

Abstract
The impacted maxillary incisor is detrimental for problems related to esthetics and occlusion in permanent dentition stage. A case with an unerupted maxillary central incisor was diagnosed radiographically with impacted dilacerated maxillary central incisor. The management of the case was carried out surgically and orthodontically. By combining two stages of surgical exposure, orthodontic traction and alignment, the impacted dilacerated incisor was successfully moved into desired position. A two-year follow-up of the stability and periodontal health showed that the tooth placed in the occlusion maintained both esthetics and function.
Keywords: Dilacerated, Impacted, maxillary central incisor, orthodontic correction, surgical exposure
Introduction
The missing maxillary central incisor is an important esthetic and functional concern for the patients. The unerupted tooth may be associated with various factors. Most common factors associated with impacted teeth include supernumerary teeth, odontoma, cysts, crown or root malformation, or ectopic development of tooth germ.[1,2] The frequency of maxillary central incisor impaction has been found in the range of 0.006% to 0.2%.[3]
The dilaceration is characterized by an angulation in the crown and root of the tooth. This is often related to the trauma from the primary central incisors during the early developmental stages of the permanent central incisors.[4] The dilacerated maxillary central incisor poses a clinical dilemma, but can be successfully managed by multidisciplinary surgical and orthodontic treatment modalities to get the best functional and esthetic results. The prognosis of such teeth depends on the ankylosis, external root resorption, and root exposure after traction.[5]
This article presents a case of a 12-year-old female patient with impacted permanent maxillary central incisor, which was diagnosed as dilacerated after the radiographic examination. The case was managed with the multidisciplinary approach surgically and orthodontically.
Case Report
A 12-year-old female patient reported to the Dental Care and Implant Center, Wardha, India, with the complaint of missing maxillary anterior tooth [Figure 1]. The child was physically healthy and had no history of dental and medical trauma. Examination of oral cavity revealed a healthy dental status with permanent dentition. The intraoral radiographs revealed that the permanent central incisor was vertically placed with dilacerated root [Figure 2]. Radiograph showed the presence of sufficient space between maxillary right central incisor and maxillary left lateral incisor.
Figure 1.

Missing permanent maxillary left central incisor
Figure 2.
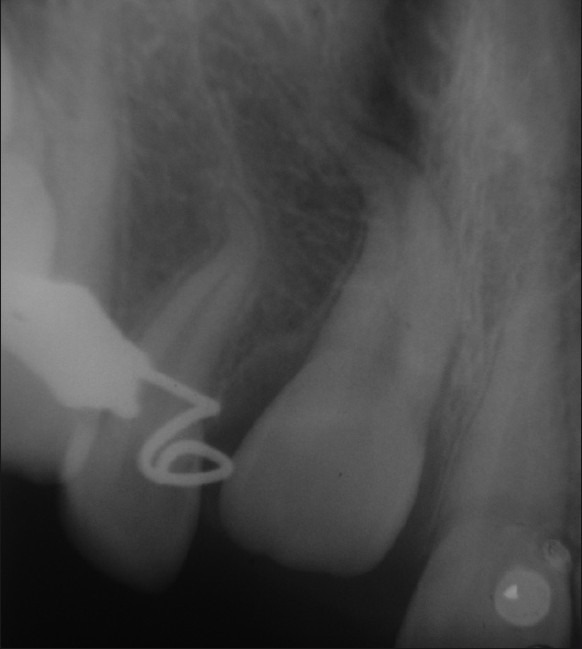
Intraoral periapical radiograph showing dilacerated 21
A combined surgical-orthodontic approach was used to align the dilacerated incisor. Surgical exposure of the crown of the impacted incisor provided access for coronal bracket attachment [Figure 3]. The orthodontic treatment was provided in two phases. The first phase of orthodontic treatment involved an upper removable appliance with elastic traction to the incisor [Figure 4]. Following three months of traction of the tooth, it showed developing cross bite and distal angulation [Figure 5]. This developing malocclusion was corrected by placing inclined plane on the lower incisors. Simultaneously, bracket was placed on maxillary right central incisor along with elastic chain for correction of rotation [Figure 6]. This phase was completed in 10 months.
Figure 3.

Surgical exposure of 21 with bonded bracket on labial aspect
Figure 4.

Removable appliance with elastic traction
Figure 5.

Developing cross-bite of 21
Figure 6.

Bonded bracket on 11 and 21 with elastic chain and cemented inclined plane on 31
The second phase of orthodontic treatment was with an upper fixed appliance to correct the alignment [Figure 7]. There was no complication related to the traction and alignment of the tooth. The treatment in this phase completed in 2 months. The results after completion of the treatment were satisfying, with the tooth in correct esthetic and functional position with normal gingival contour and healthy periodontium [Figure 8].
Figure 7.

Fixed orthodontic correction
Figure 8.

Photograph showing 21 in desired position at the end of the treatment
The patient was recalled for check-up every 6 months and remained symptom-free 2 years after treatment [Figure 9].
Figure 9.

After 2-year follow-up
Discussion
Impacted maxillary permanent central incisor due to dilaceration is rare and has serious impact on esthetics, phonetics, mastication, and psychology in young patients.
The impacted permanent teeth commonly results in migration of adjacent teeth leading to the space loss and hence insufficient space available for the movement of impacted tooth in the desired position.[6] In this case, the clinical as well as radiographic examinations clearly showed that there was enough space available for the traction of the impacted maxillary left central incisor.
Depending on the localization and degree of dilaceration, a number of treatment options have been suggested. Surgical exposure and moving the impacted tooth into normal occlusion with light force orthodontic traction is well accepted and reported as a current treatment modality.[7–11] The present case illustrates the management of impacted dilacerated maxillary central incisor in permanent dentition. The crown of the tooth was palpable in the vestibular sulcus and the covering mucosa was thick and fibrous. A small window was opened surgically to expose the crown and facilitate the placement of the bracket on labial surface. The bracket was cemented and the orthodontic traction was carried out, which resulted in successful positioning of the dilacerated tooth in the arch.
It is suggested that the success rate of dilacerated impacted tooth depends on the degree of dilaceration, position of the tooth, and the amount of root formation.[10] The patient presented here was in permanent dentition with completely formed root with acute dilaceration, which was a challenge for the clinicians.
The slow orthodontic traction resulted in good periodontal and periapical health of the tooth. The present case showed successful results after multidisciplinary approach maintaining the natural tooth in desired position. In comparison with other treatment modalities like extraction and prosthetic appliances including dental implants, the patient's own tooth being the most biocompatible one brings about better functional, esthetical, and emotional results.[10,11]
Conclusion
The coordinated multidisciplinary approach toward the management of impacted maxillary central incisor resulted in favorable esthetic and functional outcome. The creation of surgical window, use of the orthodontic traction, and an availability of sufficient space were the important parameters for the positive outcome. The present case endorses the — surgical-orthodontic treatment approach for sustainable and guaranteeing results.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
References
- 1.Stewart DJ. Dilacerated unerupted maxillary central incisors. Br Dent J. 1978;145:229–33. doi: 10.1038/sj.bdj.4804154. [DOI] [PubMed] [Google Scholar]
- 2.Andreasen JO. The impacted incisor. In: Andreasen JO, Petersen JK, Laskin DM, editors. Textbook and color atlas of tooth impactions. Diagnosis, treatment and prevention. Copenhagen: Munksgaard; 1997. pp. 113–24. [Google Scholar]
- 3.Grover PS, Lorton L. The incidence of unerupted permanent teeth and related clinical cases. Oral Surg Oral Med Oral Pathol. 1985;59:420–5. doi: 10.1016/0030-4220(85)90070-2. [DOI] [PubMed] [Google Scholar]
- 4.Andreasen JO. Injuries to developing teeth. In: Andreasen JO, Andreasen FM, editors. Textbook and color atlas of traumatic injuries to the teeth. Copenhagen: Munksgaard; 1994. pp. 457–94. [Google Scholar]
- 5.Lin YJ. Treatment of an impacted dilacerated maxillary central incisor. Am J Orthod Dentofac Orthop. 1999;115:406–9. doi: 10.1016/s0889-5406(99)70260-x. [DOI] [PubMed] [Google Scholar]
- 6.Duncan WK, Ashrafi MH. Management of the nonerupted maxillary anterior tooth. J Am Dent Assoc. 1983;106:640–4. doi: 10.14219/jada.archive.1983.0144. [DOI] [PubMed] [Google Scholar]
- 7.Tanaka E, Watanabe M, Nagaoka K, Yamaguchi K, Tanne K. Orthodontic traction of an impacted maxillary central incisor. J Clin Orthod. 2001;35:375–8. [PubMed] [Google Scholar]
- 8.Crawford LB. Impacted maxillary central incisor in mixed dentition treatment. Am J Orthod Dentofac Orthop. 1997;112:1–7. doi: 10.1016/s0889-5406(97)70266-x. [DOI] [PubMed] [Google Scholar]
- 9.Macias E, Carlos F, Cobo J. Posttraumatic impaction of both maxillary central incisors. Am J Orthod Dentofac Orthop. 2003;124:331–8. doi: 10.1016/s0889-5406(03)00305-6. [DOI] [PubMed] [Google Scholar]
- 10.Kuvvetli SS, Seymen F, Gencay K. Management of an unerupted dilacerated maxillary central incisor: A case report. Dent Traumatol. 2007;23:257–61. doi: 10.1111/j.1600-9657.2005.00424.x. [DOI] [PubMed] [Google Scholar]
- 11.Giampietro F, Cinzia M, Davide F. Orthodontic movement of a dilacerated maxillary incisor in mixed dentition treatment. Dent Traumatol. 2009;25:451–6. doi: 10.1111/j.1600-9657.2008.00722.x. [DOI] [PubMed] [Google Scholar]