

Abstract
Introduction:
An increased notification rate of tuberculosis (TB) in men is seen in the SAARC region. In India, the Revised National Tuberculosis Control Programme (RNTCP) detects nearly three times more male than female TB patients. Gender differences have also been reported in the clinical forms of tuberculous disease and in treatment adherence and cure rates in patients undergoing treatment for tuberculosis. The present study was undertaken to find out the sex differences in the notification rates and treatment outcomes of TB patients registered under the RNTCP in a rural tuberculosis unit (TU) in West Bengal.
Materials and Methods:
A retrospective record-based study was carried out among a total of 3605 cases registered under the RNTCP between January 1999 and June 2005. Notification rates of TB, clinical forms of TB and disease treatment outcomes recorded in the registers were analyzed based on genders. Outcomes were defined in accordance with the standard RNTCP definitions. The Z-test for proportion (for comparing differences in proportions), Student t-test (for comparing mean), and χ2 test (to see association) were performed for statistical analysis.
Results:
Among the total of 3605 patients, 2498 (69.3%) were male and 1107 (30.7%) were female with a male female ratio of 2.25:1. In patients less than 20 years of age, the notification rates among males and females were similar. In the other age groups, males were more likely to be notified compared to females and the difference was statistically significant. While new smear positive and retreatment cases were significantly more than in males, among females, new smear negative and new extrapulmonary cases were significantly higher. Among the new smear positive patients 89.4% of females were cured compared to 85.8% of males which was again significant statistically (Z=1.70, P<0.05). Male patients outnumbered females in all the unfavorable outcomes like death, failure, and default although none of the differences were statistically significant (P>0.05).
Conclusion:
The present study demonstrates a gender difference in the notification rates, clinical presentations and treatment outcomes of patients with tuberculosis. Integrated research is necessary to find the reasons for these differences. Such studies will be helpful in improving the efficacy of the RNTCP.
KEY WORDS: Gender, revised national tuberculosis control programme, tuberculosis, West Bengal
INTRODUCTION
About one third of the current global population is infected with TB. An estimated 1 billion women are infected with TB worldwide.[1] TB kills approximately 1 million women every year and is responsible for more deaths in women in the reproductive age group than all causes of maternal mortality combined.[1,2]
All countries in the world show an increased notification rate of pulmonary TB in men.[3] In India, the Revised National Tuberculosis Programme (RNTCP) detects nearly three times more male than female TB patients.[4] In addition to these differences in the notification rates of TB, clinical; presentations of tuberculosis have also been shown to be different among the sexes. Extrapulmonary disease has been reported more commonly in women with lymph nodes being the predominant site.[1,2] Surprisingly, despite facing more socioeconomic and cultural adversities women are less likely to default from TB treatment.[3] Even after adjusting for confounders the male sex was a strong risk factor of unsuccessful treatment outcome.[4]
An extensive search of literature failed to reveal any research from West Bengal that examined gender-related differences in TB patients notified under the RNTCP. The present study was designed to find out whether gender based differences are present in the notification rates, clinical presentations and treatment outcomes of TB patients registered under the RNTCP in a rural tuberculosis unit (TU) in West Bengal.
MATERIALS AND METHODS
The present study was a retrospective record-based study, carried out at the Bagula tuberculosis unit (TU), Nadia, West Bengal. The TU caters to a population of approximately 0.5 million. The majority of the population belongs to a lower socio-economic status. The Bagula TU has five DMCs (Designated Microscopy Centre) manned by five trained laboratory technicians, supervised by a senior tuberculosis laboratory supervisor (STLS). All these MCs are attached to peripheral health institutions and all health care providers in these institutions have been trained in RNTCP. A total of 3605 cases, registered in the TB register of the TU for treatment between January 1999 and June 2005 were taken for the study. All registered cases were stratified into males and females and the results analyzed. The outcomes cured, treatment completed, failure, died, default, and transferred out were in accordance with the RNTCP definitions.[2] The Z test for proportion (for comapring differences in proportions) and student t-test (for comparing mean) were performed for statistical analysis.
RESULTS
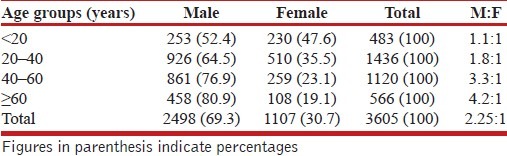
Among the total of 3605 patients, 2498 (69.3%) were male and 1107 (30.7%) were female with an overall male female ratio of 2.25:1. The proportion of male patients notified was significantly higher than females (Z=21.59, P<0.001). The mean ages of males and females were 43.7 ± 17.6 and 36.3 ± 16.9 years respectively with a significant difference (Student t-test=11.79, P<0.001).
In the below 20 years age group, the notification rates in both the sexes were similar. With increasing age the notification rate among males increased with the highest notification rates seen among males in the age group of 60 years and above [Table 1].
Table 1.
Distribution of tuberculosis patients by age and sex group (n=3605)
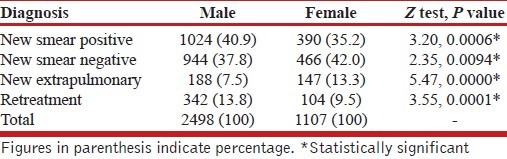
Among the males, the proportion of new smear positive and retreatment cases were significantly higher while among females new smear negative and new extrapulmonary cases were significantly higher [Table 2].
Table 2.
Distribution of case detection by gender (n=3605)
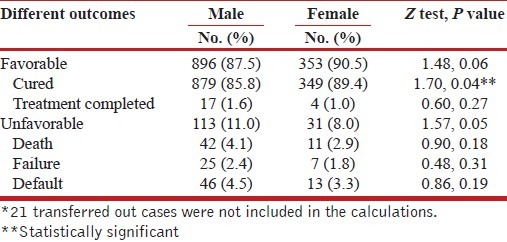
The cure rate in females was 89.4% compared to 85.8% of the males and this difference was statistically significant (Z=1.70, P<0.05). Male patients outnumbered female patients in all the unfavorable outcomes like death, failure, and default although none of the differences were statistically significant (P>0.05) [Table 3].
Table 3.
Different favorable and unfavorable outcomes in new smear-positive cases by gender (n=1393*)
DISCUSSION
TB notification rates have been found to be similar in both sexes till puberty, followed by a continuing widening of the gap between male and female cases. This difference becomes more pronounced after 35–40 year age.[5] The present study reveals that the notification rates of TB before the age of 20 years are similar in both the sexes. With increasing age, the TB notification rates are higher in males. This difference is most marked in the age group beyond 60 years. A similar fourfold increase in the incidence of TB in males aged above 60 years has been seen in other studies.[6]
Differential access to the health care services among females due to socioeconomic and cultural factors, especially in the developing countries has long been considered important reasons for this difference in the TB notification rates. Traditionally, women have poorer access to money, education, information, and health. The decision regarding a woman's treatment is made by the husband or senior members of the family. Women have to depend on the men for their treatment-related expenses and mobility.[7] However, studies from India show that women are more likely than men to access health care services, be notified under DOTS and adhere to treatment in spite of the barriers to the access of the health services.[8]
In a large house to house prevalence survey conducted in Bangladesh difference in the sex ratio (3:1) with an excess of cases in males was noted even after adjusting for confounding factors like income, awareness, and social stigma.[9] A comparison between age- and sex-specific prevalence and notification rates from 29 surveys in 14 countries suggested that the reasons for a low notification rate for TB in females was more due to epidemiological factors than a differential access of the health care.[10] A higher proportion of women had minimal disease compared to men at the time of diagnosis, suggesting an earlier diagnosis among females.[6]
It is evident therefore that biological factors, in addition to the sociocultural factors are to a large extent responsible in the decreased incidence of TB in females, especially in the reproductive age group. Differences in the cellular immunity and antibody response following immunization,[11] increased levels of CD4+ lymphocytes than men,[12] and influence of sex hormones[11] have all been implicated in the decreased incidence of TB in females. However, research in this area is lacking.
Interestingly, although men have higher rates of TB,[13] women have an increased incidence of extrapulmonary TB compared to men.[14,15] The reasons for this increased proportion of extrapulmonary TB in women are not clear but may be due to endocrinal factors.[16]
Paradoxical association of a favourable outcome despite inadequate knowledge about TB among TB patients has been noted in studies from Tanzania.[5] In India, higher success of TB treatment rates in females have been reported.[17] Women are less likely to die, default, or fail on treatment.[18,19] The lack of education and knowledge among females TB patients probably make them more dependent on their directly observed treatment (DOT) providers. These providers, who in most cases are females, tend to interact better with the female patients. In the long run, the trust built up between the patient and her DOT provider ensure better adherence to treatment and hence better treatment outcomes. However, the role of biological factors in causing the differences in treatment outcome among males and females also need to be looked into.
CONCLUSION
Our study demonstrates a sex difference in the notification rate of TB. This difference, traditionally attributed to poor access to health care in females, is at least partially due to biological reasons. Better treatment outcomes in females may reflect biological differences in addition to health system-related factors. Integrated research is necessary to outline the relative roles played by biological factors and gender issues in causing these differences in the notification rates and treatment outcomes of patients under the RNTCP.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Thorson A, Diwan VK. Gender inequalities in tuberculosis: Aspects of infection, notification rates, and compliance. Curr Opin Pulm Med. 2001;7:165–9. doi: 10.1097/00063198-200105000-00009. [DOI] [PubMed] [Google Scholar]
- 2.2005. Directorate General of Health Services. Ministry of Health and family Welfare. New Delhi, India. Revised National Tuberculosis Control Programme. Technical Guidelines for Tuberculosis Control.
- 3.World Health Organization. Gender and tuberculosis control: Towards a strategy for research and action. WHO/CDS/TB/2000.280. [Google Scholar]
- 4.Khatri GR, Frieden TR. The status and prospectus of tuberculosis control in India. Int J Tuberc Lung Dis. 2000;4:193–200. [PubMed] [Google Scholar]
- 5.Chakraborty AK. Epidemiology of tuberculosis: Current status in India. Indian J Med Res. 2004;120:248–76. [PubMed] [Google Scholar]
- 6.Chan-Yeung M, Noertjojo K, Chan SL, Tam CM. Sex differences in tuberculosis in Hong Kong. Int J Tuberc Lung Dis. 2002;6:11–8. [PubMed] [Google Scholar]
- 7.Karim F, Islam MA, Chowdhury AM, Johansson E, Diwan VK. Gender differences in delays in diagnosis and treatment of tuberculosis. Health Policy Plan. 2007;22:329–33. doi: 10.1093/heapol/czm026. [DOI] [PubMed] [Google Scholar]
- 8.Balasubramanian R, Garg R, Santha T, Gopi PG, Subramani R, Chandrasekaran V, et al. Gender disparities in tuberculosis: Report from a rural DOTS programme in south India. Int J Tuberc Lung Dis. 2004;8:323–32. [PubMed] [Google Scholar]
- 9.Salim HM, Declercq E, Van Deun A, Saki KA. Gender differences in tuberculosis: A prevalence survey done in Bangladesh. Int J Tuberc Lung Dis. 2004;8:952–7. [PubMed] [Google Scholar]
- 10.Borgdorff MW, Nagelkerke NJ, Dye C, Nunn P. Gender and tuberculosis: A comparison of prevalence surveys with notification data to explore sex differences in case detection. Int J Tuberc Lung Dis. 2000;4:123–32. [PubMed] [Google Scholar]
- 11.Whitacre CC, Reingold SC, O’Looney PA. A gender gap in autoimmunity. Science. 1999;283:1277–8. doi: 10.1126/science.283.5406.1277. [DOI] [PubMed] [Google Scholar]
- 12.Mair C, Hawes SE, Agne HD, Sow PS, N’doye I, Manhart LE, et al. Factors associated with CD4 lymphocyte counts in HIV-negative Senegalese individuals. Clin Exp Immunol. 2008;151:432–40. doi: 10.1111/j.1365-2249.2007.03573.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Martinez AN, Rhee JT, Small PM, Behr MA. Sex differences in the epidemiology of tuberculosis in San Francisco. Int J Tuberc Lung Dis. 2000;4:26–31. [PubMed] [Google Scholar]
- 14.Yang ZH, Kong Y, Wilson F, Foxman B, Fowler AH, Marrs CF, et al. Identification of risk factors for extrapulmonary tuberculosis. Clin Infect Dis. 2004;38:199–205. doi: 10.1086/380644. [DOI] [PubMed] [Google Scholar]
- 15.Sreeramareddy CT, Panduru KV, Verma SC, Joshi HS, Bates MN. Comparison of pulmonary and extrapulmonary tuberculosis in Nepal - a hospital- based retrospective study. BMC Infect Dis. 2008;8:8. doi: 10.1186/1471-2334-8-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Forssbohm M, Zwahlen M, Loddenkempe R, Rieder HL. Demographic characteristics of patients with extrapulmonary tuberculosis in Germany. Eur Respir J. 2008;31:99–105. doi: 10.1183/09031936.00020607. [DOI] [PubMed] [Google Scholar]
- 17.Ahmed J, Chadha VK, Singh S, Venkatachalappa B, Kumar P. Utilization of RNTCP services in rural areas of Bellary District, Karnataka, by gender, age and distance from health centre. Indian J Tuberc. 2009;56:62–8. [PubMed] [Google Scholar]
- 18.Jimenez-Corona ME, Garcıa-Garcıa L, DeRiemer K, Ferreyra-Reyes L, Bobadilla-del-Valle M, Cano-Arellano B, et al. Gender differentials of pulmonary tuberculosis transmission and reactivation in an endemic area. Thorax. 2006;61:348–53. doi: 10.1136/thx.2005.049452. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.2004. Centre for Public Health Research Administrative Staff College of India. Hyderabad, India. Gender Differentials in the Revised National Tuberculosis Control Programme: Report.