

Abstract
Background:
The aim of the present study is to determine the number of third molars per person, angulation, level, amount of space for eruption of third molar between ramus of mandible and second molar and the eruption status of third molar in a group of Libyan students, with different impaction patterns and agenesis of third molars.
Materials and Methods:
In this descriptive retrospective study, a total of 200 students (100 male and 100 female students of bachelor of dental surgery, Faculty of Dentistry, Garyounis University, Benghazi, Libya) were enrolled. Students who had complete complement of teeth within the age group 17–26 years were selected for this study, while those cases who had history of extraction of any of the teeth or who refused to give consent were excluded. Before starting the study, ethical concern from the ethical committee, IRB and informed consent from each student who underwent radiography were obtained.
Results:
The results showed that 5% of third molars were congenitally missing. Approximately 93.5% of the subjects had all four third molars, 1% had two third molars and 0.5% had one third molars with 2.5% having agenesis of all third molars. Third molar agenesis showed predilection for maxilla with higher proportion in females (3%) than males (2.1%). Angular position was maximum with vertical position (5.83%), with least being horizontal impactions. Level of occlusal plane of third molar similar to that of adjacent tooth was seen in 44.74%, below the occlusal plane in 24.76%, totally impacted noted in 30%.
Conclusion:
The present study showed that 33% of the teeth were fully erupted and 66% were in various stages of eruption and 5% were congenitally missing in these students.
Keywords: Dental, epidemiology, impacted molar, prevalence
INTRODUCTION
The third molars are the last teeth to erupt in all races despite racial variations in the eruption sequence. This late eruption is responsible for the third molar being the most frequently impacted tooth. Facial growth, jaw size, and tooth size differ among different races and population groups and exhibit definite inheritance patterns. Racial variation in facial growth, jaw size, and tooth size is crucial to the eruption pattern, impaction status and incidence of agenesis of third molars.[1] The cause of agenesis of one or more teeth is still unknown, but several reasons such as physical disruption of the dental lamina, space limitation, and an inherent defect of the dental lamina, or failure of induction of the underlying mesenchyme have been suggested.[2]
To date, no information is documented regarding the pattern of third molar eruption status in the Libyans. The aim of the present study is to determine the number of third molar per person, angulation, level, amount of space for eruption of third molar between ramus of mandible and second molar.
MATERIALS AND METHODS
A total of 200 students (100 males and 100 females) who were in various phases of bachelor of dental surgery (between the age group of 17–26 years) volunteered to get enrolled in the study. The duration of the study was 3 months. All students were examined in the department of Oral medicine, diagnosis and radiology at Faculty of Dentistry, Garyounis University, Benghazi, Libya. Before starting the study, ethics approval was obtained from the Garyounis University ethical committee. The details regarding the study were explained for each of the student and informed consent was taken. Among a total of 1240 students, only those students who had full complement of teeth (did not give any history of extraction due to impaction or orthodontia or caries) were included. Exclusion criteria were those cases who had history of extraction of any of the teeth or who refused to give consent. To avoid bias, all the students were examined by two well-trained dentists and intra and interobserver kappa correlation ranged from 0.8 to 0.76.
Based upon the feasibility of the students and the examiner, each student underwent thorough examination of the third molar region. On an average, five students per day were examined.
All students were examined clinically to see the status of third molar and based upon their clinical status they were classified as completely erupted, partially erupted and unerupted. The eruption status was assessed by using visual method and with the help of probe. The teeth which were partially erupted and unerupted were subjected for radiographic examination. Each student after clinical examination was subjected for panoramic radiography. The standard OPG machine (PANARAY PC- 1000 with 70-90 KvP and 6-100 mA) was used. The teeth radiographically noted are divided as mesioangular, distoangular, vertical and horizontal impactions. The following parameters were also considered: Number of impacted tooth per person, incidence of angulation, level of eruption, space of eruption of third molar.
Angulation
The angulation of the mandibular third molars was determined on the panoramic radiographs by drawing a line through the midpoint of the occlusal surface and bifurcation of the second molar and the third molar. These lines represent the long axes of the teeth. The angle formed between the intersected long axes gave either a mesial or distal inclination of third molar in relation to second molar. The inclination for vertical was +10° to –10°, mesioangular +11° to +79°, distoangular –11° to 79°. The inclination angle was then read in increments of 5° to a maximum of 65°, above which the tooth was considered to be horizontally impacted.
Level of eruption
Level of eruption was grouped as level A, where the occlusal plane of the third molar was on the same level or above the occlusal plane of adjacent second molar. In level B, the occlusal plane was below the occlusal plane but above the cervical line of the second molar. In level C, the occlusal plane was beneath the cervical line of the second molar.
Third molar space
Third molar space was measured as the distance between the distal surface of second molar crown and anterior border of the ramus on the occlusal plane in proportion to the width of third molar crown.[3]
RESULTS
The collected data were analyzed by Chi-square test, t test and analysis of variance approach.
The mean age of the study group was 21.5 years (±2.9). The number of third molars found in 200 subjects was 760; 381 teeth were in the upper jaw and 379 teeth in the lower jaw. The proportion of third molar agenesis was around 5% (40 of total 800 teeth).
Table 1 shows 93.5% subjects had all four third molars, 2.5% had three third molars, and 1% had two third molars, 1% had one third molar. Only 2.5% of the subjects had agenesis of all third molars.
Table 1.
Total number of molars per person
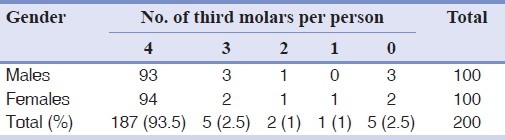
Table 2 shows the angulation of maxillary and mandibular third molars. The mandibular third molars showed a higher frequency of mesial inclination (41.68%), followed by vertical (38.25%), with distal inclination of (13.45%), and followed by horizontal inclination (6.29%). The angulation of upper jaw showed a higher frequency of vertical angulations (72.17%), followed by distoangular (22.04%), with mesioangulation third in frequency (5.77%).
Table 2.
Angular position of mandibular and maxillary third molars

The mean and SD values of vertically, mesially, and distally tilted third molars of the right and left side in both of the jaws were calculated. Each of the 3 sets of data was subjected to one-way analysis of variance (ANOVA) with 2 factors: A, upper versus lower jaw, and B, right versus left. In the vertical group, the third molar angulation averaged 5.41° (±2.8°) in the mandible and 7.13° (±2.3°) in the maxilla; the difference was highly significant (P<0.01).
However, the third molar angulation averaged 6.31° (±2.64°) on the right side and 6.01° (±2.6°) on the left side in both jaws; the difference was statistically nonsignificant. The inclination angle of mesially tilted third molars averaged 25.41° (±8.28°) in the mandible and 26.31° (±15.28°) in the maxilla; the difference was statistically non significant. Similarly the difference between the right side [(26.91° (±12.8°)] and left side [27.41° (±8.18°)] in both jaws was nonsignificant. The angle of distally inclined third molar averaged 15.41° (±2.8°) in the mandible and 18.18° (±4.8°) in the maxilla; this difference was significant at a level of P<0.05. However, the difference between the right and left teeth in both jaws was statistically significant. Pearson's correlation coefficient was computed to find the relationship between right and left inclination angles in both jaws. A highly significant correlation in the mandible (r=0.543); P<0.01) and maxilla (r=0.643); P<0.01) was obtained.
Table 3 shows the level of eruption of third molars in the maxilla and mandible. Of the 751 teeth, 336 (44.74%) were positioned with their occlusal surfaces on the same level or above the occlusal plane of adjacent second molar (level A). The maxilla is the predominant site in 173 teeth (46.5%) over the mandible 163 teeth (43%). Level B eruption was the least frequent in occurrence among the other levels of eruption. Level B eruption showed a higher frequency in maxilla 95 teeth (25.53%) than in the mandible 91 teeth (24%). Two hundred and twenty nine third molars (30.49%) were erupted to level C. A Chi-square test was applied to find the presence or association if any, between eruption levels of third molar in the upper and lower jaw. As per analysis [Table 2], the computed value of Chi-square test (95.3; Pearson coefficient of contingency (=0.39) turned out to be highly significant (P<0.02); at A and B levels. The proportions of third molar in upper jaw were smaller than those of mandible, whereas at level C, the pattern was just the opposite. Similarly, at each of the 3levels of eruption, the proportion of male cases was significantly higher than that of female cases [Table 3]. However, no association could be detected between the levels of eruption and sex of the patients (computed Chi-square test=0.1, critical Chi-square test=4.9).
Table 3.
Level of eruption of maxillary and mandibular third molars
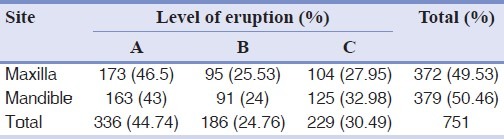
Table 4 describes the level of eruption in both males and females. Females demonstrate a higher frequency (20%) of level A eruption than males. Males had 9.4% more third molar at Level B eruption than females. Females 118 teeth (31.29%) had higher level C frequency than males 111 (29.67%). This was statistically significant where Chi-square test was applied (computed Chi-square test value and critical Chi-square test found no association between level of eruption but association was found with sex of the patient.
Table 4.
Level of eruption of third molars in males and females
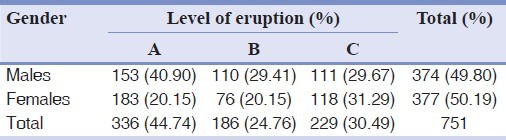
Table 5 shows the occurrence of different angulations of impaction in male and female students. Vertical angulation was the common, with horizontal angulation being the least common.
Table 5.
Distribution of angulation of impaction in third molar
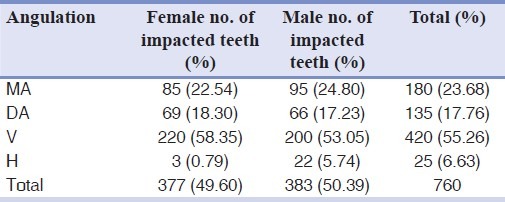
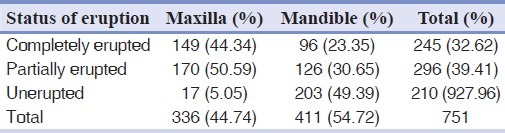
Table 6 shows the status of eruption of maxillary and mandibular third molars in which 32.6% of teeth were completely erupted, 39.4% of them were partially erupted and unerupted teeth were 27.9%.
Table 6.
Status of eruption of maxillary and mandibular third molars
DISCUSSION
Third molars are most often congenitally missing. As racial variation, nature of diet, degree of use of masticatory apparatus, and genetic inheritance can affect the jaw size and tooth size, studies of prevalence and incidence of impacted third molars have been carried out on different population groups.[4–11]
In our study, about 33% of the teeth were found to be completely erupted and remaining 66% of the teeth were in various stages of eruption. In Sandhu et al.'s[5] study, 24% of the teeth were found to be erupted and 76% were in various stages of eruption.
The mean age of our study group was 21.58 years (±2.9079 std deviation), Hellman[12] reported a mean age for eruption as 20.5 years among Americans. In African races, the period of eruption ranges from 13 to 20 years. Fanning[11] found the median age of eruption to be 19.8 years in men and 20.4 years in women among Bostonians. Sandhu et al.[5] Quek[13] and Schersten et al.[7] study have shown mean age of their subjects as 19.3, 26.5±5 and 20 to 25 years, respectively.
The proportion of students having all 4 third molars was higher (93.5%) than a study by Sandu[5] (76%) in Indian population and Hattab[6] (73%) in Jordanians.
Our observation showed that incidence of congenitally missing third molars was 5% which is lower than the data reported by Sandhu et al.[5] (11.5%), Levesque et al.[14] for French Canadians (9%), Hattab[6] for Jordanians (9.1%), Gorgani et al.[15] for Americans, Venta et al.[16] for Finnish students (12%) and Kruger et al.[12] for New Zealand population (15.2%).
In the present study conducted on Libyan students, 2.5% had agenesis of all third molars, which is slightly higher than the results obtained from Hattab et al.[6] (1.7%) and Hugoson and Kugelberg,[11] on Swedish population (2%). But our observation is considerably less than that for the Scandanavian population (10% to 13%)[7,17,18] and Americans (7% to 10%).[15]
The proportion of agenesis of third molars for Libyan females (3%) was higher than males (2.1%) which were similar to the findings of Sandhu et al.[5] {where Indian females showed 12.8% and males 8.3%}, Hellman et al.[12] and Shah et al.[19] but differ from those of Levesque et al.[14] Gorgani et al.[15] and Hattab et al.[6]
Our results show that mandibular agenesis was more common than the maxillary, which differ with the results of previous studies.[5,6,18,20,21]
There was no equal distribution between right and left side as noted by Hattab, Hellman,[12] Granen[18] and Shah et al.[19] Results of our study showed that about three quarters of the subjects had all four third molars, which was similar to the results obtained by Hattab et al.[6] and Sumeeth sandhu et al.[5] But this proportion was higher compared with the findings of Hellman[12] on American students and Schersten et al.[7] on Scandanavians, who also noted that one half of the persons had all four third molars.
Our results showed differences in both male and female group, which was statistically significant (Chi-square test), which was in agreement with the results obtained from Hellman[12] Schersten,[7] but differ from Hattab,[6] Dachi and Howell.[21]
The order of frequency for missing teeth in the present study is 1 (1 subjects), 2 (2 Subjects), 3 (5 subjects), 4 (187 subjects) which were in accordance with the findings of Hattab et al.[6] and Nanda and Kruger et al.,[9] but differ from Banks[11] (where it is most common for 2 third molar to be missing, followed by 1, 4 and 3.
In the Libyan students with a mean age of 21.5 years, 30% of the third molars were unerupted (Level C of eruption). This finding is in agreement with Sumeeth sandhu et al.[5] (34% mean age 19.3 years), also with Bjork[17] and Venta[22] (between 22.3% and 66.6%, with age between 19.5 and 20.5 years).
Table 6 shows that mandible had a higher frequency of unerupted teeth (49.39%) than the maxilla (5.05%). These findings were in agreement with Kruger et al.[9] (age, 18 years), and differs from Sandhu et al.[5] (mean age 19.3 years), Hattab[6] (Mean age 20.4 years) and Venta et al.[23] (age 20 years).
In this study, 32.62% of third molars were fully erupted, this value is close to Venta et al.[16] ((35%) but more than that reported by Sandhu et al.[5] (24%), Kruger et al.,[9] (17%) and less than that reported by Hattab et al.[6] (11) (58%); Odusanya et al.[1] (1) (100%).
In this study, 41.68% of the mandibular third molars were found to be in the mesioangular position. This number is close to the observations by Sandhu et al.[5] (49%), Hattab et al.[6] and Richardson.[24] This number is considerably higher than that reported by Sewerin and Wowern[25] (18%) and less in proportion to that noted by Kruger et al.[9] (62.9%), Richardson[24] and Venta et al.[23] (71%).
Our observation that 38.25% of the lower third molar was in vertical position is close to the findings of Hattab et al.[6] and Kruger et al.[9] and Venta et al.[23] and less than the finding of Sandhu et al.[5] (42%).
The frequency of distoangular mandibular third molar in the present study (13.45%) is more compared with the findings of Sandhu et al.,[5] Hattab et al.,[6] Kruger et al.[9] and Venta et al.[23]
The present study showed that 22.04% of the maxillary third molars were in the distoangular position. This value is similar to the results obtained from Venta et al.[23] (23%), but less than the results reported by Sumeeet Sandhu et al.[5] (48%) but higher than that by Kruger et al.[9] (12.2%).
Our observation that 72.17% of maxillary third molars were in the vertical position is also more compared with the findings of Sandhu et al.[5] (43%), Venta et al.[23] (54%), and Kruger et al.[9] (18.1%).
The frequency of mesioangular maxillary third molars 5.77% is less than that reported by Venta et al.,[23] Kruger et al.[9] and Sandhu[5] (10) (9%).
CONCLUSION
The present study showed that 33% of the teeth were fully erupted and 66% were in various stages of eruption and 5% were congenitally missing in these students.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Odusanya SA, Abayomi IO. Third molar eruption among rural Nigerians. Oral Surg Oral Med Oral Pathol. 1991;71:151–4. doi: 10.1016/0030-4220(91)90457-n. [DOI] [PubMed] [Google Scholar]
- 2.Stewart RE, Barber TK, Thoutman KC, Wei SH. 1st ed. St. Louis: CV Mosby; 1982. Pediatric dentistry: Scientific foundation and clinical practice; p. 91. [Google Scholar]
- 3.Andreasen JO, Petersen JK, Laskin DM. Copenhagen: Munksgaard; 1997. Textbook and color atlas of tooth impactions; pp. 223–3. [Google Scholar]
- 4.Alling CC, Helfrick JF, Alling RD. 2nd ed. Philadelphia: WB Saunders; 1993. Impacted teeth; p. 46. [Google Scholar]
- 5.Sandhu S, Kaur T. Radiographic evaluation of the status of third molars in the Asian Indian students. J Oral Maxillofac Surg. 2005;63:640–5. doi: 10.1016/j.joms.2004.12.014. [DOI] [PubMed] [Google Scholar]
- 6.Hattab FN, Fahmy MS, Rawashdehma MA. Impaction status of third molars in Jordanian students. Oral Surg Oral Med Oral Pathol Radiol Endod. 1995;79:24–9. doi: 10.1016/s1079-2104(05)80068-x. [DOI] [PubMed] [Google Scholar]
- 7.Schersten E, Lysell L, Rohlin M. Prevalence of impacted third molars in dental students. Swed Dent J. 1989;13:7–13. [PubMed] [Google Scholar]
- 8.Fanning EA. Third molar in Bostonians. Am J Phys Anthropol. 1962;20:151–55. [Google Scholar]
- 9.Kruger E, Thomson WM, Konthasinghe P. Third molar outcomes from age 18 to 26: Findings from a population-based New Zealand longitudinal study. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2001;95:150–5. doi: 10.1067/moe.2001.115461. [DOI] [PubMed] [Google Scholar]
- 10.Haidar Z, Shalhoub SY. The incidence of impacted wisdom teeth in a Saudi community. Int J Oral Maxillofac Surg. 1986;15:569–71. doi: 10.1016/s0300-9785(86)80060-6. [DOI] [PubMed] [Google Scholar]
- 11.Hugoson A, Kugelberg CF. The prevalence of third molars in a Swedish population: An epidemiological study. Community Dent Health. 1988;5:121–38. [PubMed] [Google Scholar]
- 12.Hellman M. Our Third Molar Teeth; Their Eruption, Presence and Absence. Dent Cosmos. 1936;78:750–62. [Google Scholar]
- 13.Quek SL, Tray CK, Tay KH, Toh SL, Lim KC. Pattern of third molar impaction in a Singapore Chinese population: A retrospective radiographic survey. Int J Oral Maxillofac Surg. 2003;32:548–52. [PubMed] [Google Scholar]
- 14.Levesque GY, Demirjian A, Tanguay R. Sexual dimorphism in the development, emergence, and agenesis of the mandibular third molar. J Dent Res. 1981;60:1735–41. doi: 10.1177/00220345810600100201. [DOI] [PubMed] [Google Scholar]
- 15.Gorgani N, Sullivan RE, DuBois L. A radiographic investigation of third-molar development. J Dent Child. 1990;57:106–10. [PubMed] [Google Scholar]
- 16.Venta I, Turtola L, Ylipaavalniemi P. Changes in clinical status of third molars in adults during 12 years of observation. J Oral Maxillofac Surg. 1999;57:386–9. doi: 10.1016/s0278-2391(99)90273-2. discussion 389-91. [DOI] [PubMed] [Google Scholar]
- 17.Bjork A, Jensen E, Palling M. Mandibular growth and third molar impaction. Acta Odontol Scand. 1956;14:231–72. [Google Scholar]
- 18.Grahnen H. Hypodontia in the permanent dentition. Odont Revy. 1956;7:l–100. [PubMed] [Google Scholar]
- 19.Shah RM, Boyd MA, Vakil TF. Studies of permanent tooth anomalies in 7886 Canadian individuals. J Can Dent Assoc. 1978;44:262–4. [PubMed] [Google Scholar]
- 20.Mead SV. Incidence of impacted teeth. Int J Orthod. 1930;16:885–90. [Google Scholar]
- 21.Dachi SF, Howell FV. A survey of 3874 routine full-mouth radiographs. II. A study of impacted teeth. Oral Surg Oral Med Oral Pathol. 1961;14:165–9. doi: 10.1016/0030-4220(61)90003-2. [DOI] [PubMed] [Google Scholar]
- 22.Venta I, Murtomaa H, Turtola L, Meurman J, Ylipaavalniemi P. Clinical follow up study of third molar eruption from ages 20 to 26 years. Oral Surg Oral Med Oral Pathol. 1991;72:150–3. doi: 10.1016/0030-4220(91)90154-5. [DOI] [PubMed] [Google Scholar]
- 23.Venta I, Turtola L, Ylipaavalniemi P. Radiographic follow up of impacted third molars in young adults from age 20 to 32 years. Int J Oral Maxillofac Surg. 2001;30:54–7. doi: 10.1054/ijom.2000.0002. [DOI] [PubMed] [Google Scholar]
- 24.Richardson M. Changes in lower third molar position in the young adult. Am J Orthod Dentofacial Orthop. 1992;102:320–7. doi: 10.1016/0889-5406(92)70047-E. [DOI] [PubMed] [Google Scholar]
- 25.Sewetin I, Von Wowern N. A radiographic four – year follow –up study of asymptomatic mandibular third molars in young adults. Int Dent J. 1990;40:24–30. [PubMed] [Google Scholar]