

Myositis ossificans (MO) is a rare condition characterized by bonelike deposits in muscles, especially in areas exposed to trauma or in devitalized tissues within the muscle or other soft tissues1. This ectopic bone formation is seen not only in children with MO, but also as a complication of several connective tissue disorders2. Studies of the chemical compositions of these calcifications have been limited because of lack of access to involved tissue. We had described the structure and composition of calcific deposits in 5 children with juvenile dermatomyositis (JDM) using Fourier transform infrared spectroscopic imaging (FTIRI)3. We hypothesized that although the mineral deposits in children with MO as well as in JDM were classified as dystrophic calcifications, the lesion in MO would have unique characteristics, but would be distinct from human trabecular bone.
Examination of the specimen of a 9-year-old girl with MO by FTIRI revealed that the only mineral present was a poorly crystalline hydroxyapatite (Figure 1). The mineral/matrix ratio and carbonate contents were lower in MO than in bone or JDM calcifications. The collagen crosslink ratio was greater in both bone and MO compared to JDM calcifications. The crystallinity was similar in both types of pediatric dystrophic calcifications and in adult bone. These data contradict the original report that the mineral in MO is a highly crystalline fluoro-apatite without any carbonate substitution4. Although the deposits in both JDM and MO are dystrophic, they each have unique characteristics on FTIRI.
Figure 1.
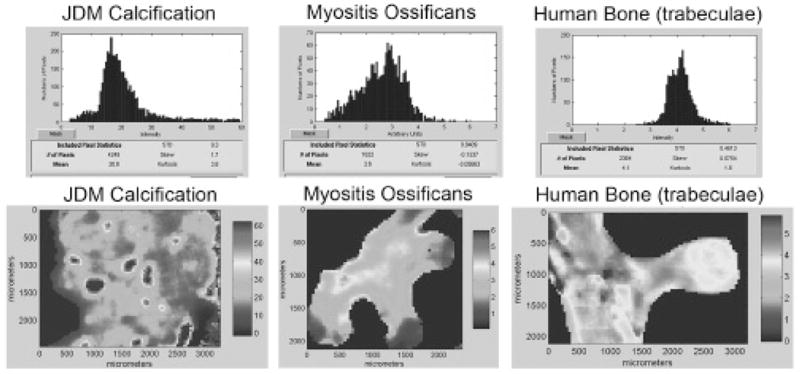
The mineral/matrix ratio of the myositis ossificans is more similar to that of human bone than to juvenile dermatomyositis, in which the ratio is much higher than that of either bone or myositis ossificans.
Acknowledgments
Supported by DE04141 and NIAMS AR046121 (to ALB) and CureJM Program of Excellence in Myositis Research and NIAMS R01 AR48289 (to LMP).
Contributor Information
MARIA IBARRA, Division of Rheumatology, The Children’s Memorial Hospital, Northwestern University, Feinberg School of Medicine, Chicago, Illinois.
PAULINE M. CHOU, Department of Pathology, The Children’s Memorial Hospital, Northwestern University, Feinberg School of Medicine, Chicago, Illinois.
LAUREN M. PACHMAN, Division of Rheumatology, The Children’s Memorial Hospital, Northwestern University, Feinberg School of Medicine, Chicago, Illinois.
YONG-DONG ZHAO, Cincinnati Children’s Hospital Medical Center, Department of Pediatrics, Cincinnati, Ohio.
ADELE L. BOSKEY, The Hospital for Special Surgery, Musculoskeletal Integrity Program, Weill Medical College of Cornell University, New York, New York, USA.
References
- 1.Vanden Bossche L, Vanderstraeten G. Heterotopic ossification: a review. J Rehabil Med. 2005;37:129–36. doi: 10.1080/16501970510027628. [DOI] [PubMed] [Google Scholar]
- 2.Boulman N, Slobodin G, Rozenbaum M, Rosner I. Calcinosis in rheumatic diseases. Semin Arthritis Rheum. 2005;34:805–12. doi: 10.1016/j.semarthrit.2005.01.016. [DOI] [PubMed] [Google Scholar]
- 3.Pachman LM, Veis A, Stock S, Abbott K, Vicari F, Patel P, et al. Composition of calcifications in children with juvenile dermatomyositis. Arthritis Rheum. 2006;54:3345–50. doi: 10.1002/art.22158. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Pinter J, Lenart G, Rishak G. Histological, physical and chemical investigation of myositis ossificans traumatica. Acta Orthop Scand. 1980;51:899–902. doi: 10.3109/17453678008990891. [DOI] [PubMed] [Google Scholar]