

Abstract
INTRODUCTION
Spillage of calculi in the abdomen is frequent during Laparoscopic Cholecystectomy (LC). Though uncommon, these stones may lead to early or late complications. We describe a rare case of spilled gallstone presenting four years after the index procedure, with a mass in the parietal wall mimicking a neoplastic lesion.
PRESENTATION OF CASE
A 50 year old male presented with a mass in the right upper quadrant for the past 2 years. His past surgical history included a LC done four years ago. Intraoperative procedural details of the surgery were not available. A Computed Tomography (CT) scan showed an extrahepatic mass in the subdiaphragmatic space extending onto the soft tissues of the parietal wall. He underwent laparoscopic piecemeal excision of this organized mass. His post operative period was uneventful and he was pain-free on follow up.
DISCUSSION
Gallbladder perforation can occur due to excessive traction during retraction or during dissection from the liver bed. It can also occur during extraction from the abdomen. Infected bile, pigment gallstones, male gender, advanced age, perihepatic location of spilled gallstones, more than 15 gallstones and an average size greater than 1.5 cm have been identified as risk factors for complications. Definitive treatment is surgery with excision of the organized inflammatory mass and extraction of gallstones to avoid future recurrence.
CONCLUSION
Spilled gallstones can be a diagnostic challenge and can cause significant morbidity to the patient. Clear documentation of spillage and explanation to the patient is of utmost importance, as this will enable prompt recognition and treatment of any complications. Prevention of spillage is the best policy.
Keywords: Laparoscopic Cholecystectomy complication, Spilled gallstones, Inflammatory pseudotumour
1. Introduction
Gallbladder perforation with spillage of stones occur in 5–40% of patients undergoing Laparoscopic Cholecystectomy.1 The consequences of this spillage are innocuous and complications are rare.1,2 Even when they do occur, complications present in the early postoperative period. Long-term consequences of intra-peritoneal spillage gallstones are undefined.2 We describe a rare case of spilled gallstones four years after the index surgery presenting as a parietal wall pseudotumour, thereby creating a diagnostic conundrum.
2. Case report
A 50 year old otherwise healthy male presented with a minimally painful, slowly progressing mass in the right upper quadrant for the past 2 years. He denied any history of fever, chills, pain or gastrointestinal symptoms. His past surgical history included a Laparoscopic Cholecystectomy done for calculous cholecystitis four years ago. Intraoperative procedural details of the surgery were not available. On examination, he had a 6 cm × 5 cm firm to hard non tender immobile lump in right lower intercostal region along the anterior axillary line. This mass was away from any of the port-site scars (Fig. 1). Abdominal examination was unremarkable apart from healed port-site scars. His complete haemogram, renal function tests and liver function tests were within normal limits. A Computed Tomography (CT) scan showed a 10 cm × 5 cm organized extrahepatic mass in the subdiaphragmatic space extending onto the soft tissues of the parietal wall. There was a 0.5 cm × 0.5 cm calcific focus noted within the lesion (Fig. 2). He underwent laparoscopic piecemeal excision of this organized mass, there was 10 ml of purulent fluid within the lesion. The resected material contained calculous debris. Histopathology revealed inflammatory tissue consisting of a fibrous stroma and chronic inflammatory infiltrates with a predominance of plasma cells and an absence of dysplasia. His post operative period was uneventful and he was pain-free on follow up with no further increase in size of the parietal lesion.
Fig. 1.
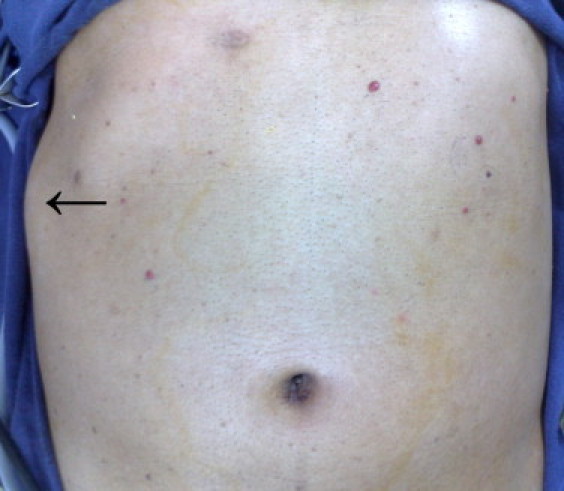
Parietal wall mass.
Fig. 2.
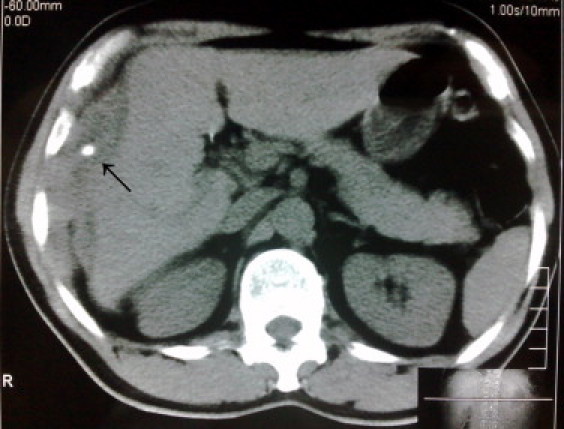
CT showing calcific focus in subdiaphragmatic space.
3. Discussion
Gallbladder perforation and spillage of gallstones into the peritoneal cavity are the most common complications during Laparoscopic Cholecystectomy.2–5 Gallstones are retained 1–13% of the time, and complications develop in 0.08–2.9% of cases.1–3,5,6 Difficulty in recovering all gallstones laparoscopically makes the rate of complications due to lost gallstones higher in Laparoscopic Cholecystectomy than in open Cholecystectomy.2–5 Spilled gallstones are the most frequently located in the right hypochondrium and the pelvis.5,6During Laparoscopic Cholecystectomy, there are three maneuvers that can result in a perforated gallbladder. First, is when the gallbladder is used for traction to assist in the dissection of the Calot's triangle. This exposes the gallbladder to excessive traction forces that may create a tear in the wall. The use of atraumatic graspers without teeth will decrease the incidence of tearing the gallbladder wall.2–6 Secondly, the gallbladder wall may be breached during its dissection from the liver bed.2–6 Finally, when the gallbladder is extracted from the abdomen through one of the ports, at this time it is put under high pressures.3–6 Perforation is easily avoided if an extension of the fascial incision is performed when needed. Removal of the gallbladder should be visualized with the scope to identify spillage when it occurs.5–7 The amount of inflammation present may also contribute to the rate of perforation. Inflammation could cause the gallbladder wall to be friable and more prone to tearing under the stress of traction.1,4–6 It may also cause it to be more difficult to define the plane between the liver and the gallbladder during dissection. If a perforation does occur, control of the rent with a pre-tied suture ligature, hemoclip, or grasper should be considered.1–8 When a tear is recognized, a suction cannula can be introduced into the gallbladder lumen through the tear for aspiration of the remaining contents.3,4,7 As many gallstones as possible should be removed, this can be achieved by the use of laparoscopic forceps, an intra-abdominal retrieval bag, a 10-mm suction device, or a “shuttle” gallstone collector.1–8 The abdomen should be irrigated copiously to dilute the spilled bile.4,5,7 These events should always be documented.1–8 The indication for converting to laparotomy in the event of gallstone spillage is a controversial subject. Most authors believe it is better to contain the spill, and retrieve the stones laparoscopically, especially since most patients will not develop a major complication from this event.1,4–7 Laparotomy is indicated only in selected cases of significant spillage of gallstones in which recovery of most of them has not been possible, especially when bile contamination is suspected.4–8 The role of perioperative antibiotics in prevention of postoperative abscess has not been defined, but probably has little effect.4,5 Late complications are less frequent, though the development of an intra-abdominal abscess has been reported.2,6 The diagnosis of complications due to spilled gallstones requires a high level of clinical suspicion. The operative record should be reviewed for report of stone spillage during the procedure, although this may not be accurate.4 The typical symptoms of intrabdominal spilled gallstones are pain and fever.4,7 The most frequent microorganisms in the cultures are Escherichia coli, Klebsiella pneumoniae, and Enterococcus faecalis.1,4–6 CT is most useful, as it is capable of depicting the extent of inflammatory process and the presence of calcifications consistent with gallstones.3 In cases where the gallstones are not radiopaque, the diagnosis may be confused with simple abscesses. Ultrasound is more specific in diagnosis, revealing a hyperechoic lesion with an acoustic shadow, regardless of whether there is calcification or not.5,7,8 Infected bile, pigment gallstones, male gender, advanced age, perihepatic location of spilled gallstones, more than 15 gallstones, and an average size greater than 1.5 cm have been identified as risk factors for complications.1–4 In some cases, intra-abdominal abscesses have been treated with antibiotic therapy. Drainage of the abscess and percutaneous extraction of the gallstone have been attempted, although the rate of failure and recurrence is high with these conservative methods of treatment.4–8 Definitive treatment is surgery with excision of the organized inflammatory mass and extraction of gallstones to avoid future recurrence.3–5 Laparoscopy helps to confirm the diagnosis and also to treat it in the same sitting. However, some patients may require laparotomy for complete removal of stones.1,3,4,6,8 Clear operative documentation and explanation to the patient are critical in avoiding future diagnostic confusion and therapeutic morbidity.1–8 Prevention of spillage is the best policy.1–8
Conflict of interest statement
None.
Funding
None.
Ethical approval
Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Author contributions
Dr. Ashwin Rammohan: Data Collection, Writing.
Dr. U.P. Srinivasan: Data Analysis, Writing.
Dr. S. Jeswanth: Data Analysis, Editing.
Dr. P. Ravichandran: Data Analysis, Editing
References
- 1.Castellón-Pavón C.J., Morales-Artero S., Martínez-Pozuelo A., Valderrábano-González S. Complications due to spilled gallstones and surgical clips during laparoscopic cholecystectomy. Cir Esp. 2008;84(1):3–9. doi: 10.1016/s0009-739x(08)70596-7. [DOI] [PubMed] [Google Scholar]
- 2.Rice D.C., Memon M.A., Jamison R.L., Agnessi T., Ilstrup D., Bannon M.B. Long-term consequences of intraoperative spillage of bile and gallstones during laparoscopic cholecystectomy. J Gastrointest Surg. 1997;1(1):85–91. doi: 10.1007/s11605-006-0014-x. [DOI] [PubMed] [Google Scholar]
- 3.Woodfield J.C., Rodgers M., Windsor J.A. Peritoneal gallstones following laparoscopic cholecystectomy. Surg Endosc. 2004;18(8):1200–1207. doi: 10.1007/s00464-003-8260-4. [DOI] [PubMed] [Google Scholar]
- 4.Schafer M., Suter C., Klaiber C., Wehrli H., Frei E., Krahenbuhl L. Spilled gallstones after laparoscopic cholecystectomy. A relevant problem? A retrospective analysis of 10,174 laparoscopic cholecystectomies. Surg Endosc. 1998;12:305–309. doi: 10.1007/s004649900659. [DOI] [PubMed] [Google Scholar]
- 5.Manukyan M.N., Demirkalem P., Gulluoglu B.M., Tuney D., Yegen C., Yalin R., Aktan A.O. Retained abdominal gallstones during laparoscopic cholecystectomy. Am J Surg. 2005;189:450–452. doi: 10.1016/j.amjsurg.2004.09.015. [DOI] [PubMed] [Google Scholar]
- 6.Horton M., Florence M.G. Unusual abscess patterns following dropped gallstones during laparoscopic cholecystectomy. Am J Surg. 1998;175(5):375–379. doi: 10.1016/S0002-9610(98)00048-8. [DOI] [PubMed] [Google Scholar]
- 7.Papasavas P., Caushaj P., Gagne D. Spilled gallstones after laparoscopic cholecystectomy. J Laparoendosc Adv Surg Tech. 2002;12(5):383–386. doi: 10.1089/109264202320884144. [DOI] [PubMed] [Google Scholar]
- 8.Brockmann J.G., Kocher T., Senninger N.J., Schurmann G.M. Complications due to gallstones lost during laparoscopic cholecystectomy. Surg Endosc. 2002;16(1):226–232. doi: 10.1007/s00464-001-9173-8. [DOI] [PubMed] [Google Scholar]