

Abstract
Odontomas have been extensively reported in the dental literature, and the term refers to tumors of odontogenic origin. Though the exact etiology is still unknown, the postulated causes include: local trauma, infection, inheritance and genetic mutation. The majority of the lesions are asymptomatic; however, may be accompanied with pain and swelling as secondary complaints in some cases. Here, we report a case of a compound odontome in a 14 year old patient.
Keywords: Compound odontoma, hamartoma, odontogenic tumor
Introduction
Odontomas are an abnormal mass of calcified dental tissue, usually representing a developmental abnormality. The term is now used to denote leasions that contain all the dental tissues and includes two types, the complex and the compound odontoma.[1] According to the World Health Organization (WHO), a compound odontome is defined as “A malformation in which all dental tissues are represented in a more orderly pattern than in the complex odontoma, so that the lesion contains many tooth like structures. Most of these structures do not morphologically resemble the teeth in the normal dentition; however, enamel, dentin, cementum and pulp are arranged as in the normal tooth.”[1]
Odontomes are the most frequently occurring odontogenic tumors in the oral cavity, and are considered to be hamartomas rather than true neoplasms.[2] They can be considered as mixed odontogenic tumors, as they are composed of both epithelial and mesenchymal elements. These cells and tissues can appear either normal or be deficit in structure. The level of differentiation may vary, creating various formations of dental tissues (enamel, dentin, cementum and pulp). The tissues may form non-descript masses of dental tissues known as complex odontomas to multiple, well-formed tooth like structures known as compound odontomas.[3] They can be discovered at any age, and in any location of the dental arch. The mean age of detection on an average is 14.8 years, with the prevalent age being the second decade of life. There is a slight predilection for occurrence in males (59%) compared to females (41%). The compound odontome is known to occur more commonly in the maxilla (67%) as compared to the mandible (33%), with a marked predilection for the anterior maxillary region (61%).[3,4,5] Here we present a case of a compound odontome discovered accidentally on an Orthopantomogram (OPG) in a patient who desired orthodontic treatment.
Case Report
A 14 year old male patient reported for orthodontic treatment. Patient had maxillary protrusion and wanted orthodontic treatment for the same. A complete intraoral and extraoral examination was carried out. Further, an OPG was advised. The radiographic picture revealed the presence of multiple radio opaque tooth-like structures between the roots of 13 and 14, surrounded by a narrow radiolucent zone [Figure 1]. Adjacent teeth appeared normal without any displacement or resorption. A provisional diagnosis of compound odontome was made. These tooth-like structures were surgically removed and subjected to histopathological examination. Macroscopically, these hard tissue bits were 3 in number and measured approximately 1 cm each in length [Figure 2]. They appeared yellowish-white in color and were hard in consistency. Specimens were subjected to decalcification using 5% nitric acid, and routine histopathological processing was carried out. A part of the specimen was studied by making a ground section. On microscopic examination of hematoxylin and eosion (H and E stain) section, normal appearing enamel spaces, dentin and pulp tissue were seen, and they were exhibiting a regular relation to one another. Presence of cementum was not evident [Figure 3]. Ground section revealed normal tooth architecture. Dentinal tubules and abundant interglobular dentin was seen. Cementum was sparse and seen in isolated distribution [Figure 4]. A definitive diagnosis of “compound odontome” was then made.
Figure 1.

Orthopantomogram showing multiple radio opaque tooth-like structures present between the roots of 13 and 14, surrounded by a narrow radiolucent zone
Figure 2.

Gross specimen of the surgically removed odontomas showing three tooth-like structures
Figure 3.
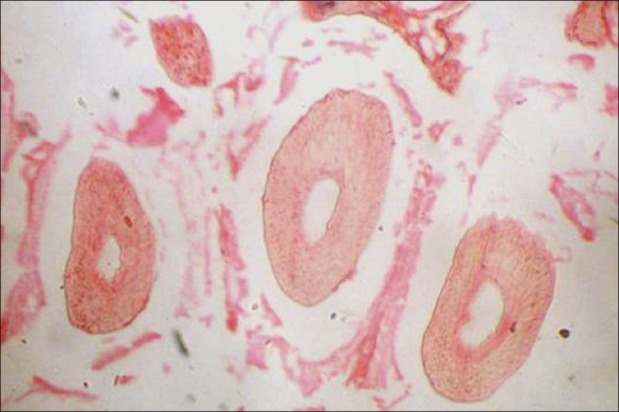
Presence of enamel spaces, dentin and pulp tissue, exhibiting normal relation to one another and thin background stroma, with no evidence of cementum (hematoxylin and eosion stain, ×10)
Figure 4.

Ground section showing normal tooth architecture and arrangement of enamel and dentin, with sparse and isolated cementum (Ground section, ×10)
Discussion
Odontomas are commonly encountered in the first and second decades of life, and are accepted as developmental anomalies (hamartomas) rather than true neoplasms.[6,7,8] The etiology of odontoma remains unknown. Several theories have been proposed, and various causes including trauma, infection, family history and genetic mutation have been postulated. Some investigators have suggested that the ameloblastic fibroma and ameloblastic fibro-odontoma both developmentally and histo-morphologically represent the early stages of formation of odontomes. Most odontomes are asymptomatic, and radiographic findings are by and large diagnostic. Usually, the compound odontoma appears as a collection of tooth-like structures surrounded by a narrow radiolucent zone.[2,9,10] Hence, it can seldom be confused with any other entity such as supernumerary teeth. In our case, the diagnosis was further confirmed with the aid of histopathology. Occasionally, they may become large and produce expansion of bone with consequent facial asymmetry. Odontomes must be surgically removed, in order to prevent cyst formation and possible conversion to odonto-ameloblastoma.[4,5] Ameloblastic odontoma and ameloblastic fibroodontoma bear great resemblance to the common odontoma, particularly on the radiograph, and thus it is suggested that all odontomas should be sent to an oral pathologist for microscopic examination and definitive diagnosis.[4] In most of the odontomas, pathologic alterations are observed in the neighbouring teeth as well such as devitalization, malformation, aplasia, malposition and remaining embedded. Most odontomas are discovered accidently, thus further supporting the use of radiography as an indispensable tool in routine dental clinical examination.
Acknowledgment
I would like to extend my sincere thanks to Dr. Vijay Kabre (Department of Orthodontia) for all his help and guidance.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
References
- 1.Philipsen, Richart PA. Revision of the 1992 edition of the WHO histological typing of odontogenic tumors –A suggestion. J Oral Pathol Med. 2002;31:253–8. doi: 10.1034/j.1600-0714.2002.310501.x. [DOI] [PubMed] [Google Scholar]
- 2.Neville, Damm, Allen, Bouquet . Odontogenic cysts and tumors. 2nd ed. Philadelphia: WB Saunders Company; 2002. Oral and Maxillofacial Pathology; pp. 631–2. [Google Scholar]
- 3.Owens BM, Sachuman NJ, Mineer H, Turner JE, Oliver FM. Dental odontomas: A retrospective study of 104 cases. Clin Pediat Dent. 1997;21:261–4. [PubMed] [Google Scholar]
- 4.Shafer, Hine, Levy . Shafer's Textbook of Oral Pathology. In: Rajendran R, Sivapathasundharam B, editors. Cysts and tumors of odontogenic origin. 5th ed. New Delhi: Elsevier; 2006. pp. 404–7. [Google Scholar]
- 5.Syed MR, Meghana SM, Ahmedmujib BR. Bilateral complex odontomas in mandible. J Oral Maxillofac Pathol. 2006;10:89–91. [Google Scholar]
- 6.To EW. Compound composite odontome associated with impacted canine. Case report. Aust Dent J. 1989;34:414–6. doi: 10.1111/j.1834-7819.1989.tb00698.x. [DOI] [PubMed] [Google Scholar]
- 7.Budnick SD. Compound and complex odontomas. Oral Surg. 1976;42:501–6. doi: 10.1016/0030-4220(76)90297-8. [DOI] [PubMed] [Google Scholar]
- 8.Kamakura S, Matsui K, Katou F, Shirai N, Kochi S, Motegi K. Surgical and orthodontic management of compound odontoma without removal of the impacted permanent tooth. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2002 Nov;94(5):540–2. doi: 10.1067/moe.2002.128096. [DOI] [PubMed] [Google Scholar]
- 9.Cuesta S Amado, Albiol J Gargallo, Aytés L Berini, Escoda C Gay. Review of 61 cases of odontoma. Presentation of an erupted complex odontoma. Med Oral. 2003 Nov-Dec;8(5):366–73. [PubMed] [Google Scholar]
- 10.Yassin OM. Delayed eruption of maxillary primary cuspid associated with compound odontoma. J Clin Pediatr Dent. 1999;23:147–9. [PubMed] [Google Scholar]