

Abstract
Background:
The students’ vulnerability to different problems can have an impact on their mental health. Regarding the lack of evidence on the effectiveness of interventional programs based on health education planning models in this area in developing countries, an educational-participatory program based on the PRECEDE model was used, to promote the medical science students’ self-esteem and mental health status, in Iran.
Methods:
In this experimental study, 154 students from the universities of medical sciences in the north east of Iran were selected by stratified random sampling method. Then, they were randomly assigned to two groups of case and control. The questionnaires, including the enabling, reinforcing, and predisposing factors, the Rosenberg self-esteem scale, and the GHQ-28 were used for data collection. Then, an intervention plan, including focus group discussions and training of selected life skills, based on the PRECEDE model, was conducted for the case group.
Results:
The predisposing, reinforcing, and enabling factors, and the self-esteem and mental health of the students showed a significant difference between the case and control groups. The Pearson correlation coefficient showed that there was a correlation between mental health and knowledge (P =0.008), between self-esteem and knowledge (P =0.02), self-esteem and attitude (P =0.01), and mental health and attitude (P = 0.03).
Conclusion:
Health promotion planning by using life skills training based on the PRECEDE model can result in participation and empowerment, in order to promote the self-esteem and mental health of the students.
Keywords: Mental health, PRECEDE model, self-esteem, students
INTRODUCTION
The concept of mental health is a state of health in which a person knows his abilities, can deal with normal life pressures, can be fruitful to the community, and can also have the power of decision-making and participation.[1] Self-esteem means the acceptance and a value that a person feels in him. Psychologists also believe that self-esteem is a portion of mental health, and they consider the enjoyment of self-esteem as a basic and central cause of the social–emotional adjustment of the people.[2]
Self-esteem involves all the daily activities of humans, so it is one of the most important aspects of one's personality and a determinant of the actualization and behavioral characteristics of human beings, and most of the experts know it as an important and fundamental factor in social and emotional adjustment.[3] This characteristic is a general feature in all human beings and is not limited or transient, but is fixed and permanent.[4] People with a low level of self-esteem should be diagnosed, to improve their self-esteem, with appropriate educational programs.[5]
Students are constantly exposed to stressors and experience numerous problem due to the nature of their life during immigration to other places far from home.[6] The studies indicate that students are affected by various psychiatric disorders.[7]
The PRECEDE model is a model for health education and promotion planning, which is used for changing behavior. Its focus is on behavior change at individual or group levels. Green and Kreuter believe that the PRECEDE model has been considered successful in the application of clinical and field trials. This model provides a framework in which the factors affecting behavior, such as: The predisposing, enabling, and reinforcing factors in the educational and assessment phases are determined. The PRECEDE model can be used as a guideline to analyze health problems or health behaviors, and also to determine knowledge, attitudes, and those beliefs that are effective in changes.[8,9]
Several studies, particularly in the last 15 years, suggest that self-esteem is considered as a major psychological factor influencing health and quality of life. It has also been determined that a sense of empowerment and value trace is created for every person with increasing his / her self-esteem, and positive changes flourish in them to gain success, such as: academic achievement, more efforts for success, having a high self-esteem, and a great desire to preserve and promote health.[10] A research on self-esteem and mental health in Canada showed that the most important mental need in 87.4% of the adolescents was self-esteem. A significant relationship was found between low self-esteem and behavioral problems, such as, lack of confidence in relation to others, loss of social relations, and anxiety and depression.[11] Wright, et al. in a large interventional study, in Australia, tried to improve and evaluate community awareness and participation in mental health and mental disorders of individuals, 12 to 18 years of age, using the PRECEDE model,[12] while the researchers’ survey and effort did not show any study based on the PRECEDE model for promoting both self-esteem and mental health among students in Iran. Subsequently, this study was performed to evaluate the effect of an educational-participatory program, based on the PRECEDE model, for promoting the self-esteem and mental health of students in Iran.
METHODS
This is a pre-post experimental study with the control group, conducted during 2006 – 2007. The studied population was the first year students (the freshman students) of medical sciences from two universities in the north east of Iran.
Sampling was done initially, based on a pilot study, among universities of medical sciences in the north east of Iran. Two universities were selected that showed a high prevalence of psychological problems among their students and they also had similar academic conditions and situations. Next, one of the two universities was randomly assigned as the case group and the other was identified as the control group. Considering P1 = 0.27, P2 = 0.05, Zα = 1.96, Zβ = 1.64, and with confidence interval values of 95%, the sample size was determined to be more than 134 students. The students were randomly selected based on a stratified random sampling method. Following this, they were randomly assigned to two groups of case and control. So, the intervention effect was free from any relationship effects between the groups. Both the groups were matched for age, sex, discipline, and educational degree. The inclusion criteria were, studying in medical science subjects, passing at least one university educational term, and voluntary participation in the study. Exclusion criteria were, having a psychiatric disorder and not volunteering for participation in the study. The following tools were used for data collection.
Predisposing, enabling, and reinforcing factors questionnaire (PRECEDE model constructs)
In order to prepare this section of instruments, after a literature review on information resources, a questionnaire was designed. For assessing the predisposing factors, the questions were designed in three parts: (a) Demographic data; (b) Knowledge including a 10-item, three-choice option questions with ‘Yes’, ‘No’, and ‘somewhat’ answers, with a possible range score from 0 to 20 (Example: Do you know the conflicts of the situations you encounter?); and (c) Attitude including an 18-item scale (six points that included, ‘Disagree a little’, ‘Disagree’, ‘completely disagree’, ‘agree a little’, ‘agree’, ‘completely agree’) with a possible range score of 6 to 36. (Example: The best way to prevent getting sick, I see the physician regularly).
For assessing the enabling factors a 10-item, three-choice option questions with ‘Yes’, ‘No’, and ‘somewhat’ answers were designed, related to economic, religious, and environmental factors, with a possible range of score from 0 to 20 (Example: Do you think economic conditions are involved in predicting health behaviors, particularly in your mental health?).
For assessing the reinforcing factors two questions were designed in a three-choice option question with ‘Yes’, ‘No’, and ‘somewhat’ as answers (Example: Have you been encouraged by others such as family, teachers, classmates, friends, etc?)
For determining the content validity of the tools, the questionnaires were given to seven faculty members in the related subjects. After the announcement of their viewpoints and after resolving the problems and reforming the faults, they were submitted to 50 medical students, for reviewing and verifying from the sentences, matching points of view, with implementation, purposes, and aims of the scale producer, and resolving any objection or challenge regarding the understanding of the same concept from each question, by the students. After reviewing and correction of the cases, the reliability of the questionnaire was estimated for 188 students, using the internal consistency and test – retest. The Cronbach's alpha coefficients for internal consistency of the scales were 0.74, 0.78, and 0.78, respectively, and after three weeks of test–retest, the reliability coefficients were 0.80, 0.77, and 0.77, respectively.
Rosenberg self-esteem scale
This known and standard tool, which was developed by Rosenberg (1989), includes 10 questions, and each question is scored based on a four-choice options scale, from ‘quite agree’ to ‘disagree’, with divers scoring for question numbers 9, 6, 5, and 2. The possible range of scores for this scale are from 10 to 40. Hemmati[13] has reported a Cronbach's alpha coefficient of 0.78 for the Farsi translation of this questionnaire.
General Health Questionnaire (GHQ-28)
The General Health Questionnaire-28 is the most recognized screening tool in psychiatry and mental health status, and has had dramatic effects on the development of researches. The 28-item questionnaire was made in order to increase the variance rate, and was based on factor analysis, copied from the main form. It has four scales, with seven questions in each scale, including physical symptoms, anxiety, depression, and disorder in social function. The GHQ's non-traditional method of scoring is the same as the Likert method in which scoring of each test is with four degrees, ‘0, 1, 2, and 3,’ and thus the total score of each individual varies from 0 to 84. In this study the cut off point was considered to be 22 for the student population and for both sexes, so, persons with scores less than 22 were considered to have optimal mental health. Several studies conducted on this questionnaire indicated and showed the high validity and reliability of the questionnaires.[14,15]
For conducting the educational-participatory program based on the PRECEDE model, Focus Group Discussion (FGD) intervention was designed and performed on 12-person subgroups during 12 thirty-to-forty minute sessions for each one, by using life skills training separately, such as, problem-solving, confidence, decision-making, and critical thinking, by one of the researchers. After three months from the pre-test, the questionnaires were completed by the case and control groups. The data were analyzed separately by the SPSS-11.5 software and ANOVA, regression, Pearson correlation coefficient, paired-t, and independent-t-test.
RESULTS
In this study, in both groups, 69.8% were girls and 30.2% were boys, with a mean age of 20.6 ± 1.95 years.
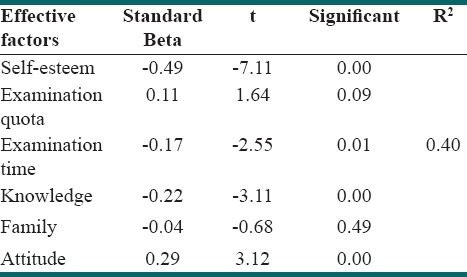
Before performing the program on the case group, the variables affecting the mental health of the students, including the predisposing, enabling, and reinforcing factors, and particularly self-esteem were analyzed by the linear regression test, with controlling of the confounding factors in which self-esteem, examination times, and knowledge and attitude of significant variables were introduced [Table 1]. The statistical test showed predictors, or on the other hand, variables affecting the mental health of the students, to fully explain the process and for effective intervention in accordance with the educational-ecological models’ level, for the researchers.
Table 1.
Multiple regression of self-esteem, knowledge, attitude, examination, and family on the mental health
One-way ANOVA analysis showed no significant relationship between the demographic characteristics, including marital or single status of the top students, or even sex with self-esteem and / or mental health, before their performances.
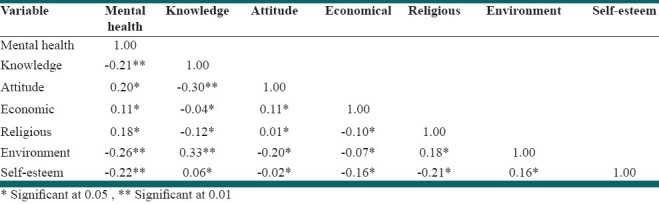
Also, according to Table 2, a significant correlation was obtained based on the polychoric correlation coefficient before intervention in the experimental (case) group, between the predisposing and enabling factors and self-esteem and mental health, and it was significant even after intervention, so that the correlation between mental health and self-esteem (P < 0.0001), and mental health and knowledge (P < 0.008) was at a significant level of 0.01, and also between self-esteem and knowledge (P < 0.02), self-esteem and attitude (P < 0.01), and mental health and attitude (P < 0.03) was obtained at a significant level of 0.05, respectively, even when such a status was not observed in the samples of the control group.
Table 2.
Matrix of polychoric correlation coefficient of variables in experimental group before intervention
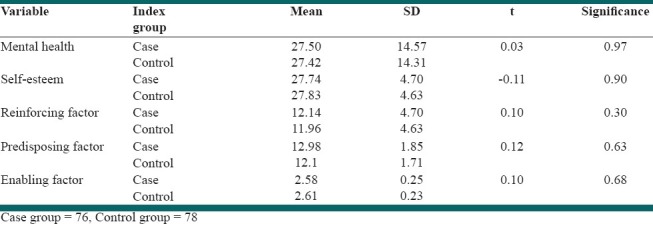
According to Table 3, an independent t-test showed that there were no significant differences between mental health, self-esteem, predisposing, enabling, or reinforcing factors in the case and control groups before the intervention (participatory-educational program based on the PRECEDE model).
Table 3.
Comparison of study variables based on independent t- test before intervention
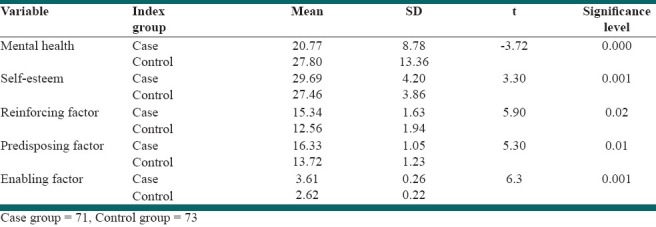
After intervention using an independent t-test, a significant difference had emerged between the mental health, self-esteem, predisposing, enabling, and reinforcing factors in the case and control groups [Table 4]. Comparing Tables 3 and 4, the findings indicated the program efficacy on the students of the experimental group rather than the control group.
Table 4.
Comparison of study variables based on independent t- test after intervention
DISCUSSION
The aim of the research was to determine the effect of a participatory-educational program based on the PRECEDE model to promote the self-esteem and mental health of the students. In short, the research findings introduced self-esteem, examination times, knowledge, and attitude as the significant and affecting variables on the mental health of students.
There was also a significant difference between the predisposing, enabling, and reinforcing factors, self-esteem, and ultimately the students’ mental health, in the case group and the control group, after the intervention. A significant correlation was observed between mental health and self-esteem, mental health and knowledge, self-esteem and knowledge, self-esteem and attitude, and mental health and attitude in the case group after intervention, while such a correlation was not seen in the control group.
In the study, the mental health status showed no significant difference between single and married students, but in Fakhraei's study,[16] the psychological disorder status was reported to be significant in single students. Fakhraei[16], Ziaei and his colleagues[17], and Faraji[18] did not show any relationship between marital states and psychological disorders. Ildarabadi, et al.[19] reported that the depression in married students was higher than in single students. It is also important to note that the length of the education period in the university, especially in medical sciences, varies in different subjects and this can cause variations in the prevalence rate of mental disorders in the students of those fields.
The results before intervention indicated the influence and close relationship of knowledge, attitude, and self-esteem with mental health. Meanwhile, the regression analysis test introduced the self-esteem, knowledge, and attitude variables as significant variables affecting the students’ mental health. The results were considered to be the base and foundation of the design and implementation of the intervention programs based on the model, hence, they were highlighted in the focus group discussions (FGD) among students, and its effectiveness was identified in the intervention program process after implementation on the case group, rather than on the control group. It also showed significant differences in the correlation between self-esteem and mental health, correlation of mental health with knowledge and attitude, and correlation of self-esteem with knowledge and attitude; so self-esteem and the mental health status of the samples were better with increase in knowledge and a positive attitude level. The promotion of students’ mental health was observed as their self-esteem increased and that coordinated with the results of this research and many other texts, such as, those by Mann and colleagues,[10] Mohair,[20] and Moshki et al.[21] Particularly, the significance of these factors, after performing the program, indicated a confirmation of compliance with the study findings and reports of Pope,[22] Botvin,[23] and Talebpour, et al.[24] The influence of knowledge and attitude status from the predisposing factors has been emphasized on mental health and self-esteem, and also a significant correlation between the variables of knowledge, attitude, economic, religious, and environmental factors has been confirmed in the related literature, with self-esteem and their mental health.[20] Meanwhile, the role of self-esteem as a variable of an impressive predictor correlated with mental health has been explained in the studies of Mann and his colleagues, quoted by Tudor[10], Furnham and Cheng[25] Zimmermann[26].
Even Krueter and Green have noted and expressed the influencing role of self-esteem based on the model and have mentioned it specifically and implicationally in the training-ecological stage of the model.[10] Its efficacy can show the power of the model, which can facilitate the exact determining of the study aims, through community participation and empowerment. It cannot be achieved, except through the process of community assessment, using evidence based on community-based participatory approaches, capacity building, and correcting the contributing factors during a review, and regular and continuous evaluation in the form of this model.[12] It is possible that the significant increasing factor of self-esteem and especially mental health, is the use of the educational-participatory program based on the PRECEDE model in the case group rather than in the control group. Using this model as a framework of an intervention, to reduce mental health problems, confirms the study findings in relation to the predisposing factors (knowledge and attitudes), enabling factors (educational resources and skills), and reinforcing factors (social support), with the results of other related researches, including the use of the PRECEDE model in anxiety reduction of the Tehran fire fighters,[27] the impact of education on depression in bypass heart surgery patients, and in accordance with the PRECEDE model in Isfahan,[28] the development and evaluation of community mental health with public awareness based on the PRECEDE–PROCEED model in Australia.[12]
Phoenix and Winnie[29] utilized the predisposing, reinforcing, and enabling factors in the educational diagnosis of the PRECEDE model, to examine their effects on the mental well-being and quality of life among adults in Hong Kong. Structural equation modeling showed that the sense of coherence (predisposing factor), social support (reinforcing factor), and daily hassles (enabling factor) were significantly related to mental health promoting behaviors, which were associated with the mental well-being. We also found a significant relationship between mental health and the mentioned factors of the PRECEDE model in this study.
Wright and colleagues[12] showed that mental health campaigns were differently higher in the target region. It meant that the object of the enabling factor which was to make mental health information more available was accessed. The predisposing and reinforcing factors showed a significant change. They also stated that suicide beliefs associated with depression and psychosis increased or stabilized in the target region, while it declined in the comparison region.
Skarsater, et al.[30] indicated that if mental health was well-designed as an intervention it could empower individuals to take responsibility for adopting mental health promoting behaviors. They emphasized on social supports as a factor to promote mental health. They also recommended the PRECEDE model as a useful framework for understanding factors involved with mental health promoting behaviors, among a large number of their samples.
Considering the effect of the predisposing, enabling, and reinforcing factors of the educational–ecological model on self-esteem and the students’ mental health at first glance, and as the ultimate goal, the cumulative effect of related variables with each of the factors, and during implementation of the educational-participatory programs is matched and has conformity with the PRECEDE model. This model provides some steps for policy development, implementation, and evaluation of an educational program process, because a health education program is a process that is presented in regular consecutive stages.[8]
It is clear that the samples of this study cannot be a representative of the country's student population because of the wide extent and the different distribution of cultural, social, and ethnic characteristics. On the other hand the study samples are limited to the study subjects in two universities of medical sciences, and certainly more studies are needed among students in other subjects across the country, Iran, as also in the state universities, non-profit, and even non-governmental universities. However, may different factors such as individual ethnicity, customs and habits of the students that are effective on students’ self-esteem and their mental health and similar researches should be conducted and expanded in different parts of the country to observe how they work and impact.
CONCLUSION
This study is a part of an extensive and innovative project, using internationally recognized standards of a health promotion program model to promote self-esteem and mental health in the Iran students’ community. The study also offers confidence to researchers in this manner to use approved skills and training methods with student empowerment and participation based on the PRECEDE model, which finally leads to health promotion in a part of the community. In fact, this pattern can provide a clear concept of designing an effective program through community awareness about mental health, so that it can have the ability to comply with all areas, problems, and mental disorders.
In the same manner, and with the help of health education, we should step on the path to promote personal and social confidence and empower people to participate in health promotion. To promote mental health, health education approaches should be strengthened based on this study context and methods. In fact, this strategy shows that even educated people of the society should strive to rely on their own resources. To achieve such self-confidence, people should be informed adequately about having the accurate attitude and sufficient skill to participate in the planning, implementation, and evaluation of health interventions. The goal will be effectively achieved only through appropriate educational activities intending to empower people to protect their health, family, and community in which they live.
ACKNOWLEDGMENTS
We thank all those who assisted us in the implementation of the research, and those who cooperated in performing the task are also appreciated.
Footnotes
Source of Support: Gonabad University of Medical Sciences
Conflict of Interest: None declared.
REFERENCES
- 1.Department of mental health. Australia: University of Melbourne; 2004. WHO. Promoting mental health: a report of the world health organization. [Google Scholar]
- 2.Ansari JA, Ravari A, Kazemi M. The effect of Ramadan on the self-esteem of nursing and midwifery students in Rafsanjan medical university. And isheh Raftar. 2001;7:63–7. [Google Scholar]
- 3.Monk EM. Student mental health: The case studies. Coun Psychol Q. 2004;17:395–412. [Google Scholar]
- 4.Harter S. A model of effects of Perceived Parent Peer support on adolescent false self behavior. Child Dev. 1996;6:360–74. [PubMed] [Google Scholar]
- 5.Bee HL. The Developing Child. 9th ed. Boston, MA: Allyn and Bacon; 2000. [Google Scholar]
- 6.Ross SE. Sources of stress among college student. Coll Stud J. 1999;18:205–14. [Google Scholar]
- 7.Misra R. Academic stress of college students: Comparison of student and faculty perceptions. Coll Stud J. 2000;19:64–72. [Google Scholar]
- 8.Butler Th. Principle of health education and health promotion. United States: Wads Words Co; 2000. pp. 269–74. [Google Scholar]
- 9.Naidoo J, Wills J. Health promotion (foundation for practice) Vol. 6. UK: Bailiere Lindal Co; 2000. pp. 361–3. [Google Scholar]
- 10.Mann M, Hosman CM, Schaalma HP, de Vries NK. Self-esteem in a broad-spectrum approach for mental health promotion. Health Educ Res. 2004;19:357–72. doi: 10.1093/her/cyg041. [DOI] [PubMed] [Google Scholar]
- 11.Plancherel B, Bolognini M. Self esteem and mental heath in early adolescence. J Adolesc. 1995;18:450–74. doi: 10.1006/jado.1996.0022. [DOI] [PubMed] [Google Scholar]
- 12.Wright A, McGorry DP, Harris MG, Jorm AF, Pennell K. Development and evaluation of a youth mental health community awareness campaign – The Compass Strategy. BMC Public Health. 2006;6:215. doi: 10.1186/1471-2458-6-215. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Hemmati R. Factors influencing women harassment: the case study of Tehran family [monograph on the Internet] 2004. [Last cited on 2005 June 28]. Available from: http://www.uswr.ac.ir/S/WQ/refah12/so3.htm .
- 14.Noorbala A, Mohammad K, Yazdi AB, Yasami MT. Mental health survey of the adult population in Iran. Br J Psychiatry. 2004;184:70–3. doi: 10.1192/bjp.184.1.70. [DOI] [PubMed] [Google Scholar]
- 15.Taghavi MR. Validity and reliability of the general health questionnaire (GHQ) J Psychol. 2002;5:381–97. [Google Scholar]
- 16.Fakhraei SA. Dissertation of psychiatric. Tehran: Tehran medical university; 1999. The mental health survey of students in Tehran medical university (IRAN) p. 88. [Google Scholar]
- 17.Ziaei V, Moinolghorabaei M, Jamali M, Faghih A, Malekinejad MH, Naziri Gh. The mental health survey of students in Tehran medical university at the first based on SCL90-R and the result comparison with interview. Teb va Tazkieh. 2001;43:25–33. [Google Scholar]
- 18.Faraji A. MD's thesis. Tehran: Tehran medical university; 2000. The mental health survey of medicine students of Tehran medical university (1994) at the end of internship and the result comparison with their entrance and the effective factors; pp. 91–2. [Google Scholar]
- 19.Ildarabadi A, Firoozkouhi MR, Mazloum SR, Navidian A. The prevalence of student depression of Zabol medical college (IRAN) Sci J Sharekord Med Univ. 2004;6:15–21. [Google Scholar]
- 20.Mohr WK. Johnson's psychiatric-mental health nursing. 5th Ed. USA: Lippincott; 2003. [Google Scholar]
- 21.Moshki M, Ghofranipour F, Allahyari AA. The effectiveness of group discussion on adolescent boys in Gonabad high schools. J Qazvin Med Univ. 2001;19:16–22. [Google Scholar]
- 22.Pope AW, McHale SM, Craighed EW. Translation in Persian by Parisa Tajalli. Tehran: Roshd populations; 1996. Self – esteem enhancement with children and adolescents. [Google Scholar]
- 23.Botvin G J, Griffin K W, Paul E, Macaulay A P. Preventing tobacco and alcohol use among elementary school students through Life Skills Training. J Child Adolesc Subst Abuse. 2003;12:1–18. [Google Scholar]
- 24.Talebpour A, Noori A, Molavi H. The effect of cognitive training on locus of control, development motivation and literacy development of Shahed students. J Psychol. 2002;6:18–29. [Google Scholar]
- 25.Furnham J, Cheng H. Lay theories of happiness. J Happiness Stud. 2000;1:227–46. [Google Scholar]
- 26.Zimmerman SL. States’ spending for public welfare and their suicide rates, 1960 to 1995: what is the problem? J Nerv Ment Dis. 2002;190:349–60. doi: 10.1097/00005053-200206000-00001. [DOI] [PubMed] [Google Scholar]
- 27.Lessan Sh, Ghofranipour F, Birashk B, Faghihzadeh S. Using the PRECEDE model on the anxiety reduction among fire fighters of Tehran city. J Andisheh va Raftar. 2003;9:77–84. [Google Scholar]
- 28.Hazavehei SM, Sabzmakan L, Hassanzadeh A, Rabiei K. The effect of PRECEDE Model-based educational program on depression level in patients with coronary artery bypass grafting. J Qazvin Med Univ. 2008;12:32–40. [Google Scholar]
- 29.Phoenix KH Mo, Winnie WS M. Application of the PRECEDE Model to Understanding Mental Health Promoting Behaviors in Hong Kong. Health Educ Behav. 2008;35:574–87. doi: 10.1177/1090198108317409. [DOI] [PubMed] [Google Scholar]
- 30.Skarsater I, Langius A, Agren H, Haggstrom L, Dencker K. Sense of coherence and social support in relation to recovery in first-episode patients with major depression: A one-year prospective study. Int J Ment Health Nurs. 2005;14:258–64. doi: 10.1111/j.1440-0979.2005.00390.x. [DOI] [PubMed] [Google Scholar]