clearance [11-13] or creatinine based estimated GFR (eGFR) [7-9]. In contrast, we applied 99m-Tc-DTPA-clearance - a radioisotope gold standard method to measure glomerular function - to evaluate the course of renal function after conversion, since it has meanwhile been well established that serum creatinine and creatinine based equations, e.g. MDRD, only insufficiently reflect true GFR [18,19]. In contrast to the work of Schlitt, Reich and Créput [5,11,14], CNI-free immunosuppression did not reveal any improvement of renal function in our patients. However, since we used an ITT analysis, the number of drop-outs may have influenced our assessment of outcomes.
In our study, CNI-free immunosuppression comprised MMF in combination with corticosteroids, which had been chosen, because a high number of rejections had been reported in patients with MMF monotherapy. Although only a low dose of 10 mg prednisone was administered, this type of treatment was associated with an increment of 11 mmHg in diastolic blood pressure. This unexpected effect may have counterbalanced the potentially positive effects of CNI withdrawal in our patients in group 1. On the other hand, both MMF in combination with reduced dose CNI and MMF in combination with corticosteroids proved to be relatively safe, taking into account that acute rejection occurred in only 10% (2/21) of patients. Of note, all rejection episodes responded well to corticosteroid pulse therapy, so that normal hepatic function was restored in all patients with rejection. Both rejection episodes occurred in a "stable phase" of immunsuppression 4.6 and 7.5 months after conversion, so that the causal relationship to the treatment protocol remains unclear. In our study the frequency of BPR was similar to that reported by Reich et al. (9-14%) but higher than in the trials of Pageaux and Creput (0%) [11-13].
As expected, gastrointestinal intolerance was the most frequent side effect, which required treatment discontinuation in 2 of 3 patients with this complication. Otherwise, the spectrum of side effects was similar to other studies. Herpes infection is a complication which had already been previously attributed to MMF treatment [20]. In contrast, myoclonia, which was observed in a single patient of group 2 has not yet been reported under MMF medication. Finally, polyserositis which was observed also in a patient must most likely not be attributed to MMF medication, because the syndrome re-occurred 17 months after MMF had been discontinued.
This study had been planned as a pilot trial to provide data for a larger multicentre trial. Thus the low number of patients and the single centre design may limit interpretation of our results. Nevertheless, we obtained a clear result not favouring CNI-free immunosuppression in liver transplant recipients with impaired renal function. Of note this result is based on direct measurement of GFR with a gold standard method rather than indirect assessments of renal function by serum creatinine or eGFR which may be invalid in patients after liver transplantation [18,19] or with impaired liver function.
Thus, the obligate use of corticosteroids with their potentially hypertensive effect cannot be generally recommended in a CNI-free regimen of MMF-based immunosuppression. In addition, our trial adds evidence to the existing data using a GFR gold standard meaesurement, that CNI-reduction in combination with MMF is a safe and effective method to treat liver transplant recipients with an impairment of renal function.
Abbreviations
CNI: calcineurin inhibitor; GFR: glomerular filtration rate; eGFR: estimated GFR; MMF: mycophenolate mofetil; OLT: orthotopic liver transplantation; SE: side effects; SCr: serum creatinine
Acknowledgements
This study was supported by an unrestricted grant from Roche Pharma AG, Grenzach-Whylen, Germany.
References
- Ojo AO, Held PJ, Port FK, Wolfe RA, Leichtman AB, Young EW, Arndorfer J, Christensen L, Merion RM. Chronic renal failure after transplantation of a nonrenal organ. N Engl J Med. 2003;349(10):931–940. doi: 10.1056/NEJMoa021744. [DOI] [PubMed] [Google Scholar]
- Gonwa TA, Mai ML, Melton LB, Hays SR, Goldstein RM, Levy MF, Klintmalm GB. End-stage renal disease (ESRD) after orthotopic liver transplantation (OLTX) using calcineurin-based immunotherapy: risk of development and treatment. Transplantation. 2001;72(12):1934–1939. doi: 10.1097/00007890-200112270-00012. [DOI] [PubMed] [Google Scholar]
- Pawarode A, Fine DM, Thuluvath PJ. Independent risk factors and natural history of renal dysfunction in liver transplant recipients. Liver Transpl. 2003;9(7):741–747. doi: 10.1053/jlts.2003.50113. [DOI] [PubMed] [Google Scholar]
- Falkenhain ME, Cosio FG, Sedmak DD. Progressive histologic injury in kidneys from heart and liver transplant recipients receiving cyclosporine. Transplantation. 1996;62(3):364–370. doi: 10.1097/00007890-199608150-00011. [DOI] [PubMed] [Google Scholar]
- Schlitt HJ, Barkmann A, Boker KH, Schmidt HH, Emmanouilidis N, Rosenau J, Bahr MJ, Tusch G, Manns MP, Nashan B, Klempnauer J. Replacement of calcineurin inhibitors with mycophenolate mofetil in liver-transplant patients with renal dysfunction: a randomised controlled study. Lancet. 2001;357(9256):587–591. doi: 10.1016/S0140-6736(00)04055-1. [DOI] [PubMed] [Google Scholar]
- Beckebaum S, Cicinnati VR, Klein CG, Brokalaki E, Yu Z, Malago M, Frilling A, Gerken G, Broelsch CE. Impact of combined mycophenolate mofetil and low-dose calcineurin inhibitor therapy on renal function, cardiovascular risk factors, and graft function in liver transplant patients: preliminary results of an open prospective study. Transplant Proc. 2004;36(9):2671–2674. doi: 10.1016/j.transproceed.2004.10.008. [DOI] [PubMed] [Google Scholar]
- Yoshida EM, Marotta PJ, Greig PD, Kneteman NM, Marleau D, Cantarovich M, Peltekian KM, Lilly LB, Scudamore CH, Bain VG, Wall WJ, Roy A, Balshaw RF, Barkun JS. Evaluation of renal function in liver transplant recipients receiving daclizumab (Zenapax), mycophenolate mofetil, and a delayed, low-dose tacrolimus regimen vs. a standard-dose tacrolimus and mycophenolate mofetil regimen: a multicenter randomized clinical trial. Liver Transpl. 2005;11(9):1064–1072. doi: 10.1002/lt.20490. [DOI] [PubMed] [Google Scholar]
- Soliman T, Hetz H, Burghuber C, Györi G, Silberhumer G, Steininger R, Mühlbacher F, Berlakovich GA. Short-term induction therapy with anti-thymocyte globulin and delayed use of calcineurin inhibitors in orthotopic liver transplantation. Liver Transpl. 2007;13(7):1039–1044. doi: 10.1002/lt.21185. [DOI] [PubMed] [Google Scholar]
- Neuberger JM, Mamelok RD, Neuhaus P, Pirenne J, Samuel D, Isoniemi H, Rostaing L, Rimola A, Marshall S, Mayer AD. ReSpECT Study Group. Delayed introduction of reduced-dose tacrolimus, and renal function in liver transplantation: the 'ReSpECT' study. Am J Transplant. 2009;9(2):327–336. doi: 10.1111/j.1600-6143.2008.02493.x. [DOI] [PubMed] [Google Scholar]
- Tzakis AG, Tryphonopoulos P, Kato T, Nishida S, Levi DM, Madariaga JR, Gaynor JJ, De Faria W, Regev A, Esquenazi V, Weppler D, Ruiz P, Miller J. Preliminary experience with alemtuzumab (Campath-1H) and low-dose tacrolimus immunosuppression in adult liver transplantation. Transplantation. 2004;77(8):1209–1214. doi: 10.1097/01.TP.0000116562.15920.43. [DOI] [PubMed] [Google Scholar]
- Pageaux GP, Rostaing L, Calmus Y, Duvoux C, Vanlemmens C, Hardgwissen J, Bernard PH, Barbotte E, Vercambre L, Bismuth M, Puche P, Navarro F, Larrey D. Mycophenolate mofetil in combination with reduction of calcineurin inhibitors for chronic renal dysfunction after liver transplantation. Liver Transpl. 2006;12(12):1755–1760. doi: 10.1002/lt.20903. [DOI] [PubMed] [Google Scholar]
- Reich DJ, Clavien PA, Hodge EE. Mycophenolate mofetil for renal dysfunction in liver transplant recipients on cyclosporine or tacrolimus: randomized, prospective, multicenter pilot study results. Transplantation. 2005;80(1):18–25. doi: 10.1097/01.TP.0000165118.00988.D7. [DOI] [PubMed] [Google Scholar]
- Créput C, Blandin F, Deroure B, Roche B, Saliba F, Charpentier B, Samuel D, Durrbach A. Long-term effects of calcineurin inhibitor conversion to mycophenolate mofetil on renal function after liver transplantation. Liver Transpl. 2007;13(7):1004–1010. doi: 10.1002/lt.21170. [DOI] [PubMed] [Google Scholar]
- Stewart SF, Hudson M, Talbot D, Manas D, Day CP. Mycophenolate mofetil monotherapy in liver transplantation. Lancet. 2001;357(9256):609–610. doi: 10.1016/S0140-6736(00)04065-4. [DOI] [PubMed] [Google Scholar]
- Watson CJ, Gimson AE, Alexander GJ, Allison ME, Gibbs P, Smith JC, Palmer CR, Bradley JA. A randomized controlled trial of late conversion from calcineurin inhibitor (CNI)-based to sirolimus-based immunosuppression in liver transplant recipients with impaired renal function. Liver Transpl. 2007;13(12):1694–1702. doi: 10.1002/lt.21314. [DOI] [PubMed] [Google Scholar]
- Shenoy S, Hardinger KL, Crippin J, Desai N, Korenblat K, Lisker-Melman M, Lowell JA, Chapman W. Sirolimus conversion in liver transplant recipients with renal dysfunction: a prospective, randomized, single-center trial. Transplantation. 2007;83(10):1389–1392. doi: 10.1097/01.tp.0000261630.63550.41. [DOI] [PubMed] [Google Scholar]
- Russell CD, Bischoff PG, Kontzen FN, Rowell KL, Yester MV, Lloyd LK, Tauxe WN, Dubovsky EV. Measurement of glomerular filtration rate: single injection plasma clearance method without urine collection. J Nucl Med. 1985;26(11):1243–1247. [PubMed] [Google Scholar]
- Gonwa TA, Jennings L, Mai ML, Stark PC, Levey AS, Klintmalm GB. Estimation of glomerular filtration rates before and after orthotopic liver transplantation: evaluation of current equations. Liver Transpl. 2004;10(2):301–309. doi: 10.1002/lt.20017. [DOI] [PubMed] [Google Scholar]
- Gerhardt T, Pöge U, Stoffel-Wagner B, Ahrendt M, Wolff M, Spengler U, Palmedo H, Sauerbruch T, Woitas RP. Estimation of glomerular filtration rates after orthotopic liver transplantation: Evaluation of cystatin C-based equations. Liver Transpl. 2006;12(11):1667–1672. doi: 10.1002/lt.20881. [DOI] [PubMed] [Google Scholar]
- Herrero JI, Quiroga J, Sangro B, Pardo F, Rotellar F, Alvarez-Cienfuegos J, Prieto J. Herpes zoster after liver transplantation: incidence, risk factors, and complications. Liver Transpl. 2004;10(9):1140–1143. doi: 10.1002/lt.20219. [DOI] [PubMed] [Google Scholar]