

Abstract
Background:
Some boys with sexual precocity are known to have behavioral problems like increased physical and verbal aggression and school and social maladjustments. It is believed to be due to premature androgen exposure. However, it is not clear why only some develop this problem, difference in etiology could be one explanation.
Aim:
The aim of the study is to assess behavioral aggression in boys with sexual precocity due to different disorders.
Materials and Methods:
Seven children, ages three to seven years, were enrolled for this study. Two were diagnosed to have congenital adrenal hyperplasia (CAH), three had testotoxicosis, while two had central precocious puberty. Parents of children with precocious puberty underwent the (CASP) questionnaire (children's aggression scale-parent version).
Results:
Testosterone levels were high in all patients. Parents denied any history of physical or verbal aggression in the two boys with CAH. Their CASP rating was 0. In contrast, the CASP ratings in the two boys with testotoxicosis and the two with precocious puberty for five domains ranged from 3.1 – 24.2, 2.6 – 8.3,1-5.6,0 – 7.1, and 0 – 1, respectively. In the present study, increased aggression was seen among all the patients with testotoxicosis and both with precocious puberty. In contrast, there were no symptoms of either increased verbal or physical aggression in either of the two patients with CAH.
Conclusions:
The hormonal milieu in the boys with CAH versus those with sexual precocity due to other causes differed in terms of cortisol and androgen precursors. The androgen excess in CAH children was a consequence of cortisol deficiency. It is possible that cortisol sufficiency is required for androgen-mediated behavioral effects.
Keywords: Aggression, cortisol, hormones, precocious puberty, testosterone
INTRODUCTION
The onset of puberty in males is associated with heightened self-esteem, increased aggression, and an increased sense of social dominance.[1–3] Sexual precocity in boys may be due to a premature activation of the hypothalamo-pituitary-gonadal axis (also referred to as true precocious puberty) or peripheral production of androgens from the adrenals or testis (i.e., congenital adrenal hyperplasia and adrenal or testicular tumors) or due to hypersensitivity to gonadotropins (i.e., testotoxicosis). All these conditions are characterized by increased levels of androgens. Precocious androgen exposure (sexual precocity) is associated with behavioral problems in the form of increased physical and verbal aggression, poor school performance, and social maladjustments.[4] Sonis et al., described 33 children with precocious puberty (due to different causes). Twenty-seven percent of these children scored above the ninety-eighth percentile on the aggression scale.[5] Money and Alexander reported temper tantrums and increased energy expenditure in some of the 18 boys with precocious puberty (four idiopathic precocious puberty and 14 CAH).[6] Increased aggression was observed in two of the 24 males with precocious puberty.[4] The aggression in one male was so severe that admission to Psychiatry and later transfer to a mental hospital was required. It is not known why only some children with sexual precocity manifest with aggressive behavior. Differences in the pathogenetic mechanisms for sexual precocity may underlie the differences in the manifestations of behavioral aggression. Duration of androgen exposure, social factors, and levels of other hormones may variably influence behavioral aggression.[7–9] Even as testosterone levels are high in all the conditions leading to sexual precocity, androgen precursors and cortisol levels differ depending on the etiology and age at presentation. Some previous studies have suggested that androgen precursors and cortisol may moderate androgen response to behavioral aggressiveness.[10,11] Sexual precocity provides natural models to study the effects of androgens on aggressive behavior. The aim of the present study was to assess behavioral aggression in boys with sexual precocity due to different conditions.
MATERIALS AND METHODS
Boys with sexual precocity attending this hospital were enrolled for this study. They underwent detailed evaluation, including medical history and a physical examination, including anthropometry, hormonal assessment, and radiological evaluation, to identify the pathological basis for the sexual precocity. Prior to the treatment, the parents of these children were asked to rate their child's behavior using the CASP-questionnaire (children's aggression scale-parent version).[10] This scale had 33 items, each representing the five domains (verbal aggression, aggression against objects and animals, provoked physical aggression, unprovoked physical aggression, and use of weapons). The CAS-P questionnaire gauges the frequency and severity of the aggressive acts within each domain. Differences in frequency are accounted for by assigning each rating on the Likert Scale with a whole number value (i.e., never = 0, once / month or less = 1, once per week or less = 3, and most days = 4), which is multiplied by the weighting value of each item. The validity and reliability of the CAS-P scale and the high internal consistency and correlation with other rating scales has been demonstrated earlier.[10] Parents were also queried with regard to the problems related to aggression faced by the family at home and at school.
Hormonal assays
Samples for Luteinizing hormone (LH), Follicle-stimulating hormone (FSH), Adrenocorticotropic hormone (ACTH), cortisol, dehydroepiandrosterone (DHEAS), and testosterone were measured by electrochemiluminescence (ELECSYS2010, Roche diagnostics). The 17-OH-progesterone (17 OHP) was measured by radio immunoassay (kit supplied by Immunotech, Marcelle, France. Magnetic resonance imaging (MRI) was done for cranial imaging, while computed tomography / ultrasound was used for abdominal imaging. The luteinizing hormone-releasing hormone (LHRH) stimulation test was performed with Triptorelin (LHRH analog) given in the dose of 100 μg, subcutaneously. Samples for LH and FSH were estimated at 0, 2, 4, 8, and 24 hours, respectively.
RESULTS
Seven boys with sexual precocity were enrolled for this study. Investigations revealed that three had testotoxicosis, two had CAH, and two had central precocious puberty (1- pinealoma and 1-Idiopathic Precocious Puberty). The age at presentation and details of hormonal investigations are given in Table 1. The mother of MA commented that her child had age-appropriate genitalia till six months back, which had grown to almost an adult-sized phallus recently. This was in contrast to other children who had gradual enlargement of their genitalia over a period of one to three years. Testosterone levels were high in all the patients. Parents of patients with CAH denied any history of physical or verbal aggression in them. Their CASP rating was 0. In contrast, the CASP rating for all domains of aggression in boys with testotoxicosis and idiopathic precocious puberty were high [Table 2]. The three boys with testotoxicosis scored 3.1, 12.8, and 24.2 on verbal aggression, 2.6, 4.3, and 8.3 on aggression against objects and animals, 1.0, 1.0, and 5.6 on a scale of provoked physical aggression, and 3.1, 3.2, and 7.1 on a scale of unprovoked physical aggression. Among the three boys with testotoxicosis, MA was comparatively less aggressive as compared to the other two. He also had a more rapid progression of symptoms compared to other children. The CASP rating for the boys with precocious puberty for five domains ranged from 0 – 10.1. The parents of all the children felt that their children were intelligent and had good learning abilities. The parents of RG reported that he was experiencing difficulty adjusting at school. He was jeered at by other children for his tall stature and masculine voice. This resulted in frequent fights. He had also used bricks on two occasions to hurt other children. The parents had discussed his illness and these issues with the school authorities, but there was little improvement. RG did not want to go to school. The relatives and elders in the house suggested transfer to another school and a higher class (class 1) for his age. SP, a boy with testotoxicosis, also used to have frequent fights with children at school. MK, one with IPP, was living with his grandparents and mother, as he had lost father at an early age. The grandfather felt his grandson was quite intelligent. He was also facing problems adjusting in school.
Table 1.
Hormonal details for the subjects
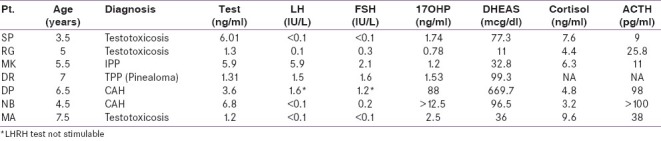
Table 2.
Measures of aggression representing five domains for the subjects

DISCUSSION
Several studies have shown a positive, albeit a low association between aggression and androgen levels in adult males. However, a few studies have reported lack of association between the two parameters.[7,12–14] Lack of uniformity of data has been attributed to a number of factors that include differences in the parameters used to define various aspects of behavioral aggression, social and developmental factors, and the modulating effect of the intelligence on aggressive behavior.[7–9,15] It has also been suggested that hormonal factors, especially some components of the HPA axis (cortisol and androgen precursors), besides testosterone, may affect the expression of behavioral aggression.[10,11] Low cortisol levels and low cortisol variability have been shown to be associated with increased aggression and antisocial behavior.[16–18] In contrast, Scerbo et al., reported no interaction between testosterone and cortisol in relation to aggression.[11] Van Goozen et al., observed a positive relationship between androstenedione (androgen precursor) and aggressive behavior in the conduct disorder of prepubertal boys.[19] Azurmendi et al., also observed a positive association between aggression and androstenedione levels, but no relationship with the DHEA levels in five-year-old boys.[20] In contrast, Susman et al., reported a lack of association between androstenedione or DHEA levels and aggression in male volunteers aged 10 – 14 years.[2] It is difficult to interpret these different studies, as gonadal and adrenal steroids in normal individuals show that wide inter-individual variations fluctuate throughout the day and vary with various extrinsic factors.
The present study included patients with congenital adrenal hyperplasia (CAH), testotoxicosis, and central precocious puberty. All these conditions are rare hormonal disorders, characterized by a precocious androgen excess that provide natural models, to study the role of androgens on behavior during childhood. CAH is an autosomal recessive disorder,[21] caused due to the deficiency of one of the five enzymes involved in adrenal steroidogenesis.[22] Steroid deficiency leads to ACTH excess and adrenal androgen overproduction. Testotoxicosis is another rare autosomal dominant disorder that is characterized by increased androgen production, as a consequence of the autoactivation of the LH receptor.[23,24] The hypothalamo-pituitary-adrenal axis is essentially normal in patients with testotoxicosis. Central precocious puberty is a true puberty, wherein there is a premature activation of the hypothalamo-pituitary-gonadal axis. The various causes for central precocious puberty include hypothalamic and pituitary tumors, infections or radiation. Pineal tumors are extremely rare causes for precocious puberty.
The two males with CAH in the present study had absence of any features of behavioral aggression, as reported by the parents. These results are in agreement with the previous reports. Pasterski et al., reported no increase in aggression or activity in 29 boys with CAH (age 3 – 11 years) in comparison to the normal controls.[25] Lack of behavioral aggression was also reported in some previous studies in young boys with CAH.[26,27] Females with CAH are known to express a tomboyish behavior and have preferences for male play toys during childhood.[28–31] However, studies on other aspects of aggression, dominance or activity have shown mixed results.[26,27,32,33]
The three boys with testotoxicosis in the present study scored high on the CASP scale for aggressive behavior. The two boys with central precocious puberty also scored high on the aggression scale. One patient with testotoxicosis, who had a rapid progression of symptoms, was comparatively less aggressive than the other children, with either precocious puberty or testotoxicosis. It is possible that the degree of behavioral aggressiveness is affected by the duration of androgen exposure. Testotoxicosis being a rare disorder, there are no systematic studies assessing the behavior pattern of these boys. Anecdotal case reports have shown high measures of verbal and physical aggression in them. Laue et al., studied nine boys with familial testotoxicosis. The parents of all the nine boys reported an aggressive behavior that disappeared with the combined spironolactone and testolactone treatment.[34] Leschek et al., described 10 boys with testotoxicosis, four of whom reported aggressive behavior.[35] However, no detailed assessment of measures of aggression was done in this study.
In the present case series, the absence of aggressive behavior in boys with CAH and high measures of aggression in those with testotoxicosis are in agreement with previous reports. These conditions differ in terms of the prevailing cortisol. The basal cortisol levels were in the normal range for subjects with testotoxicosis and idiopathic precocious puberty. In patients with CAH, although basal cortisol was only marginally lower, high ACTH levels and increased androgen precursors in them indicated a state of partially compensated cortisol deficiency. It is possible that for optimal androgen action, a cortisol sufficient state is required. That could explain the absence of aggression seen in the two patients with CAH in the present case series. We had recently reported the fertility outcomes in patients with classical CAH in spite of the absence of steroid initiation till the age of nine years.[36] Even mild androgen excess in cortisol replete states (PCOS and Cushing's) is known to have adverse effects on ovarian functions. CAH females in our study had good fertility outcomes in spite of prolonged androgen exposure. We hypothesized that cortisol deficiency, as a consequence of an untreated CAH state, was responsible for the apparent androgen resistance in these patients, that is, normal cortisol levels are needed for mediating the adverse effects of androgens on the reproductive endocrine axis of CAH patients. It is also possible that cortisol in a similar fashion also moderates the action of androgens on aggressive behavior.
In conclusion, the boys with CAH had differential behavioral aggressive patterns compared to those with testotoxicosis or precocious puberty. Cortisol sufficiency was possibly a prerequisite for optimal androgen action. This being a small study, larger studies involving more number of patients in each group, are required to validate our findings.
ACKNOWLEDGEMENT
We would like to acknowledge the assistance of Dr. Rajesh Khadgawat for providing patients for this study.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Bernstein I, Gordon TP, Rose RM. The interaction of hormones, behavior and social context in non human primates. In: Svare BB, editor. Hormones and Aggressive Behaviour. New York: Plenum; 1983. pp. 535–61. [Google Scholar]
- 2.Susman EJ, Inoff-Germain G, Nottelmann ED, Loriaux DL, Cutler GB, Jr, Chrousos GP. Hormones, emotional dispositions, and aggressive attributes in young adolescents. Child Dev. 1987;58:1114–34. [PubMed] [Google Scholar]
- 3.Olweus D, Mattsson A, Schalling D, Löw H. Testosterone, aggression, physical, and personality dimensions in normal adolescent males. Psychosom Med. 1980;42:253–69. doi: 10.1097/00006842-198003000-00003. [DOI] [PubMed] [Google Scholar]
- 4.Sigurjonsdottir TJ, Hayles AB. Precocious puberty. A report of 96 cases. Am J Dis Child. 1968;115:309–21. doi: 10.1001/archpedi.1968.02100010311003. [DOI] [PubMed] [Google Scholar]
- 5.Sonis WA, Comite F, Pescovitz OH, Hench K, Rahn CW, Cutler GB, Jr, et al. Biobehavioral aspects of precocious puberty. J Am Acad Child Psychiatry. 1986;25:674–9. doi: 10.1016/s0002-7138(09)60293-4. [DOI] [PubMed] [Google Scholar]
- 6.Money J, Alexander D. Psychosexual development and absence of homosexuality in males with precocious puberty.Review of 18 cases. J Nerv Ment Dis. 1969;148:111–23. doi: 10.1097/00005053-196902000-00002. [DOI] [PubMed] [Google Scholar]
- 7.Archer J. The influence of testosterone on human aggression. Br J Psychology. 1991;82:1–28. doi: 10.1111/j.2044-8295.1991.tb02379.x. [DOI] [PubMed] [Google Scholar]
- 8.Booth A, Johnson DR, Granger DA, Crouter AC, McHale S. Testosterone and child and adolescent adjustment: The moderating role of parent-child relationships. Dev Psychol. 2003;39:85–98. doi: 10.1037//0012-1649.39.1.85. [DOI] [PubMed] [Google Scholar]
- 9.Rowe R, Maughan B, Worthman CM, Costello EJ, Angold A. Testosterone, antisocial behavior, and social dominance in boys: Pubertal development and biosocial interaction. Biol Psychiatry. 2004;55:546–52. doi: 10.1016/j.biopsych.2003.10.010. [DOI] [PubMed] [Google Scholar]
- 10.Susman EJ, Granger DA, Murowchick E, Ponirakis A, Worrall BK. Gonadal and adrenal hormones.Developmental transitions and aggressive behavior. Ann N Y Acad Sci. 1996;794:18–30. doi: 10.1111/j.1749-6632.1996.tb32506.x. [DOI] [PubMed] [Google Scholar]
- 11.Scerbo AS, Kolko DJ. Salivary testosterone and cortisol in disruptive children: Relationship to aggressive, hyperactive, and internalizing behaviors. J Am Acad Child Adolesc Psychiatry. 1994;33:1174–84. doi: 10.1097/00004583-199410000-00013. [DOI] [PubMed] [Google Scholar]
- 12.Brain PF, Haug M. Hormonal and neurochemical correlates of various forms of animal “aggression”. Psychoneuroendocrinology. 1992;17:537–51. doi: 10.1016/0306-4530(92)90014-x. [DOI] [PubMed] [Google Scholar]
- 13.Rubinow DR, Schmidt PJ. Androgens, brain, and behavior. Am J Psychiatry. 1996;153:974–84. doi: 10.1176/ajp.153.8.974. [DOI] [PubMed] [Google Scholar]
- 14.Book AS, Starzyk KB, Quinsey VL. The relationship between testosterone and aggression: A meta- analysis. Aggress Voilent Behav. 2001;6:579–99. [Google Scholar]
- 15.Chance SE, Brown RT, Dabbs JM, Casey R. Testosterone, intelligence and behavior disorders in young boys. Pers Individ Differ. 2000;28:437–45. [Google Scholar]
- 16.McBurnett K, Lahey BB, Rathouz PJ, Loeber R. Low salivary cortisol and persistent aggression in boys referred for disruptive behavior. Arch Gen Psychiatry. 2000;57:38–43. doi: 10.1001/archpsyc.57.1.38. [DOI] [PubMed] [Google Scholar]
- 17.Shoal GD, Giancola PR, Kirillova GP. Salivary cortisol, personality, and aggressive behavior in adolescent boys: A 5-year longitudinal study. J Am Acad Child Adolesc Psychiatry. 2003;42:1101–7. doi: 10.1097/01.CHI.0000070246.24125.6D. [DOI] [PubMed] [Google Scholar]
- 18.Popma A, Vermeiren R, Geluk CA, Rinne T, van den Brink W, Knol DL, et al. Cortisol moderates the relationship between testosterone and aggression in delinquent male adolescents. Biol Psychiatry. 2007;61:405–11. doi: 10.1016/j.biopsych.2006.06.006. [DOI] [PubMed] [Google Scholar]
- 19.van Goozen SH, Matthys W, Cohen-Kettenis PT, Thijssen JH, van Engeland H. Adrenal androgens and aggression in conduct disorder prepubertal boys and normal controls. Biol Psychiatry. 1998;43:156–8. doi: 10.1016/S0006-3223(98)00360-6. [DOI] [PubMed] [Google Scholar]
- 20.Azurmendi A, Braza F, Sorozabal A, García A, Braza P, Carreras MR, et al. Cognitive abilities, androgen levels, and body mass index in 5-year-old children. Horm Behav. 2005;48:187–95. doi: 10.1016/j.yhbeh.2005.03.003. [DOI] [PubMed] [Google Scholar]
- 21.Pang S. Congenital adrenal hyperplasia. Endocrinol Metab Clin North Am. 1997;26:853–91. doi: 10.1016/s0889-8529(05)70285-1. [DOI] [PubMed] [Google Scholar]
- 22.White PC, Speiser PW. Congenital adrenal hyperplasia due to 21-hydroxylase deficiency. Endocr Rev. 2000;21:245–91. doi: 10.1210/edrv.21.3.0398. [DOI] [PubMed] [Google Scholar]
- 23.Aziz AA, Jafri SM, Haque NU. Testotoxicosis: Gonadotrophin-independent male sexual precocity. Postgrad Med J. 1992;68:225–8. doi: 10.1136/pgmj.68.797.225. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Reiter EO, Norjavaara E. Testotoxicosis: Current viewpoint. Pediatr Endocrinol Rev. 2005;3:77–86. [PubMed] [Google Scholar]
- 25.Pasterski V, Hindmarsh P, Geffner M, Brook C, Brain C, Hines M. Increased aggression and activity level in 3- to 11-year-old girls with congenital adrenal hyperplasia (CAH) Horm Behav. 2007;52:368–74. doi: 10.1016/j.yhbeh.2007.05.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Ehrhardt AA, Baker SW. Fetal androgens, human central nervous system differentiation, and behaviour sex differences. In: Friedman RC, Richart RM, van de Wiele RL, editors. Sex Differences in Behaviour. New York: Wiley; 1974. pp. 33–52. [Google Scholar]
- 27.Berenbaum SA, Resnick SM. Early androgen effects on aggression in children and adults with congenital adrenal hyperplasia. Psychoneuroendocrinology. 1997;22:505–15. doi: 10.1016/s0306-4530(97)00049-8. [DOI] [PubMed] [Google Scholar]
- 28.Dittmann RW, Kappes MH, Kappes ME, Börger D, Meyer-Bahlburg HF, Stegner H, et al. Congenital adrenal hyperplasia.II: Gender-related behavior and attitudes in female salt-wasting and simple-virilizing patients. Psychoneuroendocrinology. 1990;15:421–34. doi: 10.1016/0306-4530(90)90066-i. [DOI] [PubMed] [Google Scholar]
- 29.Bernbaum SA, Hines M. Early androgens are related to childhood sex –typed toy preferences. Psychol Sci. 1992;3:203–6. [Google Scholar]
- 30.Hines M, Kaufman FR. Androgen and the development of human sex-typical behavior: Rough-and-tumble play and sex of preferred playmates in children with congenital adrenal hyperplasia (CAH) Child Dev. 1994;65:1042–53. [PubMed] [Google Scholar]
- 31.Pasterski VL, Geffner ME, Brain C, Hindmarsh P, Brook C, Hines M. Prenatal hormones and postnatal socialization by parents as determinants of male-typical toy play in girls with congenital adrenal hyperplasia. Child Dev. 2005;76:264–78. doi: 10.1111/j.1467-8624.2005.00843.x. [DOI] [PubMed] [Google Scholar]
- 32.Ehrhardt AA, Epstein R, Money J. Fetal androgens and female gender identity in the early treated adrenogenital syndrome. John Hopkins Med J. 1968;122:165–7. [PubMed] [Google Scholar]
- 33.Money J, Shwatrz M. Fetal androgens in the early treated adrenogenital syndrome of 46 XX hermaphroditism: Influence on aggressive and assertive types of behavior. Aggress Behav. 1976;2:19–30. [Google Scholar]
- 34.Laue L, Kenigsberg D, Pescovitz OH, Hench KD, Barnes KM, Loriaux DL, et al. Treatment of familial male precocious puberty with spironolactone and testolactone. N Engl J Med. 1989;320:496–502. doi: 10.1056/NEJM198902233200805. [DOI] [PubMed] [Google Scholar]
- 35.Leschek EW, Jones J, Barnes KM, Hill SC, Cutler GB., Jr Six-year results of spironolactone and testolactone treatment of familial male-limited precocious puberty with addition of deslorelin after central puberty onset. J Clin Endocrinol Metab. 1999;84:175–8. doi: 10.1210/jcem.84.1.5413. [DOI] [PubMed] [Google Scholar]
- 36.Kulshreshtha B, Marumudi E, Khurana ML, Kriplani A, Kinra G, Gupta DK, et al. Fertility among women with classical congenital adrenal hyperplasia: Report of seven cases where treatment was started after 9 years of age. Gynecol Endocrinol. 2008;24:267–72. doi: 10.1080/09513590801945230. [DOI] [PubMed] [Google Scholar]