

Abstract
The endodontic treatment of a mandibular molar with aberrant canal configuration can be diagnostically and clinically challenging. This case report presents the treatment of a mandibular first molar with six root canals, of which three canals were located in the mesial root and three in distal root. Third canals were found between the two main root canals. This case presents a rare anatomic configuration and points to the importance of expecting and searching for additional canals.
Keywords: Cone beam computed tomography, mandibular first molar, middle distal canal, middle mesial canal
Introduction
Knowledge of internal dental morphology is an extremely important step in planning and administering endodontic therapy.[1] The numerous anatomical variations existing in the root canal system may contribute to the failure of root canal therapy. Failure to explore and instrument even one of the canals results in improper cleaning of root canal system and can lead to endodontic treatment failure.[2] The mandibular first molar, the earliest permanent posterior tooth to erupt, seems to be the tooth that most often requires root canal treatment. The usual canal distribution is two canals in the mesial root and one or two canals in the distal root. Baugh D and Wallace J. also described the presence of a middle mesial canal.[3] Additionally, Stoner et al. and Beatty and Iterian[4,5] have reported on more obscure cases in which a third canal was located in the distal root. Martinez and Bandaneli[6] showed two cases with six canals. Astonishingly, Reeh[7] has even reported a case with seven canals, consisting of four canals in the mesial root and three in the distal root. The role of advanced diagnostic tools cannot be overlooked in the diagnosis and management of such a complex canal system.
It has been postulated that secondary dentin apposition during tooth maturation would form dentinal vertical partitions inside the root canal cavity, thus creating root canals. A third root canal may also be created inside the root canal cavity of mandibular molars by this process. Such third canals are usually situated centrally between the two main root canals, the buccal and lingual of the mesial and distal roots. The diameter of these third middle canals is usually smaller than that of the other two.[6] This case report presents the management of a mandibular first molar with six root canals, three in mesial and three in distal root. Additionally, this case report highlights the use of Cone Beam Computed Tomography (CBCT) as a diagnostic tool in Endodontics.
Case Report
A 38 year-old female patient presented with a chief complaint of pain in the mandibular right posterior region for the past two weeks. Clinical examination revealed a carious left mandibular first molar (36). The clinical and radiographic findings led to a diagnosis of chronic irreversible pulpitis, necessitating endodontic therapy. Preoperative radiographic evaluation of the involved tooth pointed towards the presence of more than one canals in the distal root [Figure 1]. Anaesthesia of mandibular left first molar was achieved with inferior alveolar nerve block using 2% Lignocaine. The tooth was isolated using a rubber dam and an endodontic access cavity preparation was done. Clinical examination revealed four distinct orifices, two located mesially (mesiobuccal, and mesiolingual) and two distally (distobuccal and distolingual). However, on careful examination of the access cavity with endo-explorer, an additional orifice was detected between the two main canals, both mesially and distally. [Figures 2a and b]
Figure 1.
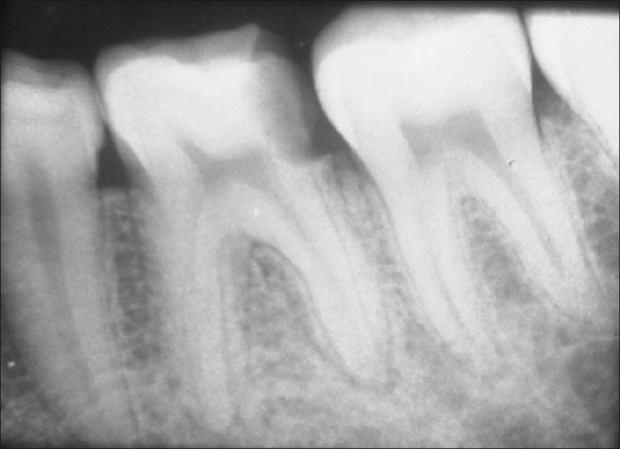
Pre operative radiograph of the mandibular left first molar tooth showing the presence of more than one canals in the distal root, in the patient in the case report
Figure 2a.

Mesial Orifices showing an an additional orifice between the two main buccal and lingual canals in the mandibular left first molar tooth in the patient in the case report
Figure 2b.
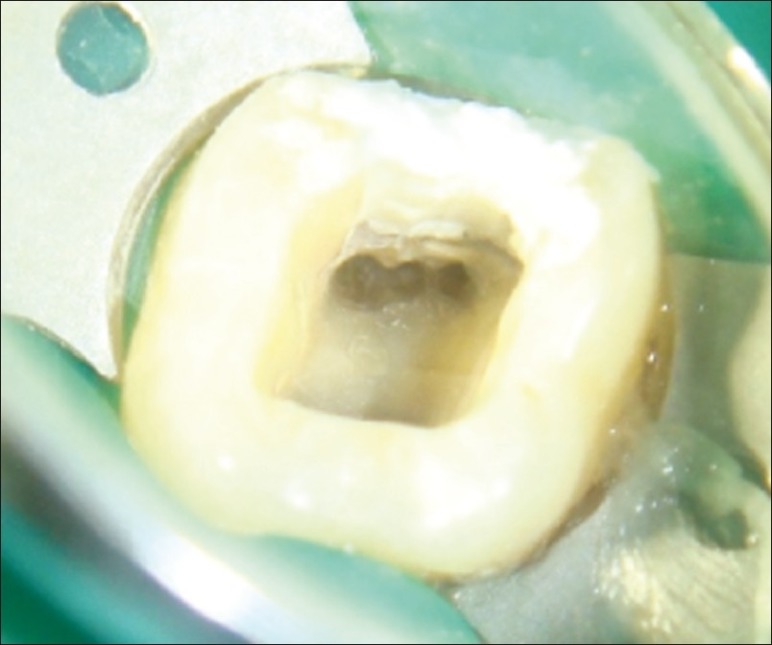
Distal Orifices showing an an additional orifice between the two main buccal and lingual canals in the mandibular left first molar tooth in the patient in the case report
Glide path and patency was achieved using no. 6, 8, and 10 k- files. Working-length radiographs were taken at different angulations with a file placed in each of the three mesial and three distal orifices [Figure 3], and confirmed with electronic apex locator (Raypex 5). Cleaning and shaping was performed using a crown down preparation with rotary Protaper instruments (Maillefer, Dentsply, Ballaigues, Switzerland) under profuse irrigation with 3% sodium hypochlorite solution. After drying the root canals with sterile paper points, obturation was carried out with Protaper gutta percha cones (Maillefer, Dentsply, Ballaigues, Switzerland) using zinc oxide eugenol sealer. The access cavity was temporarily restored with Cavit [Figure 4a and b].
Figure 3.
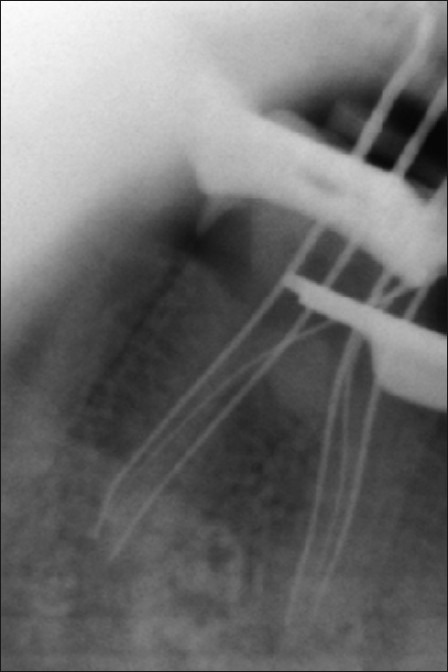
Working Length determination with a file placed in each of the three mesial and three distal orifices
Figure 4a.
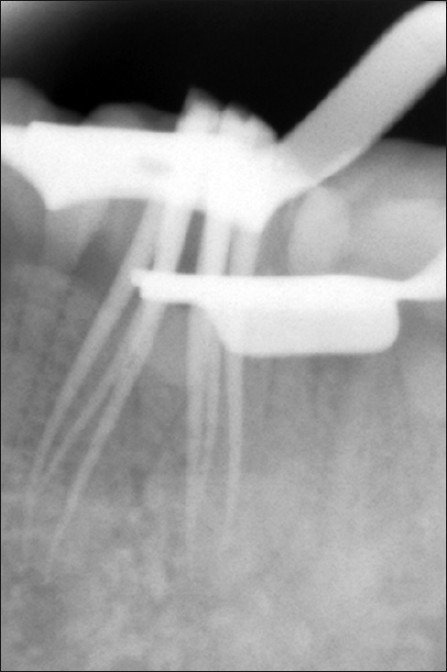
Cones Placed In each of the six root canals of the mandibular left first molar tooth in the patient in the case report
Figure 4b.

Final Obturation of the mandibular left first molar tooth in the patient in the case report
CBCT imaging confirmed the presence of six canals in the concerned tooth. However, the middle mesial and middle distal canals were found confluent with their respective mesial/distal buccal canals at the junction of middle and apical one third, indicating towards the presence of three orifice and two apical foramina in each root [Figure 5a and b].
Figure 5a and b.
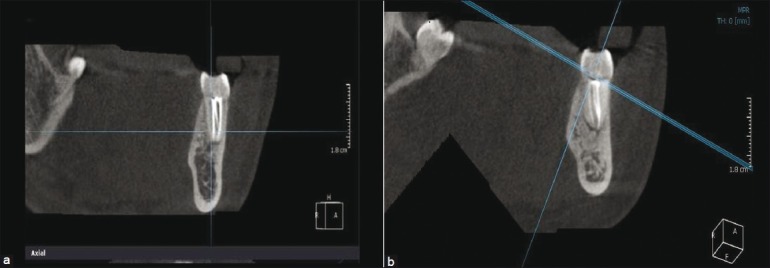
(a) CBCT Image of mesial root confirming the presence of three canals (b) CBCT Image of distal root confirming the presence of three canals
Discussion
A thorough knowledge of root canal morphology and canal configuration of the teeth plays an important role in the success of endodontic therapy.[8] Studies have described the presence of aberrant canals in the mandibular first molar with three canals in the mesial as well as distal roots.[3,9,10,11] The third mesial and distal canal is defined as being independent when a distinct coronal orifice and apical foramen are observed, or confluent when converging into one of the other two main canals and terminating at a common apical foramen.[7] Many authors have agreed on the presence of three foramina in the mesial root; however, only a few reported the presence of three independent canals, which presents itself as a rare anatomical variant. In a study of 760 mandibular molars, Fabra et al.[12] found that 20 molars (2.6%) had three canals in the mesial root. Endodontic success in teeth with the aforementioned number of canals requires a careful clinical and radiographic inspection. Diagnostic aids such as CBCT, Dentascan, multiple preoperative radiographs, examination of the pulp chamber floor with a sharp explorer, troughing of the grooves with ultrasonic tips, staining the chamber floor with 1% methylene blue dye, performing the sodium hypochlorite “champagne bubble test,” and visualizing canal bleeding points are all important aids in locating the root canal orifices.[13] The search for an extra orifice is also aided by the use of microscopes, magnifying loupes and fiber-optic trans-illumination to locate the developmental line between the mesiobuccal and mesiolingual orifices.[14]
A significant constraint in conventional radiography is that it produces a 2D image of a 3D object, resulting in the superimposition of the overlying structures. Therefore, such radiographs are of limited value in cases with complex root canal anatomy. Interpretation and appraisal based on a 2D radiograph may alert the clinician to the presence of aberrant anatomy; however, may not be able to present the variable and complex morphological structure of the root canals and their interrelations. Hence, CBCT has been specifically designed to produce undistorted three dimensional non invasive information of the root canal anatomy. Gopikrishna et al.[15] used spiral computerized tomography for the confirmatory diagnosis of a morphological aberration in the maxillary first molar. Matherne et al. (2008)[16] conducted an ex vivo investigation to compare a Charge Coupled Device Photostimuable Phosphor Plates (CCDPSP) digital radiography system with CBCT to detect the number of root canals in 72 extracted teeth. They found that with digital radiography, endodontists fail to identify at least one root canal in 40% of teeth.
Treating extra canals may be challenging; however, the inability to find and properly treat the root canals may cause failures. With advance diagnostic aids like CBCT and Dentascan, these challenges can be overcome. Although the incidence of root and canal variations is rare, every effort should be made to find and treat all the root canals for successful clinical results.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
References
- 1.Favieri A, Barros FG, Campos LC. Root canal therapy of a maxillary first molar with five root canals: Case report. Braz Dent J. 2006;17:75–8. doi: 10.1590/s0103-64402006000100017. [DOI] [PubMed] [Google Scholar]
- 2.Barbizam JV, Ribeiro RG, Tanomaru FM. Unusual anatomy of permanent maxillary molars. J Endod. 2004;30:668–71. doi: 10.1097/01.don.0000121618.45515.5a. [DOI] [PubMed] [Google Scholar]
- 3.Baugh D, Wallace J. Middle mesial canal of the mandibular first molar: A case report and literature review. J Endod. 2004;30:185–6. doi: 10.1097/00004770-200403000-00015. [DOI] [PubMed] [Google Scholar]
- 4.Stoner W, Remeikis N, Carr G. Mandibular first molar with three distal canals. Oral surgery. 1984;57:554–7. doi: 10.1016/0030-4220(84)90316-5. [DOI] [PubMed] [Google Scholar]
- 5.Beatty RG, Interian CM. A mandibular first molar with five canals: report of case. J Am Dent Assoc. 1985;111:769–71. doi: 10.14219/jada.archive.1985.0208. [DOI] [PubMed] [Google Scholar]
- 6.Martinez-Berna A, Badanelli P. Mandibular first molar with six root canals. J Endod. 1981;8:348–52. doi: 10.1016/S0099-2399(85)80043-1. [DOI] [PubMed] [Google Scholar]
- 7.Reeh E. Seven canals in a lower first molar. J Endodon. 1985;11:348–52. doi: 10.1016/S0099-2399(98)80055-1. [DOI] [PubMed] [Google Scholar]
- 8.Adanir N. An unusual maxillary first molar with four roots and six canals: A case report. Aust D J. 2007;52:333–5. doi: 10.1111/j.1834-7819.2007.tb00511.x. [DOI] [PubMed] [Google Scholar]
- 9.Holtzmann L. Root canal treatment of a mandibular first molar with three mesial root canals. Int Endod J. 1997;30:422–3. doi: 10.1046/j.1365-2591.1997.00106.x. [DOI] [PubMed] [Google Scholar]
- 10.Navarro LF, Luzi A, Garcia AA, Garcia AH. Third canal in the mesial root of permanent mandibular first molars: Review of literature and presentation of 3 clinical reports and 2 in vitro studies. Med Oral Patol Oral Cir Bucal. 2007;12:605–9. [PubMed] [Google Scholar]
- 11.Weine FS. Three canals in the mesial root of mandibular first molar: Case report. J Endod. 1981;8:517–20. doi: 10.1016/S0099-2399(82)80080-0. [DOI] [PubMed] [Google Scholar]
- 12.Fabra-Campos H. Three canals in the mesial root of mandibular first permanent molars: A clinical study. Int Endod J. 1989;22:39–43. doi: 10.1111/j.1365-2591.1989.tb00503.x. [DOI] [PubMed] [Google Scholar]
- 13.Vertucci FJ. Root canal morphology and its relationship to endodontic procedures. Endod Topics. 2005;10:3–29. [Google Scholar]
- 14.Burns RC, Herbranson EJ. Tooth morphology and access cavity preparation. In: Cohen S, Burns RC, editors. Pathways of the pulp. 8th ed. St.Louis,Missouri: Elsevier,Mosby; 2002. pp. 173–229. [Google Scholar]
- 15.Gopikrishna V, Ruben J, Kandaswamy D. Endodontic management of a maxillary first molar with two palatal roots and a single fused buccal root diagnosed with spiral computerized tomography: A case report. Oral Surg Oral Med Oral pathol Oral Radiol Endod. 2008;105:74–8. doi: 10.1016/j.tripleo.2007.11.022. [DOI] [PubMed] [Google Scholar]
- 16.Matherne RP, Angelopoulos C, Kulild JC, Tira D. Use of cone-beam computed tomography to identify root canal systems in vitro. Journal of Endodontics. 2008;34(1):87–89. doi: 10.1016/j.joen.2007.10.016. [DOI] [PubMed] [Google Scholar]