

Abstract
Background:
This study was designed to evaluate the correlation between subjective data obtained from a questionnaire and clinical examination among students in Shiraz university of medical sciences.
Materials and Methods:
In this cross-sectional prospective study, the samples consisted of 200 subjects, with equal distribution between males and females. Subjects’ ages ranged from 18 to 30 years (24.07±2.93). A functional evaluation was performed using the Helkimo clinical dysfunction (Di) and anamnestic (Ai) indices. Data were evaluated by the Chi-square test between gender and clinical dysfunction index (Di) and correlation coefficient between Di and Ai (the level of significance was set at P<0.05).
Results:
Among the total study population, 30% reported mild symptoms (Ai I) while 2% had severe (Ai II). In the clinical examination, 71% showed some degree of dysfunction. These degrees were as follows: 50% were classified as mild (Di I), 13% moderate (Di II) and 8% severe signs and symptoms (Di III).
With respect to gender, women (80%) were more affected than men (62%). A significant relationship was found between gender and the occurrence of temporomandibular disorder (TMD) (P<0.05). The correlation coefficient (r) between the reported symptoms (Ai) and recorded signs (Di) was 0.53. There were positive correlation coefficient between Di and Ai. They were statistically significant (P<0.001).
Conclusions:
A high prevalence of signs and symptoms of TMD among students in Shiraz University of Medical Sciences was seen, which was greater in women. Despite suffering from TMD, students were not aware of their disorders.
Keywords: Anamnestic dysfunction index, clinical dysfunction index, temporomandibular dysfunction
INTRODUCTION
Temporomandibular joint (TMJ) function has been the subject of considerable study for over a century, and despite voluminous literature, the multifactorial etiology of TM dysfunction is even today a cryptic issue.[1] Reports have shown that signs and symptoms of temporomandibular disorder (TMD) increase with age;[2] however, other studies have shown a decrease in symptoms with increasing age.[3] Over a 20 years period, investigations on TMD have revealed predominately mild signs and symptoms already present in childhood. An increase in symptoms occurs until young adulthood, after which they level out.[4] The concept of TMD may be attributable to specific genes that are inheritable.[5] In epidemiological studies of TMD, Helkimo found that prevalence between 12 and 57% for anamnestic symptoms and between 28 and 88% for clinical signs.[6] However, some studies have been conducted in other parts of the world, for example in the African continent, Abdel-Hakim[7] reported in an Egyptian sample that more than 24% had anamnestic symptoms and that more than 39% had clinical signs. Mazengo[8] found in randomly selected adult Tanzanians, a prevalence of 26% reported symptoms and 40% clinical signs. In Asia, Shiau[9] reported that 43% of Taiwanese university students had a prevalence of one or more signs of TMD. Jagger[10] found that more than 19% had anamnestic symptoms and that over 36% showed clinical sign in university students. The lack of standardized criteria in the evaluation of TMD, however, makes comparison between different studies difficult. This problem was addressed by Helkimo[11] in 1974 and was the basis for the development of his anamnestic (reported) and clinical dysfunction index which probably still remains the most widely applied system in epidemiological studies of TMD. Prevalence and severity of TMD studies should provide a health care need in the population studied. It is therefore important and valuable to have epidemiological data to estimate the proportion and distribution of these disorders in the population. The aim of this study was to evaluate the prevalence of temporomandibular dysfunction in university students of both sexes through the analysis of the subjective and objective data obtained from a questionnaire and clinical examination, and correlation between anamnestic and clinical dysfunction index.
MATERIALS AND METHODS
This cross-sectional, prospective clinical survey was conducted through a questionnaire and clinical examination. Written consent form was taken and the subjects participated for this study voluntarily. The samples comprised of 200 university students, with equal gender distribution who attended Shiraz University of Medical Sciences in Iran.
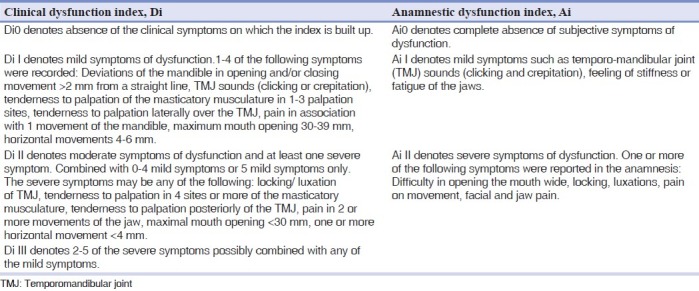
Students whose ages ranged from 18 to 30 years (24.07±2.93) with no history of systemic, musculoskeletal or neurological disorders were enrolled. Subjects were on no medications. Subject selection was based on the following criteria: Good periodontal health and absence of active caries or lesions, the presence of a full complement of permanent teeth with or without the third molar and no history of orthodontic treatment. All individuals were subjected to anamnestic and clinical examinations according to Helkimo.[11] The anamnestic examination was based on the reported symptoms by the students and classified according to anamnestic dysfunction index (Ai) as 0, I, II. A summary is given in Table 1.
Table 1.
Evaluation of clinical and anamnestic dysfunction according to Helkimo index
Clinical examination was preformed twice by one examiner previously trained and calibrated in the use of the index.
Depending on the clinical dysfunction score (CDS) following clinical examination, each student was classified as having a clinical dysfunction index (Di) of 0 (0 points, no signs and symptoms), Di I (1-4 points, mild TMD), Di II (5-9 points, moderate TMD) and Di III (10-25 points, severe TMD). Examination results were recorded on standardized charts according to Helkimo. The anamnestic examination was based on reported symptoms by the students and classified according to anamnestic dysfunction index (Ai) as I, II. Chi-square test was used to compare sex differences and clinical dysfunction index. Correlation coefficient was calculated between the anamnestic and clinical dysfunction index. (Ai, Di). P value less than 0.05 was considered statistically significant, and a correlation coefficient more than 0.4 was considered acceptable based on the results of previous studies.[12]
RESULTS
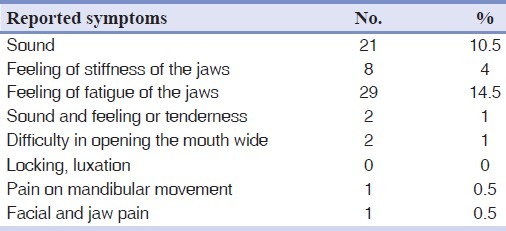
According to anamnestic dysfunction index, 68% reported no symptoms (Ai0), 30% had mild symptoms (Ai I), and 2% suffered from severe symptoms (Ai II). In clinical dysfunction index, 29% of subjects showed no signs of dysfunction (Di0), whereas 71% were positive for some degrees of dysfunction (Di): 50% had mild (Di I), 13% exhibited moderate dysfunction (Di II), while 8% suffered severe dysfunction (Di III). Feeling of fatigue (14.5%) and TMJ sounds (10.5%) were the most common anamnestic symptoms reported [Table 2]. Overall clinical examinations reveal that the prevalence of TMD exceeds the reported issues.
Table 2.
Distribution of Helkimo anamnestic (Ai) symptoms in 200 university students
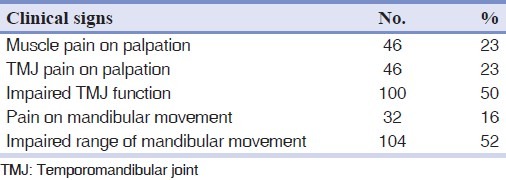
In the clinical examination, impaired range of mandibular movement (52%) and impaired TMJ function (50%) were most frequently observed in students compared to other signs and symptoms [Table 3].
Table 3.
Distribution of Helkimo dysfunction index (Di) in 200 university students
Chi-square test was used to compare sex differences and clinical dysfunction. Regarding gender versus dysfunction, 62% of male and 80% of female showed signs and symptom TMD (P<0.05), which indicate a significant difference between gender and dysfunction [Table 4]. The correlation coefficient (r) between the reported symptoms (Ai) and recorded signs (Di) was 0.53. This indicates that there was a positive linear correlation coefficient between Di and Ai and also indicates that they were statistically significant (P<0.001). Comparison of percentage distribution of the Helkimo anamnestic (Ai) and clinical dysfunction index (Di) in 200 Iranian university students is shown in Figure 1.
Table 4.
Percent and number of students with regard to dysfunction (Di) and gender (P=0.005)
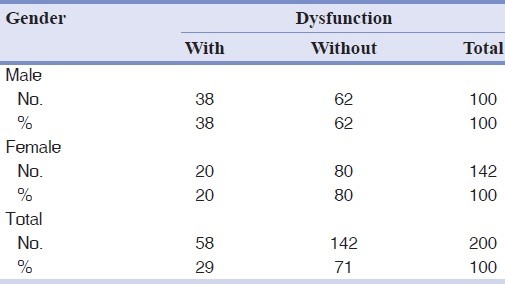
Figure 1.
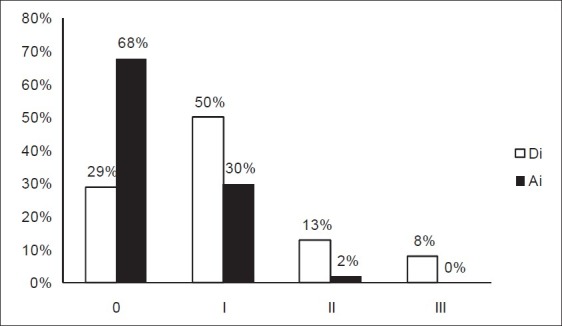
Comparison of percentage distribution of the Helkimo anamnestic (Ai) and clinical dysfunction index (Di) in 200 Iranian university students
DISCUSSION
The aim of this study was to evaluate the prevalence of signs and symptoms of TMD in university students in Shiraz University of Medical Sciences through the distribution of frequency of data obtained from a questionnaire and physical examination. According to clinical examination among the 200 students studied, a total of 71% showed some degree of TMD as follows: Mild (50%), moderate (13%) and severe (8%) clinically. The anamnestic index showed that 68% had no symptoms.
In this study, the prevalence of TMD in women (80%) was higher than men (62%). The prevalence of clinical dysfunction reported by Nourallah and Johansson[12] according to the Helkimo clinical dysfunction index was: Di 0 = 63%, Di I = 33%, Di II = 3% and Di III = 1% and anamnestic dysfunction index: Ai0 = 64%, AiI = 30%, Ai II = 6%. In their study, subjects were comprised of 105 dental students whose mean age was 23 years. Our results were dissimilar since this discrepancy may also be due to different racial, cultural and economic environments. Among TMD prevalence studies, Schiffman et al.[13] have performed a thorough TMD prevalence study of nursing students, with the use of a comprehensive questionnaire and clinical examination. In their study, 69% of subjects had positive TMD findings, which included muscle (23%) and joint disorders (19%). However, only 6% exhibited severe signs and symptoms and 34% of students would have been reported (anamnestic) with symptoms. In another study performed by Solberg et al.,[14] 65% of college students had one or more signs and symptoms of TMD. In our clinical study, 71% of all samples showed some degree of dysfunction (Di); 34% reported positive symptoms (Ai), 23% had joint pain and 23% muscle pain on palpation, which approximated the reports of Schiffman and Solberg.[13,14] In a study conducted by Nassif et al.[15] on university students with a mean age of 22.4 years, the overall results showed that 75% of subjects had TMD signs and symptoms of which 6.9% were mild, 51.4% moderate and 16.7% severe. In our study, 71% had some degree of dysfunction. Therefore, a comparison of the present results with the previous report which also involved university students has shown a similar prevalence of TMD. Studies have shown wide variations in the prevalence of clinical signs of TMD. Otuyemi[16] performed a study on university students with a mean age of 23 years which has shown mild, moderate and severe signs and symptoms of 46%, 16.5% and 0.3%, respectively, 26.3% of subject reported mild (Ai I) and 2.9% reported severe temporomandibular dysfunction (Ai II). No significant relationships were found between sex and dysfunction. The results of the present study indicated that a discrepancy exists between the two studies. In the study of Pedroni,[17] 68% of the subjects exhibited some degree of TMD. Their study was performed on 50 dental students, whose ages ranged from 19 to 25 years. In their study, women were more affected than men, which was in agreement with our findings.
In the study performed on university students (average age: 20 years) that has been reported by Nomura,[18] 53.21% of the students showed some degree of TMD: 35.78% mild, 11.93% moderate and 5.5% severe. Women were most affected, with 63.11% showing some degree of TMD when compared with 40.62% of men. The prevalence of moderate and severe TMD in our study closely approximated the result by Nomura. The high prevalence of women classified with some degree of TMD may be related to physiological differences of the female, such as hormonal variations, muscular structure and different characteristics of connective tissue.[17,18] Results of our study indicate that prevalence of TMD among Iranian university students were remarkable. Also there were significant differences between clinical and anamnestic dysfunction index. This means that most students did not know whether they had the disorder and what the prognosis were. This can be due to various reasons such as emotional and psychological stress during their educational lifetime, particularly the stress they encounter during university entrance exam. Further epidemiological studies must be done on prevalence of TMD in Iranian university students. Proper diagnosis and plan management strategies should be proposed for prevention and treatment. Because of high prevalence of signs and symptoms of TMD among university students, some therapeutic centers should be organized to screen, cure and train the students.
Due to the wide distribution of TMD among different populations, this concept requires additional investigation within different cultural, economic and educational environments.
In conclusion, the results from this study showed that among university students, 71% of all subjects revealed some degree of dysfunction (Di) by clinical examination while only 32% of students reported positive symptoms (Ai). There were a positive correlation between Di and Ai which means that with increase in Ai, Di increases. Women (80%) were more affected than men (62%).
ACKNOWLEDGEMENT
The authors wish to express their appreciation to the Research Council of College of Dentistry, Shiraz University of Medical Sciences for their support in clinical part of this study.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Wadhwa L, Utreja A, Tewari A. A study of clinical signs and symptoms of temporomandibular dysfunction in subjects with normal occlusion, untreated, and treated malocclusions. Am J Orthod Dentofacial Orthop. 1993;103:54–61. doi: 10.1016/0889-5406(93)70105-W. [DOI] [PubMed] [Google Scholar]
- 2.De Boever JA, Adriaens PA. Occlusal relationship in patients with pain-dysfunction symptoms in the temporomandibular joints. J Oral Rehabil. 1983;10:1–7. doi: 10.1111/j.1365-2842.1983.tb00093.x. [DOI] [PubMed] [Google Scholar]
- 3.Hiltunen K, Schmidt-Kaunisaho K, Nevalainen J, Närhi T, Ainamo A. Prevalence of signs of temporomandibular disorders among elderly inhabitants of Helsinki, Finland. Acta Odontol Scand. 1995;53:20–3. doi: 10.3109/00016359509005939. [DOI] [PubMed] [Google Scholar]
- 4.Magnusson T, Egermarki I, Carlsson GE. A prospective investigation over two decades on signs and symptoms of temporomandibular disorders and associated variables.A final summary. Acta Odontol Scand. 2005;63:99–109. doi: 10.1080/00016350510019739. [DOI] [PubMed] [Google Scholar]
- 5.Cairns BE. Pathophysiology of TMD pain–basic mechanisms and their implications for pharmacotherapy. J Oral Rehabil. 2010;37:391–410. doi: 10.1111/j.1365-2842.2010.02074.x. [DOI] [PubMed] [Google Scholar]
- 6.Egermark-Eriksson I, Carlsson GE, Magnusson T. A long-term epidemiologic study of the relationship between occlusal factors and mandibular dysfunction in children and adolescents. J Dent Res. 1987;66:67–71. doi: 10.1177/00220345870660011501. [DOI] [PubMed] [Google Scholar]
- 7.Abdel-Hakim AM. Stomatognathic dysfunction in the western desert of Egypt: An epidemiological survey. J Oral Rehabil. 1983;10:461–8. doi: 10.1111/j.1365-2842.1983.tb01468.x. [DOI] [PubMed] [Google Scholar]
- 8.Mazengo MC, Kirveskari P. Prevalence of craniomandibular disorders in adults of Ilala District, Dar-es-Salaam, Tanzania. J Oral Rehabil. 1991;18:569–74. doi: 10.1111/j.1365-2842.1991.tb00080.x. [DOI] [PubMed] [Google Scholar]
- 9.Shiau YY, Chang C. An epidemiological study of temporomandibular disorders in university students of Taiwan. Community Dent Oral Epidemiol. 1992;20:43–7. doi: 10.1111/j.1600-0528.1992.tb00672.x. [DOI] [PubMed] [Google Scholar]
- 10.Jagger RG, Wood C. Signs and symptoms of temporomandibular joint dysfunction in a Saudi Arabian population. J Oral Rehabil. 1992;19:353–9. doi: 10.1111/j.1365-2842.1992.tb01577.x. [DOI] [PubMed] [Google Scholar]
- 11.Droukas B, Lindée C, Carlsson GE. Relationship between occlusal factors and signs and symptoms of mandibular dysfunction.A clinical study of 48 dental students. Acta Odontol Scand. 1984;42:277–83. doi: 10.3109/00016358408993881. [DOI] [PubMed] [Google Scholar]
- 12.Nourallah H, Johansson A. Prevalence of signs and symptoms of temporomandibular disorders in a young male Saudi population. J Oral Rehabil. 1995;22:343–7. doi: 10.1111/j.1365-2842.1995.tb00783.x. [DOI] [PubMed] [Google Scholar]
- 13.Schiffman EL, Fricton JR, Haley DP, Shapiro BL. The prevalence and treatment needs of subjects with temporomandibular disorders. J Am Dent Assoc. 1990;120:295–303. doi: 10.14219/jada.archive.1990.0059. [DOI] [PubMed] [Google Scholar]
- 14.Solberg WK, Woo MW, Houston JB. Prevalence of mandibular dysfunction in young adults. J Am Dent Assoc. 1979;98:25–34. doi: 10.14219/jada.archive.1979.0008. [DOI] [PubMed] [Google Scholar]
- 15.Nassif NJ, Al-Salleeh F, Al-Admawi M. The prevalence and treatment needs of symptoms and signs of temporomandibular disorders among young adult males. J Oral Rehabil. 2003;30:944–50. doi: 10.1046/j.1365-2842.2003.01143.x. [DOI] [PubMed] [Google Scholar]
- 16.Otuyemi OD, Owotade FJ, Ugboko VI, Ndukwe KC, Olusile OA. Prevalence of signs and symptoms of temporomandibular disorders in young Nigerian adults. J Orthod. 2000;27:61–5. doi: 10.1093/ortho/27.1.61. [DOI] [PubMed] [Google Scholar]
- 17.Pedroni CR, De Oliveira AS, Guaratini MI. Prevalence study of signs and symptoms of temporomandibular disorders in university students. J Oral Rehabil. 2003;30:283–9. doi: 10.1046/j.1365-2842.2003.01010.x. [DOI] [PubMed] [Google Scholar]
- 18.Nomura K, Vitti M, Oliveira AS, Chaves TC, Semprini M, Siéssere S, et al. Use of the Fonseca's questionnaire to assess the prevalence and severity of temporomandibular disorders in Brazilian dental undergraduates. Braz Dent J. 2007;18:163–7. doi: 10.1590/s0103-64402007000200015. [DOI] [PubMed] [Google Scholar]