

Abstract
Background:
Root canal cleaning is an important step in endodontic therapy. In order to develop better techniques, a new generation of endodontic instruments has been designed. The aim of this study was to compare the effectiveness of manual K-files (Mani Co, Tokyo, Japan) and two rotary systems–Mtwo (Dentsply-Maillefer, Ballaigues, Switzerland) and ProTaper (VDW, Munich, Germany)–for root canal preparation in primary molars.
Materials and Methods:
India ink was injected to 160 mesiobuccal and distal root canals of mandibular primary molars. The teeth were randomly divided into three experimental groups and one control group. In each experimental group, either manual instruments (K-files) or rotary instruments (Mtwo or ProTaper) were used to prepare root canals. After cleaning the canals and clearing the teeth, ink removal was evaluated with a stereomicroscope. Statistical analysis was done with Kruskal–Wallis and Friedman tests.
Results:
There were no significant differences in cleaning efficiency between manual and rotary instruments. Only ProTaper files performed significantly better in the coronal and middle thirds than in the apical third of the root canal.
Conclusion:
Manual K-files and the Mtwo and ProTaper rotary systems showed equally acceptable cleaning ability in primary molar root canals.
Keywords: Deciduous tooth, root canal preparation, root canal therapy
INTRODUCTION
The removal of organic debris is the main purpose of filing in pulpectomy procedures in primary teeth.[1] This goal can be achieved with manual or rotary nickel-titanium (NiTi) instruments.[2–4] The design and flexibility of NiTi alloy instruments allow files to preserve the original anatomy of curved canals,[3,5,6] especially in primary teeth and reduce procedural errors.[5] In addition, because of the funnel-shaped canal preparation, a more predictably uniform paste filling can be obtained in primary teeth.[2] Rotary files also favor the patient's cooperation by shortening treatment time for cleaning canals.[4] However, the high cost of NiTi rotary systems and need for training to learn the technique are disadvantages of NiTi rotary files.[2–6]
NiTi rotary instruments of different designs are available.[7] Manufacturers have tried to promote their cleaning efficacy for root canal preparations, simplify the procedures and decrease instrumentation time, which are particular considerations in children. Accordingly, some studies have focused on NiTi rotary endodontic systems in pulpectomy of primary teeth;[2–4,6,8–10] however, most researchers have tested these instruments only in permanent teeth.[5,11,12]
A new generation of NiTi rotary files appeared with the Mtwo endodontic instruments. The basic series (standard set) of Mtwo rotary files includes four instruments with variable tip sizes ranging from no. 10 to no. 25, tapers ranging from .04 to .06–.07 and two lengths: 21 and 25 mm. Also file tips range in size from 30, 35, 40 and tapers of 0.5, 0.4 and 0.7 are available.
The manufacturer recommends that all Mtwo files should be used for the full length of the root canal (single-length technique).[13–15] Smaller instruments are used before larger ones, as in the step-back method. The specific design and flexibility of Mtwo instruments maintain the original root canal curvature, and these instruments are effective and safe, so cleaning can be completed in less time.[13,14]
Another rotary NiTi system is the ProTaper system, which consists of one file as an orifice opener (SX), two shaping files (S1, S2) and five finishing files (F1-F5). The files have a variable tapered shaft that is designed for the crown-down technique. File tips range in size from 20 to 50, and tapers of 0.07, 0.08 and 0.09 are available.[16] A crown-down technique is recommended for ProTaper instruments, in which larger files are used before smaller ones and canals are prepared with a coronal-to-apical approach.[11,17–19]
Several studies have compared the effectiveness of rotary NiTi files and manual instruments in cleaning root canals in permanent teeth. Most have concluded that NiTi rotary systems are faster than manual files,[3–5,9,10] reduce errors during root canal preparation, and preserve root canal shape.[4,5,20] Foschi et al. reported that both the Mtwo and Protaper rotary systems produced a clean canal in the coronal and middle thirds, but were unable to produce dentine surfaces free from smear layer and debris in the apical third.[11] Schafer et al. found debris removal with Mtwo instruments better than K3 and RaCe instruments in permanent teeth.[14] In two separate studies, Sonntag et al.,[21] and Giovannone et al.[18] found no significant difference between instrumentation with Mtwo and Profile on the cleanliness of the root canals of permanent teeth. Gu et al. reported that both Mtwo and Protaper systems are effective in the preparation of permanent curved molar canals.[19] However, the superiority of rotary systems in narrow and curved primary teeth root canals has not been unequivocally documented. Because few studies have compared the cleaning ability of hand files and rotary instruments in deciduous teeth, this in vitro study compared the cleaning ability of manual instruments (K-files) and two rotary systems (Mtwo and ProTaper) in the preparation of primary molar root canals.
MATERIALS AND METHODS
The research protocol for this study was submitted to the Human Ethics Review Committee of the School of Dentistry, Shiraz, University of Medical Sciences. After the method was approved, extracted primary teeth from several dental clinics in Shiraz and neighboring suburbs were obtained during 3 months. All patients’ parents were informed about the purpose of the research and the way the extracted teeth would be used for in vitro study. The exact reasons for tooth extraction were unknown to the researchers, but it was assumed that they were extracted because of dental pain. Immediately after extraction all teeth were stored in distilled water at 37°C. They were then immersed in 0.5% sodium hypochlorite for 1 week for disinfection, and stored in distilled water at 37°C. Among these teeth, 80 mandibular primary molars with intact, complete roots and no signs of root resorption were selected for this study. Included were 47 first mandibular molars and 33 second mandibular molars with more than 160 root canals.
Standard coronal access was achieved with diamond fissure burs. All the canals were checked radiographically for apical patency and root canal conditions by inserting a no. 15 K-file into the canals. Teeth with no abnormalities such as internal or external root resorption or canal calcification were selected. In all, 160 fully formed mesiobuccal and distal root canals with closed apices were chosen for canal preparations.
All specimens were then rinsed, and root canals were filed with India ink with a 30-gauge insulin syringe. A no. 15 K-file was introduced into the canal to assure penetration of the ink and prevent bubble formation. The teeth were left in wet conditions at room temperature for 48 h, and were then randomly divided into experimental and control groups. The three experimental groups contained 20 teeth each. Group 1 specimens were instrumented with stainless steel K-files; in group 2 Mtwo NiTi rotary files were used, and in group 3 ProTaper files were used. The mesiobuccal and distal root canals of each tooth were used for all endodontic procedures. In the control group, the root canals of 20 teeth were filled with ink and irrigated with normal saline but not instrumented.
All root canals were prepared by the same operator. The working length was recorded as the length of the initial file at the apical foramen minus 1 mm. In group 1, all 40 root canals were instrumented manually with K-files (Mani Co, Tokyo, Japan) with the step-back technique up to file no. 25- 30. In group 2 all 40 canals were cleaned with the Mtwo rotary system (VDW, Munich, Germany), using 21 mm files. The instruments were used to the full length of the root canal, as for the single-length technique. The instrumentation sequence was 10/.04, 15/.05, 20/.06, and 25/.06.
In group 3, all 40 root canals were cleaned with the ProTaper system (Dentsply-Maillefer, Ballaigues, Switzerland) in a crown-down method with three instruments in the following sequence: S1 in the coronal third of the root canal, S2 in the middle third, and F1 at the working length. As a result of a pilot study, we modified the sequence of the three ProTaper instruments slightly to prepare the canals.
The two NiTi rotary systems were driven with a torque-limited rotation Endo IT professional system (VDW, Munich, Germany) with torque control at a standardized speed for all files. In all groups, each instrument was checked after every use, and all files were discarded after 4 uses. In all three experimental groups the canals were flushed with 5 ml normal saline and dried with absorbent paper points. The pulp chamber was filled with temporary cement and teeth were then stored in wet conditions.
To analyze cleaning capacity, the teeth were placed separately in 7% hydrochloric acid for 2 days, and the acid solution was changed daily until the tooth was completely decalcified. Then the teeth were washed under running water and dehydrated in a series of ethyl alcohols: 70% alcohol for 16 h (changed after 8 h) followed by 80% alcohol for 8 h, 95% alcohol for 8 h, and 100% alcohol for 8 h. After dehydration, the teeth were cleared in methyl salicylate (Merck KGaA, Darmstadt, Germany) for 6 h.
Two observers who were unaware of which group the teeth were from examined the transparent teeth under a stereomicroscope (Zeiss, Jena, Germany) at ×10 magnification and scored the amount of India ink remaining in the coronal, middle, and apical thirds of the canal on a scale of 0 to 3 [Figure 1]:
Figure 1.

Cleared clean canals in second mandibular primary molar
0 = total clearing in which the whole canal was completely clean.
1 = almost complete ink removal.
2 = partial ink removal.
3 = no ink removal.
When disagreement arose during evaluations, consensus evaluations were obtained between examiners. Statistical analyses of the data were done with the nonparametric Kruskal–Wallis and Friedman tests (P<0.05).
RESULTS
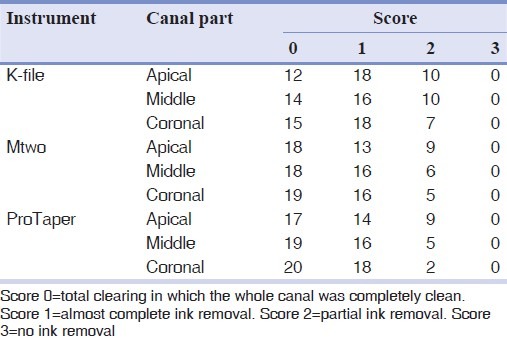
The ink adhered to the root canals and irrigation without instrumentation could not remove it. Comparisons between the control group and the three experimental groups indicated that all the instruments in the three experimental groups we compared were able to remove the ink. Table 1 shows the frequency distributions of different scores in the coronal, middle and apical thirds of root canals after K-file, Mtwo and ProTaper rotary file cleaning. Comparisons between the experimental and control group disclosed statistically significant differences in the apical, middle and coronal thirds of root canals (P<0.05). Statistical analysis detected no significant differences in cleaning capacity between the three instrumentation techniques (P>0.05). Comparisons of the three parts of the canal cleaned with different techniques showed no statistically significant differences between the three regions in group 1 (K-files) and group 2 (Mtwo system) (P<0.05). However, scores for group 3 (ProTaper) differed significantly in the coronal and middle thirds of the canals (P=0.030).
Table 1.
Comparison of cleaning efficacy scores of K-files, Mtwo and ProTaper rotary files in the coronal, middle and apical third of primary molar root canals
DISCUSSION
The importance of root canal cleaning is reflected in the many studies that have focused on different manual instruments and rotary systems for root canal preparation.[7] Most studies have compared the cleaning ability of hand files and rotary instruments in permanent teeth, whereas few of them involved deciduous teeth. This in vitro study compared the preparation efficacy of manual instruments (K-files) and two rotary systems (Mtwo and ProTaper) in the preparation of primary molar root canals. It should be noted that previous studies compared different rotary systems other than the Mtwo and ProTaper systems.[2–4,6,8–10] Different approaches have been used to evaluate the cleaning ability of instruments: Debris removal was the focus of at least once study,[3] and another used scanning electron microscopy to examine smear layer removal.[11] In the debris-removal study just mentioned, the root canals were examined after dying and clearing,[3] which was also the technique used in the present study.
We found no significant differences in the degree of cleaning capacity between manual and rotary techniques (P>0.05). In agreement with our findings, Silva et al.[3] and Schäfer and Zapke[22] have reported that the manual and rotary instruments yielded similar degree of cleanliness. Some studies noted the benefits of hand instrumentation over rotary files with regard to root canal wall preparation;[23,24] however, others reported that NiTi instruments had advantages over hand files.[5,9] The differences in the findings between ours and other studies probably reflect differences in the type of teeth, type of rotary instrument and techniques used, irrigation solutions, and operator experience.[22,23,25]
In the present study, both Mtwo and ProTaper rotary instruments prepared the root canals efficiently, as has been described by others in permanent teeth.[19] Like us, some authors found no significant difference between Mtwo and ProTaper systems regarding their cleaning ability in permanent teeth.[18,25–27] Clinical and laboratory studies in primary teeth have demonstrated the advantages of rotary files for pulpectomy.[2–4,6,8–10] Because there are no clear guidelines for the instrumentation of primary tooth root canals with rotary files, some researchers have used the same principles as for permanent teeth;[2,8] however, others recommended modified rules.[6] In their clinical study, Kuo et al. found that the ProTaper rotary system was efficient and safe for root canal preparation in primary teeth.[6] However, these authors used a combination of one manual file and two ProTaper instruments (SX and S2). In view of the lesser structural thickness and density of the dentin in primary teeth than in permanent teeth,[28] and as a result of our pilot study, we modified the sequences of the three ProTaper instruments used to prepare the canals. These modifications, and our inclusion of both first and second mandibular primary molars, are potential confounders that should be taken into account in future research.
The ability of ProTaper and Mtwo rotary files to clean the root canals depends on the instrument's cross-sectional design and flute. ProTaper files have a triangular cross-section resembling that of a reamer. This design may enhance engagement of the file edges to the canal walls and produce smooth surfaces as well as tapering towards the apex.[11,17] The ProTaper rotary instruments, like Mtwo files, have positive rake angles and non-cutting tips.[11,15,17] These characteristics of Mtwo instruments, in addition to their S-shaped cross-section, are responsible for their cutting efficiency,[15] their lower risk of instrument fracture and their ability to achieve symmetrical root canals.[12] Moreover, the use of an electric torque-limited handpiece also reduces file fractures.[13]
In all three experimental groups, cleaning capacity was apparently better in the coronal and middle thirds of the canal than in the apical third. Like us, Foschi et al., also reported that none of the manual or rotary systems could clean the apical part of root canals completely.[11] In the present study the ProTaper system was less effective in the apical third than in the other two thirds of the canal. However, manual K-files were similarly effective in all three parts of the canal, as were Mtwo rotary files. This result reflects the better cutting ability and high flexibility of Mtwo rotary files, which cleaned the narrow, curved primary root canals efficiently. Several previous studies noted the advantages of Mtwo files over ProTaper systems in permanent teeth, e.g., fewer preparation errors, simplified technique and usage, and significantly shorter preparation times.[15,18,26,29] Because no data are available regarding the superiority of any given type of file in cleaning root canals in deciduous teeth, further research is recommended to evaluate the effectiveness of different kinds of rotary systems in primary teeth.
CONCLUSIONS
Based on our findings, the following conclusions can be offered:
New-generation endodontic instruments available for root canal preparation can facilitate canal preparation in primary teeth.
Manual K-files were similar in effectiveness to Mtwo and ProTaper rotary systems in cleaning primary tooth root canals.
ACKNOWLEDGEMENTS
The authors thank the Vice Chancellery of Shiraz University of Medical Science, for supporting the research (Grant # 87-4003). The article is based on the thesis by Dr. Mokhtare and Dr. Nikaein. Also the authors thank Dr. M Vossoughi from the Center for Development of Clinical Research, Namazee Hospital, for the statistical analysis, and, K. Shashok (AuthorAID in the Eastern Mediterranean) for help in language editing the manuscript.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Pinkham JR, Casamassimo PS. 4th ed. Philadelphia, PA: WB Saunders Co; 2005. Pediatric dentistry: Infancy through adolescence; p. 390. [Google Scholar]
- 2.Barr ES, Kleier DJ, Barr NV. Use of nickel-titanium rotary files for root canal preparation in primary teeth. Pediatr Dent. 2000;22:77–8. [PubMed] [Google Scholar]
- 3.Silva LA, Leonardo MR, Nelson-Filho P, Tanomaru JM. Comparison of rotary and manual instrumentation techniques on cleaning capacity and instrumentation time in deciduous molars. J Dent Child. 2004;71:45–7. [PubMed] [Google Scholar]
- 4.Crespo S, Cortes O, Garcia C, Perez L. Comparison between rotary and manual instrumentation in primary teeth. J Clin Pediatr Dent. 2008;32:295–8. doi: 10.17796/jcpd.32.4.l57l36355u606576. [DOI] [PubMed] [Google Scholar]
- 5.Guelzow A, Stamm O, Martus P, Kielbassa A. Comparative study of six rotary nickel-titanium systems and hand instrumentation for root canal preparation. Int Endod J. 2005;38:743–52. doi: 10.1111/j.1365-2591.2005.01010.x. [DOI] [PubMed] [Google Scholar]
- 6.Kuo C, Wang Y, Chang H, Huang G, Lin C, Li U, et al. Application of Ni-Ti rotary files for pulpectomy in primary molars. J Dent Sci. 2006;1:10–5. [Google Scholar]
- 7.Kim HC, Kim HJ, Lee CJ, Kim BM, Park JK, Versluis A. Mechanical response of nickel-titanium instruments with different cross-sectional designs during shaping of simulated curved canals. Int Endod J. 2009;42:593–602. doi: 10.1111/j.1365-2591.2009.01553.x. [DOI] [PubMed] [Google Scholar]
- 8.Nagaratna PJ, Shashikiran ND, Subbareddy VV. In vitro comparison of NiTi rotary instruments and stainless steel hand instruments in root canal preparations of primary and permanent molar. J Indian Soc Pedod Prev Dent. 2006;24:186–91. doi: 10.4103/0970-4388.28075. [DOI] [PubMed] [Google Scholar]
- 9.Soares F, Varella CH, Pileggi R, Adewumi A, Guelmann M. Impact of Er,Cr: YSGG laser therapy on the cleanliness of the root canal walls of primary teeth. J Endod. 2008;34:474–7. doi: 10.1016/j.joen.2008.02.006. [DOI] [PubMed] [Google Scholar]
- 10.Sleiman P, Abou-Jaoude S, Berberi R. The use of the K3 orifice openers in primary teeth preparation. Oral Health. 2007;97:17–8. [Google Scholar]
- 11.Foschi F, Nucci C, Montebugnoli L, Marchionni S, Breschi L, Malagnino VA, et al. SEM evaluation of canal wall dentine following use of Mtwo and ProTaper NiTi rotary instruments. Int Endod J. 2004;37:832–9. doi: 10.1111/j.1365-2591.2004.00887.x. [DOI] [PubMed] [Google Scholar]
- 12.Veltri M, Mollo A, Mantovani L, Pini P, Balleri P, Grandini S. A comparative study of Endoflare-Hero Shaper and Mtwo NiTi instruments in the preparation of curved root canals. Int Endod J. 2005;38:610–6. doi: 10.1111/j.1365-2591.2005.00989.x. [DOI] [PubMed] [Google Scholar]
- 13.Schäfer E, Erler M, Dammaschke T. Comparative study on the shaping ability and cleaning efficiency of rotary Mtwo instruments. Part a. Shaping ability in simulated curved canals. Int Endod J. 2006;39:196–202. doi: 10.1111/j.1365-2591.2006.01074.x. [DOI] [PubMed] [Google Scholar]
- 14.Schäfer E, Erler M, Dammaschke T. Comparative study on the shaping ability and cleaning efficiency of rotary Mtwo instruments. Part b. Cleaning effectiveness and shaping ability in severely curved root canals of extracted teeth. Int Endod J. 2006;39:203–12. doi: 10.1111/j.1365-2591.2006.01075.x. [DOI] [PubMed] [Google Scholar]
- 15.Malagino VA, Grande NM, Plotino G, Somma F. The Mtwo NiTi rotary system for root canal preparation. [Last cited on 2012 Apr 4]. Available from: www.vdw-dental.com/pdf/presse/RO0306_59-62_Malagino.pdf .
- 16.The next progression in proficient performance. [last cited on 2012 Apr 4]. Available from: http://store.maillefer.com/lit2/pdfs/ProTaperBrochure_web.pdf .
- 17.Clauder T, Baumann MA. Protaper Nt system. Dent Clin North Am. 2004;48:87–111. doi: 10.1016/j.cden.2003.10.006. [DOI] [PubMed] [Google Scholar]
- 18.Giovannone T, Migliau G, Bedini R, Ferrari M, Gallottini L. Shaping outcomes using two Ni-Ti rotary instruments in simulated canals. Minerva Stomatol. 2008;57:143–54. [PubMed] [Google Scholar]
- 19.Gu YX, Zhu YQ, Du R. A comparative study of three different rotary NiTi systems in the preparation of curved molar canals. Shanghai Kou Qiang Yi Xue. 2009;18:147–51. [PubMed] [Google Scholar]
- 20.Schäfer E, Florek H. Efficiency of rotary nickel-titanium K3 instruments compared with stainless steel hand K-Flexofile. Part a. Shaping ability in simulated curved canals. Int Endod J. 2003;36:199–207. doi: 10.1046/j.1365-2591.2003.00643.x. [DOI] [PubMed] [Google Scholar]
- 21.Sonntag D, Ott M, Kook K, Stachniss V. Root canal preparation with the NiTi systems K3, Mtwo and ProTaper. Aust Endod J. 2007;33:73–81. doi: 10.1111/j.1747-4477.2007.00062.x. [DOI] [PubMed] [Google Scholar]
- 22.Schäfer E, Zapke K. A comparative scanning electron microscopic investigation of the efficacy of manual and automated instrumentation of root canals. Int Endod J. 2000;26:660–4. doi: 10.1097/00004770-200011000-00007. [DOI] [PubMed] [Google Scholar]
- 23.Barbizam JV, Fariniuk LF, Marchesan MA, Pecora JD, Sousa-Neto MD. Effectiveness of manual and rotary instrumentation techniques for cleaning flattened root canals. J Endod. 2002;28:365–6. doi: 10.1097/00004770-200205000-00004. [DOI] [PubMed] [Google Scholar]
- 24.Schäfer E, Schlingemann R. Efficiency of rotary nickel-titanium K3 instruments compared with stainless steel hand K-Flexofile. Part b. Cleaning effectiveness and shaping ability in severely curved root canals of extracted teeth. Int Endod J. 2003;36:208–17. doi: 10.1046/j.1365-2591.2003.00644.x. [DOI] [PubMed] [Google Scholar]
- 25.Sipert C, Hussne R, Nishiyama C. Comparison of the cleaning efficacy of the FKG race system and hand instrument in molar root canal. J Appl Oral Sci. 2006;14:6–9. doi: 10.1590/S1678-77572006000100002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Kuzekanani M, Walsh L, Yousefi MA. Cleaning and shaping curved root canals: Mtwo vs Protaper instruments, a lab comparison. Indian J Dent Res. 2009;20:268–70. doi: 10.4103/0970-9290.57355. [DOI] [PubMed] [Google Scholar]
- 27.Taşdemir T, Er K, Yildirim T, Buruk K, Celik D, Cora S, et al. Comparison of the sealing ability of three filling techniques in canals shaped with two different rotary systems: A bacterial leakage study. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009;108:e129–34. doi: 10.1016/j.tripleo.2009.05.007. [DOI] [PubMed] [Google Scholar]
- 28.Kummer TR, Calvo MC, Cordeiro MM, de Sousa Vieira R, de Carvalho Rocha MJ. Ex vivo study of manual and rotary instrumentation techniques in human primary teeth. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2008;105:e84–92. doi: 10.1016/j.tripleo.2007.12.008. [DOI] [PubMed] [Google Scholar]
- 29.Vahid A, Roohi N, Zayeri F. A comparative study of four rotary NiTi instruments in preserving canal curvature, preparation time and change of working length. Aust Endod J. 2009;35:93–7. doi: 10.1111/j.1747-4477.2008.00135.x. [DOI] [PubMed] [Google Scholar]